Practice Essentials
A bone island, also known as an enostosis, is a focus of compact bone located in cancellous bone (see the images below). [1, 2] This benign entity is usually found incidentally on imaging studies; however, the bone island may mimic a more sinister process, such as an osteoblastic metastasis (eg, from prostate cancer). [3] Bone islands demonstrate characteristic radiographic findings. In the correct clinical context, findings on radiographs are considered diagnostic. However, if the lesion is large or shows increased scintigraphic activity, or if the patient is symptomatic or has a history of malignancy, clinical follow-up and/or biopsy may be warranted. [3, 4]
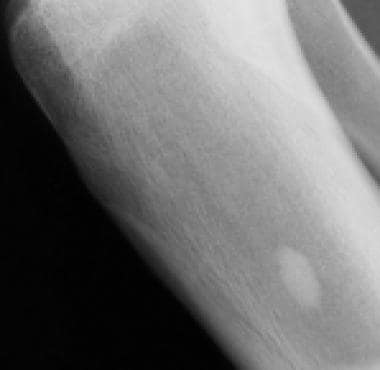 Plain-film radiograph of a bone island. Bone islands typically appear as sclerotic, round-to-ovoid intramedullary foci. The long axis of the bone island is aligned parallel to the long axis of the bone.
Plain-film radiograph of a bone island. Bone islands typically appear as sclerotic, round-to-ovoid intramedullary foci. The long axis of the bone island is aligned parallel to the long axis of the bone.
 T1- weighted, sagittal magnetic resonance imaging (MRI) scan of the knee. Because bone islands are composed of cortical bone, they demonstrate low signal intensity on MRI scans.
T1- weighted, sagittal magnetic resonance imaging (MRI) scan of the knee. Because bone islands are composed of cortical bone, they demonstrate low signal intensity on MRI scans.
Benign bone lesions may be incidentally detected on radiographs and are increasingly found on computed tomography (CT) or magnetic resonance imaging (MRI) performed for other clinical indications. Although they are most often asymptomatic or associated with minor symptoms, these lesions may simulate true pathologic lesions. Recognizing these entities as do-not-touch lesions helps avoid unnecessary further investigation or harmful intervention. [5]
Gould et al provided an in-depth review of 13 cases of bone tumor mimic (ie, a benign osseous lesion that radiologically resembles a bone tumor) and noted that this is not an uncommon finding. They reported that diagnosis and management of such lesions require knowledge of their epidemiology, clinical presentation, anatomy, and imaging features. [3]
Achong reported on a case of increased uptake of radionuclide in a bone island of the lumbar vertebral body; increased uptake was seen on single-photon emission computed tomography (SPECT) imaging but not on conventional planar imaging. [6]
Osteopoikilosis
Osteopoikilosis, a skeletal dysplasia, manifests radiographically as multiple bone islands that typically are situated in a periarticular distribution in the epiphyses (and often the metaphyses) of long and short tubular bones, as well as in the pelvis and scapulae (see the image below). [7] The distribution is typically bilateral and symmetric. The ribs, clavicles, spine, and skull are rarely involved. [8, 9, 10]
 Osteopoikilosis. A plain film radiographic image of the knee demonstrates numerous bone islands in a peri-articular distribution that is characteristic of osteopoikilosis.
Osteopoikilosis. A plain film radiographic image of the knee demonstrates numerous bone islands in a peri-articular distribution that is characteristic of osteopoikilosis.
The process usually does not result in symptoms or abnormal laboratory values, although associations with mild arthralgias and/or dermatologic manifestations have been reported. Osteopoikilosis is frequently associated with other bone dysplasias; when this occurs, the disorder is designated “overlap syndrome.” [7] As with solitary bone islands, the multiple bone islands of osteopoikilosis typically are not apparent on bone scintigraphy studies and can usually be distinguished from multifocal osteoblastic metastases (see the images below). [11, 12, 13, 14] Rare cases of misdiagnosis of this benign condition mimicking sclerotic bone metastasis have been described.
 Osteopoikilosis. A plain film radiograph of the pelvis with numerous bone islands that are characteristic of osteopoikilosis
Osteopoikilosis. A plain film radiograph of the pelvis with numerous bone islands that are characteristic of osteopoikilosis
 Osteopoikilosis. A whole body bone scan for the radiograph of the same patient as in the previous image does not demonstrate increased scintigraphic activity. Osteopoikilosis typically does not appear "hot" on bone scans.
Osteopoikilosis. A whole body bone scan for the radiograph of the same patient as in the previous image does not demonstrate increased scintigraphic activity. Osteopoikilosis typically does not appear "hot" on bone scans.
Radiography
The radiographic appearance of a bone island is well described in the literature. [15] Bone islands are round or ovoid, intramedullary, sclerotic foci that do not extend beyond the cortex. The long axis of a bone island typically parallels the long axis of the involved bone. Bone islands appear homogeneously sclerotic, with "thorny" radiating bone spicules that extend from the center of the lesion and blend with the trabeculae (see the image below). [1]
 Plain film radiograph of the hip. The right iliac bone demonstrates a bone island with "thorny" radiations that merge with the surrounding trabeculae.
Plain film radiograph of the hip. The right iliac bone demonstrates a bone island with "thorny" radiations that merge with the surrounding trabeculae.
Bone islands usually are 1 mm to 2 cm in diameter, with size typically remaining stable. However, reports have described bone islands that have increased or decreased in size; complete disappearance has also been reported. They can be found at any osseous site, with the pelvis and long bones (especially the proximal femur) most commonly involved. Other involved sites include the ribs, the carpal and tarsal bones, and the thoracolumbar vertebral bodies.
When bone islands are larger than 2 cm, they are classified as giant bone islands. [16, 17, 18, 19] With the exception of size, giant bone islands demonstrate the same radiographic features that smaller ones do. Giant bone islands most commonly are found in the pelvis; islands of up to 10 cm have been reported. [20]
Computed Tomography
Bone islands demonstrate CT scan findings that correlate with their plain film appearance. They are sclerotic and hyperdense foci with "thorny" radiations that blend with surrounding trabeculae (see the images below). [1, 21]
 Plain film radiograph of the pelvis. A sclerotic focus that is compatible with a bone island is seen in the right iliac bone adjacent to the sacroiliac joint. Bone islands typically are 1 mm to 2 cm in diameter.
Plain film radiograph of the pelvis. A sclerotic focus that is compatible with a bone island is seen in the right iliac bone adjacent to the sacroiliac joint. Bone islands typically are 1 mm to 2 cm in diameter.
 Computed tomography (CT) scan. A sclerotic focus that correlates with the radiograph in the previous image is seen in the right iliac bone adjacent to the sacroiliac joint. CT scan findings of bone islands correlate with their plain film appearance.
Computed tomography (CT) scan. A sclerotic focus that correlates with the radiograph in the previous image is seen in the right iliac bone adjacent to the sacroiliac joint. CT scan findings of bone islands correlate with their plain film appearance.
Ulano et al proposed using CT attenuation (maximum and mean values) to differentiate enostoses from untreated osteoblastic metastases after showing that both methods had high accuracy. A threshold mean CT attenuation of 885 HU and a threshold maximum CT attenuation of 1060 HU had a 95% sensitivity and a 96% specificity. [22] In a follow-up study, however, Elangovan and colleagues noted that radiologists are often asked to interpret imaging studies with limited clinical or treatment history, which can affect CT attenuation accuracy. A retrospective review of CT studies of 165 patients found that a threshold mean CT attenuation of 885 HU had accuracy rates of 91.7% and 81.7% to differentiate enostoses from untreated and treated metastases, respectively, whereas a threshold maximum CT attenuation of 1060 HU had accuracy rates of 81.3% and 72.5% to differentiate enostoses from untreated and treated metastases. [23]
Sala et al studied 46 polytrauma patients who underwent thoracoabdominal CT to determine the frequency of enostosis incidentally found on CT and the ability to distinguish them from untreated osteoblastic metastases (UOM). Twenty patients received a radiologic diagnosis of UOM. Forty-one (89%) patients had 124 enostoses (2-15 mm). The most common sites of occurrence were the proximal femur (34%), the pelvis (22%), the acetabulum (20%), the proximal humerus (11%), the vertebrae (11%), and the rib (2%). Thirteen patients had 1 bone island, 8 had 2, 9 had 3, and 11 had more than 3. Average density was 1007 ± 122 Hounsfiled unit (HU, observer 1) and 1052 ± 107 (observer 2). [24]
A study by Xu et al was conducted to evaluate the utility of Rho/Z (electron density/effective atomic number) on dual-energy computed tomography (DECT) for differentiation of osteoblastic metastases (OBMs) from bone islands (BIs). Researchers assessed diagnostic performance by performing receiver operating characteristic (ROC) analysis and evaluated cutoff values according to ROC curves. Data showed that mean values of Z, Rho, dual-energy index (DEI), and regular CT values (rCT) of OBMs were significantly lower than those of BIs, whereas standard deviation values were higher than those of BIs (all P≤0.05). ROC analysis revealed that 11.86 was the optimal cutoff value for Z, rendering an area under the ROC curve (AUC) of 0.91, with a sensitivity of 91.2% and aspecificity of 82.5%. Researchers concluded that DECT can provide quantitative values of Z, Rho, and DEI and displays good performance in differentiating between OBMs and BIs. [25]
Magnetic Resonance Imaging
Because bone islands are composed of cortical bone, they demonstrate low signal intensity on T1- and T2-weighted MRI scans that is characteristic of cortical bone (see the images below). [1]
T1- weighted, sagittal magnetic resonance imaging (MRI) scan of the knee. Because bone islands are composed of cortical bone, they demonstrate low signal intensity on MRI scans.
 Magnetic resonance imaging (MRI) scan of the hip. A T1-weighted, coronal MRI scan demonstrates a focus of low signal intensity. The bone marrow is abnormally hypo-intense, because normal fatty bone marrow has been replaced with red marrow in this patient, who also has sickle cell disease.
Magnetic resonance imaging (MRI) scan of the hip. A T1-weighted, coronal MRI scan demonstrates a focus of low signal intensity. The bone marrow is abnormally hypo-intense, because normal fatty bone marrow has been replaced with red marrow in this patient, who also has sickle cell disease.
Nuclear Imaging
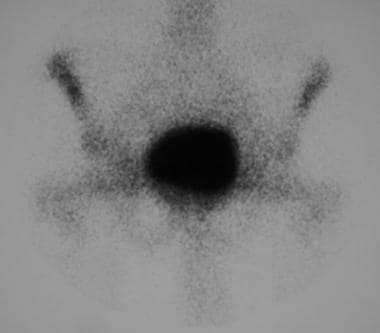
Bone islands do not usually demonstrate increased radiotracer activity on bone scans (see the image below). Thus, bone scans have been used to help differentiate bone islands from more aggressive lesions such as metastases or primary bone tumors, which demonstrate increased scintigraphic activity. [26] However, several reports in the literature on biopsy-proven bone islands have uncharacteristically demonstrated increased radiotracer activity on bone scans. [15] An additional case report described a bone island that could be detected only on single-photon emission CT (SPECT) scans, not on conventional planar images. [6]
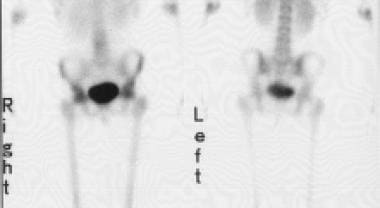 Anteroposterior and posteroanterior views from a whole body bone scan do not demonstrate a corresponding focus of increased scintigraphic activity with the radiograph shown in the previous section on Radiography. Bone islands typically do not appear "hot" on bone scans.
Anteroposterior and posteroanterior views from a whole body bone scan do not demonstrate a corresponding focus of increased scintigraphic activity with the radiograph shown in the previous section on Radiography. Bone islands typically do not appear "hot" on bone scans.
The mechanism of increased scintigraphic activity is unclear but has been hypothesized to be related either to increased metabolic activity or to osteoblastic bone remodeling associated with the growth of bone islands. [27] According to several reports, giant bone islands are more likely to show increased scintigraphic activity (appearing "warm" rather than "hot") on bone scans than are smaller bone islands. [16, 17, 18, 28]
-
Plain-film radiograph of a bone island. Bone islands typically appear as sclerotic, round-to-ovoid intramedullary foci. The long axis of the bone island is aligned parallel to the long axis of the bone.
-
T1- weighted, sagittal magnetic resonance imaging (MRI) scan of the knee. Because bone islands are composed of cortical bone, they demonstrate low signal intensity on MRI scans.
-
Plain film radiograph of the pelvis. A sclerotic focus that is compatible with a bone island is seen in the right iliac bone adjacent to the sacroiliac joint. Bone islands typically are 1 mm to 2 cm in diameter.
-
Computed tomography (CT) scan. A sclerotic focus that correlates with the radiograph in the previous image is seen in the right iliac bone adjacent to the sacroiliac joint. CT scan findings of bone islands correlate with their plain film appearance.
-
Plain film radiograph of the hip. The right iliac bone demonstrates a bone island with "thorny" radiations that merge with the surrounding trabeculae.
-
Magnetic resonance imaging (MRI) scan of the hip. A T1-weighted, coronal MRI scan demonstrates a focus of low signal intensity. The bone marrow is abnormally hypo-intense, because normal fatty bone marrow has been replaced with red marrow in this patient, who also has sickle cell disease.
-
Anteroposterior and posteroanterior views from a whole body bone scan do not demonstrate a corresponding focus of increased scintigraphic activity with the radiograph shown in the previous section on Radiography. Bone islands typically do not appear "hot" on bone scans.
-
Osteopoikilosis. A plain film radiographic image of the knee demonstrates numerous bone islands in a peri-articular distribution that is characteristic of osteopoikilosis.
-
Osteopoikilosis. A plain film radiograph of the pelvis with numerous bone islands that are characteristic of osteopoikilosis
-
Osteopoikilosis. A whole body bone scan for the radiograph of the same patient as in the previous image does not demonstrate increased scintigraphic activity. Osteopoikilosis typically does not appear "hot" on bone scans.








