Practice Essentials
Iliotibial band (ITB) syndrome (ITBS) is the most common cause of lateral knee pain among athletes. [1, 2, 3, 4, 5, 6, 7, 8] ITBS develops as a result of inflammation of the bursa surrounding the ITB and usually affects athletes who are involved in sports that require continuous running or repetitive knee flexion and extension. [3, 4, 5, 9, 10, 11, 12] This condition is, therefore, most common in long-distance runners and cyclists. ITBS may also be observed in athletes who participate in volleyball, tennis, soccer, football, skiing, weight lifting, and aerobics. [13]
The image below illustrates active stretching of the ITB.
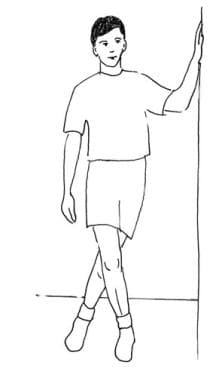 This illustration demonstrates active stretching of the iliotibial band (ITB). The athlete stands a comfortable distance from a wall and, with the contralateral knee extended, leans the proximal shoulder against the wall to stretch the ipsilateral ITB.
This illustration demonstrates active stretching of the iliotibial band (ITB). The athlete stands a comfortable distance from a wall and, with the contralateral knee extended, leans the proximal shoulder against the wall to stretch the ipsilateral ITB.
Signs and symptoms
The usual clinical history describes lateral knee pain.
Physical examination findings in patients with ITBS may include the following:
-
Abnormal gait
-
Point tenderness noted upon palpation of the lateral femoral epicondyle, as well as with palpation of a site 2-4 cm above the lateral joint line and at the Gerdy tubercle
-
Reproducible pain
See Presentation for more detail.
Diagnosis
Initially, radiographic studies are not indicated if the working diagnosis is completely consistent with ITBS. Radiographs are almost always negative.
See Workup for more detail.
Management
Modalities to decrease inflammation include ultrasonography, phonophoresis, iontophoresis, and icing. After the acute inflammation has resolved, the patient should begin a stretching program.
Surgical intervention is not indicated for ITBS except in rare cases.
See Treatment and Medication for more detail.
See also Medscape Drugs & Diseases articles Iliotibial Band Friction Syndrome and Physical Medicine and Rehabilitation for Iliotibial Band Syndrome.
Etiology
Runners
The posterior edge of the ITB impinges against the lateral epicondyle of the femur just after foot strike in the gait cycle. This friction occurs at or slightly below 30 º of knee flexion. Downhill running and running at slower speeds may exacerbate ITBS because the knee tends to be less flexed at foot strike.
Running on hard surfaces and banked surfaces: The injured leg is often the downside leg on a banked or crowned road.
Worn out or improper running shoes
Lower limb and foot misalignment such as valgus or varus alignment of the leg or leg-length discrepancy
Cyclists
In cycling, the ITB is pulled anteriorly on the pedaling downstroke and posteriorly on the upstroke. The ITB is predisposed to friction, irritation, and microtrauma during this repetitive movement because its posterior fibers adhere closely to the lateral femoral epicondyle.
Cyclists with an external tibia rotation greater than 20 º: Stress is created on the ITB if the athlete's cycling shoe is placed in a straight-ahead position or the toe is in a cleat position.
Cyclists with varus knee alignment or active pronation place a greater stretch on the distal ITB when they ride with internally rotated cleats.
Poorly fitted bicycle saddle: A high-riding saddle causes the cyclist to extend the knee more than 150 º. This exaggerated knee extension causes the distal ITB to abrade across the lateral femoral condyle. Bicycle saddles that are positioned too far back cause the cyclist to reach for the pedal, with a resultant stretch to the ITB.
All athletes
Improper warm-up and stretching
Increasing the quality and quantity of training sessions too quickly
Lower limb and foot misalignment such as valgus or varus alignment of the leg or leg-length discrepancy
Worn out or improper athletic shoes
On occasion, a contusion to the knee may precipitate ITBS.
Epidemiology
United States statistics
ITBS is the most common cause of lateral knee pain in runners. Although few studies are available regarding the incidence of ITBS in athletes, some studies cite this condition with an incidence as high as 12% of all running-related injuries. [14] Several studies of US Marine Corps recruits undergoing basic training determined the incidence of ITBS among this group to vary from 5.3 to 22.2%.
International statistics
In a Central European study of injuries related to running (N = 178), ITBS accounted for 12.3% of the injuries. [15]
Functional Anatomy
The ITB is the condensation of fascia formed by the tensor fascia lata and the gluteus medius and minimus muscles. The ITB is a wide, flat structure that originates at the iliac crest and inserts at the Gerdy tubercle on the lateral aspect of the proximal tibia. This band serves as a ligament between the lateral femoral condyle and the lateral tibia to stabilize the knee. The ITB assists in the following 4 movements of the lower extremity:
-
Abducts the hip
-
Contributes to internal rotation of the hip when the hip is flexed to 30°
-
Assists with knee extension when the knee is in less than 30° of flexion
-
Assists with knee flexion when the knee is in greater than 30° of flexion
The ITB is not attached to bone as it courses between the Gerdy tubercle and the lateral femoral epicondyle. This lack of attachment allows it to move anteriorly and posteriorly with knee flexion and extension. Some authors hypothesize that this movement may cause the ITB to rub against the lateral femoral condyle, causing inflammation. Other investigators hypothesize that injury of the ITB results from compression of the band against a layer of innervated fat between the ITB and epicondyle. Furthermore, a potential deep space is located under the ITB as it crosses the lateral femoral epicondyle and travels to the Gerdy tubercle. This bursa may become inflamed and cause a clicking sensation as the knee flexes and extends. The inflamed bursa may add another component to ITB tendinitis.
See also Medscape Drugs & Diseases topics Bursitis and Tendonitis.
Sport-Specific Biomechanics
In runners, the posterior edge of the ITB impinges against the lateral epicondyle of the femur just after foot strike in the gait cycle. [9, 10, 16, 17] This friction occurs at or slightly below 30 º of knee flexion. [4, 5, 9] Downhill running and running at slower speeds may exacerbate ITBS as the knee tends to be less flexed at foot strike. [18, 19]
In cyclists, the ITB is pulled anteriorly on the pedaling downstroke and posteriorly on the upstroke. The ITB is predisposed to friction, irritation, and microtrauma during this repetitive movement because its posterior fibers adhere closely to the lateral femoral epicondyle.
Prognosis
The prognosis for ITBS is excellent if the athlete maintains ITB flexibility and corrects the intrinsic factors that lead to this injury. The athlete must also avoid the extrinsic factors that provoke ITBS.
Complications
If the injury has not been fully rehabilitated before the athlete returns to play, ITBS can become a chronic condition.
Patient Education
Provide the athlete with educational materials that describe ITBS and its management. An individualized, written training program must be developed for each athlete through collaboration with the athlete and a physician, physical therapist, or athletic trainer.
-
The Ober test.
-
This illustration demonstrates active stretching of the iliotibial band (ITB). The athlete stands a comfortable distance from a wall and, with the contralateral knee extended, leans the proximal shoulder against the wall to stretch the ipsilateral ITB.
-
This illustration demonstrates iliotibial band syndrome stretching that is performed in a side-lying position.



