Bisset L, Beller E, Jull G, Brooks P, Darnell R, Vicenzino B. Mobilisation with movement and exercise, corticosteroid injection, or wait and see for tennis elbow: randomised trial. BMJ. 2006 Nov 4. 333(7575):939. [QxMD MEDLINE Link]. [Full Text].
Altan L, Kanat E. Conservative treatment of lateral epicondylitis: comparison of two different orthotic devices. Clin Rheumatol. 2008 Aug. 27(8):1015-9. [QxMD MEDLINE Link].
Jafarian FS, Demneh ES, Tyson SF. The immediate effect of orthotic management on grip strength of patients with lateral epicondylosis. J Orthop Sports Phys Ther. 2009 Jun. 39(6):484-9. [QxMD MEDLINE Link].
Roetert EP, Brody H, Dillman CJ, Groppel JL, Schultheis JM. The biomechanics of tennis elbow. An integrated approach. Clin Sports Med. 1995 Jan. 14(1):47-57. [QxMD MEDLINE Link].
Rossi J, Vigouroux L, Barla C, Berton E. Potential effects of racket grip size on lateral epicondilalgy risks. Scand J Med Sci Sports. 2014 Mar 20. [QxMD MEDLINE Link].
Li FX, Fewtrell D, Jenkins M. String vibration dampers do not reduce racket frame vibration transfer to the forearm. J Sports Sci. 2004 Nov-Dec. 22(11-12):1041-52. [QxMD MEDLINE Link].
Lebiedziński R, Synder M, Buchcic P, Polguj M, Grzegorzewski A, Sibiński M. A randomized study of autologous conditioned plasma and steroid injections in the treatment of lateral epicondylitis. Int Orthop. 2015 Nov. 39 (11):2199-203. [QxMD MEDLINE Link].
Herquelot E, Guéguen A, Roquelaure Y, Bodin J, Sérazin C, Ha C, et al. Work-related risk factors for incidence of lateral epicondylitis in a large working population. Scand J Work Environ Health. 2013 Nov. 39(6):578-88. [QxMD MEDLINE Link].
Lin CL, Lee JS, Su WR, Kuo LC, Tai TW, Jou IM. Clinical and ultrasonographic results of ultrasonographically guided percutaneous radiofrequency lesioning in the treatment of recalcitrant lateral epicondylitis. Am J Sports Med. 2011 Nov. 39 (11):2429-35. [QxMD MEDLINE Link].
Edwards SG, Calandruccio JH. Autologous blood injections for refractory lateral epicondylitis. J Hand Surg Am. 2003 Mar. 28(2):272-8. [QxMD MEDLINE Link].
Connell DA, Ali KE, Ahmad M, Lambert S, Corbett S, Curtis M. Ultrasound-guided autologous blood injection for tennis elbow. Skeletal Radiol. 2006 Jun. 35(6):371-7. [QxMD MEDLINE Link].
Wolf JM, Ozer K, Scott F, Gordon MJ, Williams AE. Comparison of autologous blood, corticosteroid, and saline injection in the treatment of lateral epicondylitis: a prospective, randomized, controlled multicenter study. J Hand Surg Am. 2011 Aug. 36(8):1269-72. [QxMD MEDLINE Link].
Pattanittum P, Turner T, Green S, Buchbinder R. Non-steroidal anti-inflammatory drugs (NSAIDs) for treating lateral elbow pain in adults. Cochrane Database Syst Rev. 2013. 5:CD003686. [QxMD MEDLINE Link].
Nilsson P, Baigi A, Swärd L, Möller M, Månsson J. Lateral epicondylalgia: a structured programme better than corticosteroids and NSAID. Scand J Occup Ther. 2012 Sep. 19(5):404-10. [QxMD MEDLINE Link].
Kazemi M, Azma K, Tavana B, Rezaiee Moghaddam F, Panahi A. Autologous blood versus corticosteroid local injection in the short-term treatment of lateral elbow tendinopathy: a randomized clinical trial of efficacy. Am J Phys Med Rehabil. 2010 Aug. 89(8):660-7. [QxMD MEDLINE Link].
Thanasas C, Papadimitriou G, Charalambidis C, Paraskevopoulos I, Papanikolaou A. Platelet-rich plasma versus autologous whole blood for the treatment of chronic lateral elbow epicondylitis: a randomized controlled clinical trial. Am J Sports Med. 2011 Oct. 39 (10):2130-4. [QxMD MEDLINE Link].
Altan L, Kanat E. Conservative treatment of lateral epicondylitis: comparison of two different orthotic devices. Clin Rheumatol. 2008 Aug. 27 (8):1015-9. [QxMD MEDLINE Link].
Borkholder CD, Hill VA, Fess EE. The efficacy of splinting for lateral epicondylitis: a systematic review. J Hand Ther. 2004 Apr-Jun. 17(2):181-99. [QxMD MEDLINE Link].
Bisset L, Paungmali A, Vicenzino B, Beller E. A systematic review and meta-analysis of clinical trials on physical interventions for lateral epicondylalgia. Br J Sports Med. 2005 Jul. 39(7):411-22; discussion 411-22. [QxMD MEDLINE Link].
Jafarian FS, Demneh ES, Tyson SF. The immediate effect of orthotic management on grip strength of patients with lateral epicondylosis. J Orthop Sports Phys Ther. 2009 Jun. 39(6):484-9. [QxMD MEDLINE Link].
Garg R, Adamson GJ, Dawson PA, Shankwiler JA, Pink MM. A prospective randomized study comparing a forearm strap brace versus a wrist splint for the treatment of lateral epicondylitis. J Shoulder Elbow Surg. 2010 Jun. 19(4):508-12. [QxMD MEDLINE Link].
Najafi M, Arazpour M, Aminian G, Curran S, Madani SP, Hutchins SW. Effect of a new hand-forearm splint on grip strength, pain, and function in patients with tennis elbow. Prosthet Orthot Int. 2016 Jun. 40 (3):363-8. [QxMD MEDLINE Link].
Saremi H, Chamani V, Vahab-Kashani R. A Newly Designed Tennis Elbow Orthosis With a Traditional Tennis Elbow Strap in Patients With Lateral Epicondylitis. Trauma Mon. 2016 Jul. 21 (3):e35993. [QxMD MEDLINE Link].
Buchbinder R, Green SE, Youd JM, et al. Shock wave therapy for lateral elbow pain. Cochrane Database Syst Rev. 2005 Oct 19. CD003524. [QxMD MEDLINE Link].
Aydın A, Atiç R. Comparison of extracorporeal shock-wave therapy and wrist-extensor splint application in the treatment of lateral epicondylitis: a prospective randomized controlled study. J Pain Res. 2018. 11:1459-1467. [QxMD MEDLINE Link].
Notarnicola A, Quagliarella L, Sasanelli N, Maccagnano G, Fracella MR, Forcignanò MI, et al. Effects of extracorporeal shock wave therapy on functional and strength recovery of handgrip in patients affected by epicondylitis. Ultrasound Med Biol. 2014 Dec. 40 (12):2830-40. [QxMD MEDLINE Link].
Bayram K, Yesil H, Dogan E. Efficacy of extracorporeal shock wave therapy in the treatment of lateral epicondylitis. North Clin Istanb. 2014. 1 (1):33-38. [QxMD MEDLINE Link].
Köksal İ, Güler O, Mahiroğulları M, Mutlu S, Çakmak S, Akşahin E. Comparison of extracorporeal shock wave therapy in acute and chronic lateral epicondylitis. Acta Orthop Traumatol Turc. 2015. 49 (5):465-70. [QxMD MEDLINE Link].
Lizis P. Analgesic effect of extracorporeal shock wave therapy versus ultrasound therapy in chronic tennis elbow. J Phys Ther Sci. 2015 Aug. 27 (8):2563-7. [QxMD MEDLINE Link].
Trentini R, Mangano T, Repetto I, Cerruti P, Kuqi E, Trompetto C, et al. Short- to mid-term follow-up effectiveness of US-guided focal extracorporeal shock wave therapy in the treatment of elbow lateral epicondylitis. Musculoskelet Surg. 2015 Sep. 99 Suppl 1:S91-7. [QxMD MEDLINE Link].
Beyazal MS, Devrimsel G. Comparison of the effectiveness of local corticosteroid injection and extracorporeal shock wave therapy in patients with lateral epicondylitis. J Phys Ther Sci. 2015 Dec. 27 (12):3755-8. [QxMD MEDLINE Link].
Ramsay DJ, Bowman MA, Greenman, PE, et al, for the NIH Consensus Panel. NIH Consensus Conference. Acupuncture. JAMA. 1998 Nov 4. 280(17):1518-24. [QxMD MEDLINE Link].
Li X, Zhou K, Zhang E, Qi Z, Sun W, Xu L, et al. Therapeutic effect of electroacupuncture, massage, and blocking therapy on external humeral epicondylitis. J Tradit Chin Med. 2014 Jun. 34 (3):261-6. [QxMD MEDLINE Link].
Wong CW, Ng EY, Fung PW, Mok KM, Yung PS, Chan KM. Comparison of treatment effects on lateral epicondylitis between acupuncture and extracorporeal shockwave therapy. Asia Pac J Sports Med Arthrosc Rehabil Technol. 2017 Jan. 7:21-26. [QxMD MEDLINE Link].
Calandruccio JH, Steiner MM. Autologous Blood and Platelet-Rich Plasma Injections for Treatment of Lateral Epicondylitis. Orthop Clin North Am. 2017 Jul. 48 (3):351-357. [QxMD MEDLINE Link].
Edwards SG, Calandruccio JH. Autologous blood injections for refractory lateral epicondylitis. J Hand Surg [Am]. 2003 Mar. 28(2):272-8. [QxMD MEDLINE Link].
Ozturan KE, Yucel I, Cakici H, Guven M, Sungur I. Autologous blood and corticosteroid injection and extracoporeal shock wave therapy in the treatment of lateral epicondylitis. Orthopedics. 2010 Feb. 33(2):84-91. [QxMD MEDLINE Link].
Kazemi M, Azma K, Tavana B, Rezaiee Moghaddam F, Panahi A. Autologous blood versus corticosteroid local injection in the short-term treatment of lateral elbow tendinopathy: a randomized clinical trial of efficacy. Am J Phys Med Rehabil. 2010 Aug. 89(8):660-7. [QxMD MEDLINE Link].
Karimi Mobarakeh M, Nemati A, Fazli A, Fallahi A, Safari S. Autologous blood injection for treatment of tennis elbow. Trauma Mon. 2013 Winter. 17(4):393-5. [QxMD MEDLINE Link]. [Full Text].
Bostan B, Balta O, Aşçı M, Aytekin K, Eser E. Autologous Blood Injection Works for Recalcitrant Lateral Epicondylitis. Balkan Med J. 2016 Mar. 33 (2):216-20. [QxMD MEDLINE Link].
Arik HO, Kose O, Guler F, Deniz G, Egerci OF, Ucar M. Injection of autologous blood versus corticosteroid for lateral epicondylitis: a randomised controlled study. J Orthop Surg (Hong Kong). 2014 Dec. 22 (3):333-7. [QxMD MEDLINE Link].
Chen X, Jones IA, Park C, Vangsness CT Jr. The Efficacy of Platelet-Rich Plasma on Tendon and Ligament Healing: A Systematic Review and Meta-analysis With Bias Assessment. Am J Sports Med. 2018 Jul. 46 (8):2020-2032. [QxMD MEDLINE Link].
Mishra A, Pavelko T. Treatment of chronic elbow tendinosis with buffered platelet-rich plasma. Am J Sports Med. 2006 Nov. 34(11):1774-8. [QxMD MEDLINE Link].
Creaney L, Wallace A, Curtis M, Connell D. Growth factor-based therapies provide additional benefit beyond physical therapy in resistant elbow tendinopathy: a prospective, single-blind, randomised trial of autologous blood injections versus platelet-rich plasma injections. Br J Sports Med. 2011 Sep. 45(12):966-71. [QxMD MEDLINE Link].
Raeissadat SA, Sedighipour L, Rayegani SM, Bahrami MH, Bayat M, Rahimi R. Effect of Platelet-Rich Plasma (PRP) versus Autologous Whole Blood on Pain and Function Improvement in Tennis Elbow: A Randomized Clinical Trial. Pain Res Treat. 2014. 2014:191525. [QxMD MEDLINE Link]. [Full Text].
Raeissadat SA, Sedighipour L, Rayegani SM, Bahrami MH, Bayat M, Rahimi R. Effect of Platelet-Rich Plasma (PRP) versus Autologous Whole Blood on Pain and Function Improvement in Tennis Elbow: A Randomized Clinical Trial. Pain Res Treat. 2014. 2014:191525. [QxMD MEDLINE Link].
Raeissadat SA, Rayegani SM, Hassanabadi H, Rahimi R, Sedighipour L, Rostami K. Is Platelet-rich plasma superior to whole blood in the management of chronic tennis elbow: one year randomized clinical trial. BMC Sports Sci Med Rehabil. 2014. 6:12. [QxMD MEDLINE Link].
Krogh TP, Fredberg U, Stengaard-Pedersen K, Christensen R, Jensen P, Ellingsen T. Treatment of lateral epicondylitis with platelet-rich plasma, glucocorticoid, or saline: a randomized, double-blind, placebo-controlled trial. Am J Sports Med. 2013 Mar. 41(3):625-35. [QxMD MEDLINE Link].
Yadav R, Kothari SY, Borah D. Comparison of Local Injection of Platelet Rich Plasma and Corticosteroids in the Treatment of Lateral Epicondylitis of Humerus. J Clin Diagn Res. 2015 Jul. 9 (7):RC05-7. [QxMD MEDLINE Link].
Gautam VK, Verma S, Batra S, Bhatnagar N, Arora S. Platelet-rich plasma versus corticosteroid injection for recalcitrant lateral epicondylitis: clinical and ultrasonographic evaluation. J Orthop Surg (Hong Kong). 2015 Apr. 23 (1):1-5. [QxMD MEDLINE Link].
Behera P, Dhillon M, Aggarwal S, Marwaha N, Prakash M. Leukocyte-poor platelet-rich plasma versus bupivacaine for recalcitrant lateral epicondylar tendinopathy. J Orthop Surg (Hong Kong). 2015 Apr. 23 (1):6-10. [QxMD MEDLINE Link].
Mishra AK, Skrepnik NV, Edwards SG, Jones GL, Sampson S, Vermillion DA, et al. Efficacy of platelet-rich plasma for chronic tennis elbow: a double-blind, prospective, multicenter, randomized controlled trial of 230 patients. Am J Sports Med. 2014 Feb. 42(2):463-71. [QxMD MEDLINE Link].
Arirachakaran A, Sukthuayat A, Sisayanarane T, Laoratanavoraphong S, Kanchanatawan W, Kongtharvonskul J. Platelet-rich plasma versus autologous blood versus steroid injection in lateral epicondylitis: systematic review and network meta-analysis. J Orthop Traumatol. 2016 Jun. 17 (2):101-12. [QxMD MEDLINE Link].
Chou LC, Liou TH, Kuan YC, Huang YH, Chen HC. Autologous blood injection for treatment of lateral epicondylosis: A meta-analysis of randomized controlled trials. Phys Ther Sport. 2016 Mar. 18:68-73. [QxMD MEDLINE Link].
Montalvan B, Le Goux P, Klouche S, Borgel D, Hardy P, Breban M. Inefficacy of ultrasound-guided local injections of autologous conditioned plasma for recent epicondylitis: results of a double-blind placebo-controlled randomized clinical trial with one-year follow-up. Rheumatology (Oxford). 2016 Feb. 55 (2):279-85. [QxMD MEDLINE Link].
Tonk G, Kumar A, Gupta A. Platelet rich plasma versus laser therapy in lateral epicondylitis of elbow. Indian J Orthop. 2014 Jul. 48 (4):390-3. [QxMD MEDLINE Link].
Tetschke E, Rudolf M, Lohmann CH, Stärke C. Autologous proliferative therapies in recalcitrant lateral epicondylitis. Am J Phys Med Rehabil. 2015 Sep. 94 (9):696-706. [QxMD MEDLINE Link].
Karaduman M, Okkaoglu MC, Sesen H, Taskesen A, Ozdemir M, Altay M. Platelet-rich plasma versus open surgical release in chronic tennis elbow: A retrospective comparative study. J Orthop. 2016 Mar. 13 (1):10-4. [QxMD MEDLINE Link].
Petrella RJ, Cogliano A, Decaria J, Mohamed N, Lee R. Management of Tennis Elbow with sodium hyaluronate periarticular injections. Sports Med Arthrosc Rehabil Ther Technol. 2010 Feb 2. 2:4. [QxMD MEDLINE Link]. [Full Text].
Kumai T, Muneta T, Tsuchiya A, Shiraishi M, Ishizaki Y, Sugimoto K, et al. The short-term effect after a single injection of high-molecular-weight hyaluronic acid in patients with enthesopathies (lateral epicondylitis, patellar tendinopathy, insertional Achilles tendinopathy, and plantar fasciitis): a preliminary study. J Orthop Sci. 2014 Jul. 19 (4):603-11. [QxMD MEDLINE Link].
Zeisig E, Fahlström M, Ohberg L, Alfredson H. Pain relief after intratendinous injections in patients with tennis elbow: results of a randomised study. Br J Sports Med. 2008 Apr. 42(4):267-71. [QxMD MEDLINE Link].
Branson R, Naidu K, du Toit C, Rotstein AH, Kiss R, McMillan D, et al. Comparison of corticosteroid, autologous blood or sclerosant injections for chronic tennis elbow. J Sci Med Sport. 2017 Jun. 20 (6):528-533. [QxMD MEDLINE Link].
Wong SM, Hui AC, Tong PY, et al. Treatment of lateral epicondylitis with botulinum toxin: a randomized, double-blind, placebo-controlled trial. Ann Intern Med. 2005 Dec 6. 143(11):793-7. [QxMD MEDLINE Link]. [Full Text].
Placzek R, Drescher W, Deuretzbacher G, Hempfing A, Meiss AL. Treatment of chronic radial epicondylitis with botulinum toxin A. A double-blind, placebo-controlled, randomized multicenter study. J Bone Joint Surg Am. 2007 Feb. 89(2):255-60. [QxMD MEDLINE Link].
Hayton MJ, Santini AJ, Hughes PJ, et al. Botulinum toxin injection in the treatment of tennis elbow. A double-blind, randomized, controlled, pilot study. J Bone Joint Surg Am. 2005 Mar. 87(3):503-7. [QxMD MEDLINE Link].
Guo YH, Kuan TS, Chen KL, Lien WC, Hsieh PC, Hsieh IC, et al. Comparison Between Steroid and 2 Different Sites of Botulinum Toxin Injection in the Treatment of Lateral Epicondylalgia: A Randomized, Double-Blind, Active Drug-Controlled Pilot Study. Arch Phys Med Rehabil. 2017 Jan. 98 (1):36-42. [QxMD MEDLINE Link].
Creuzé A, Petit H, de Sèze M. Short-Term Effect of Low-Dose, Electromyography-Guided Botulinum Toxin A Injection in the Treatment of Chronic Lateral Epicondylar Tendinopathy: A Randomized, Double-Blinded Study. J Bone Joint Surg Am. 2018 May 16. 100 (10):818-826. [QxMD MEDLINE Link].
Lin YC, Tu YK, Chen SS, Lin IL, Chen SC, Guo HR. Comparison between botulinum toxin and corticosteroid injection in the treatment of acute and subacute tennis elbow: a prospective, randomized, double-blind, active drug-controlled pilot study. Am J Phys Med Rehabil. 2010 Aug. 89 (8):653-9. [QxMD MEDLINE Link].
Paoloni JA, Appleyard RC, Nelson J, Murrell GA. Topical nitric oxide application in the treatment of chronic extensor tendinosis at the elbow: a randomized, double-blinded, placebo-controlled clinical trial. Am J Sports Med. 2003 Nov-Dec. 31(6):915-20. [QxMD MEDLINE Link].
Ozden R, Uruç V, Doğramaci Y, Kalaci A, Yengil E. Management of tennis elbow with topical glyceryl trinitrate. Acta Orthop Traumatol Turc. 2014. 48 (2):175-80. [QxMD MEDLINE Link].
Singh A, Gangwar DS, Singh S. Bone marrow injection: A novel treatment for tennis elbow. J Nat Sci Biol Med. 2014 Jul. 5 (2):389-91. [QxMD MEDLINE Link].
Wang A, Breidahl W, Mackie KE, Lin Z, Qin A, Chen J, et al. Autologous tenocyte injection for the treatment of severe, chronic resistant lateral epicondylitis: a pilot study. Am J Sports Med. 2013 Dec. 41 (12):2925-32. [QxMD MEDLINE Link].
Wang A, Mackie K, Breidahl W, Wang T, Zheng MH. Evidence for the Durability of Autologous Tenocyte Injection for Treatment of Chronic Resistant Lateral Epicondylitis: Mean 4.5-Year Clinical Follow-up. Am J Sports Med. 2015 Jul. 43 (7):1775-83. [QxMD MEDLINE Link].
Lee SY, Kim W, Lim C, Chung SG. Treatment of Lateral Epicondylosis by Using Allogeneic Adipose-Derived Mesenchymal Stem Cells: A Pilot Study. Stem Cells. 2015 Oct. 33 (10):2995-3005. [QxMD MEDLINE Link].
Barnes DE, Beckley JM, Smith J. Percutaneous ultrasonic tenotomy for chronic elbow tendinosis: a prospective study. J Shoulder Elbow Surg. 2015 Jan. 24 (1):67-73. [QxMD MEDLINE Link].
Chesterton LS, Lewis AM, Sim J, Mallen CD, Mason EE, Hay EM, et al. Transcutaneous electrical nerve stimulation as adjunct to primary care management for tennis elbow: pragmatic randomised controlled trial (TATE trial). Br J Sports Med. 2014 Oct. 48 (19):1458. [QxMD MEDLINE Link].
Smidt N, Assendelft WJ, Arola H, et al. Effectiveness of physiotherapy for lateral epicondylitis: a systematic review. Ann Med. 2003. 35(1):51-62. [QxMD MEDLINE Link].
Dundar U, Turkmen U, Toktas H, Ulasli AM, Solak O. Effectiveness of high-intensity laser therapy and splinting in lateral epicondylitis; a prospective, randomized, controlled study. Lasers Med Sci. 2015 Apr. 30 (3):1097-107. [QxMD MEDLINE Link].
Salli A, Akkurt E, Izki AA, Şen Z, Yilmaz H. Comparison of High Intensity Laser and Epicondylitis Bandage in the Treatment of Lateral Epicondylitis. Arch Rheumatol. 2016 Sep. 31 (3):234-238. [QxMD MEDLINE Link].
Akkurt E, Kucuksen S, Yılmaz H, Parlak S, Sallı A, Karaca G. Long term effects of high intensity laser therapy in lateral epicondylitis patients. Lasers Med Sci. 2016 Feb. 31 (2):249-53. [QxMD MEDLINE Link].
Brosseau L, Casimiro L, Milne S, et al. Deep transverse friction massage for treating tendinitis. Cochrane Database Syst Rev. 2002. CD003528. [QxMD MEDLINE Link].
Sevier TL, Stegink-Jansen CW. Astym treatment vs. eccentric exercise for lateral elbow tendinopathy: a randomized controlled clinical trial. PeerJ. 2015. 3:e967. [QxMD MEDLINE Link].
Baker CL Jr, Baker CL 3rd. Long-term follow-up of arthroscopic treatment of lateral epicondylitis. Am J Sports Med. 2008 Feb. 36(2):254-60. [QxMD MEDLINE Link].
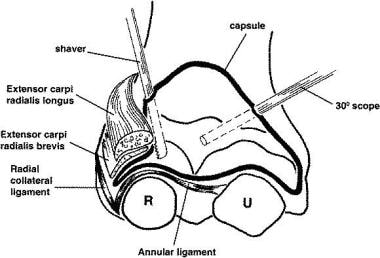 Representation of the relationships in arthroscopic release for lateral epicondylitis.
Representation of the relationships in arthroscopic release for lateral epicondylitis.



