Practice Essentials
Vitamin D deficiency results in rickets in children with growing bones and causes osteomalacia in adults with completed growth and closed growth plates. By definition, rickets is found only in children before closure of the growth plates, while osteomalacia occurs in persons of any age. Any child with rickets also has osteomalacia, but the reverse is not necessarily true. [1, 2, 3, 4] Children with radiographically confirmed rickets have an increased risk of fracture. [5]
The incidence of nutritional rickets (NR) is rising globally, and hospitalization is increasing even in high-income countries. The underlying calcium deprivation manifests not only as reduced bone mineralization (rickets and osteomalacia) but also as hypocalcaemic seizures, tetany, and dilated cardiomyopathy, including cardiac failure and death. At postmortem, the prevalence of osteomalacia histologically in adult Europeans has been found to be as high as 25%. [6]
The diagnosis of nutritional rickets is made on the basis of history, physical examination, and biochemical testing and is confirmed by radiographs. [5] Plain radiography of the ametaphyseal sites (wrists and ankles) is usually performed to confirm the diagnosis. [7] The distal radius and ulna typically demonstrate rachitic lesions early on radiographs. In preterm neonates and young infants, radiographs of the knee may be more reliable than those of the wrist. In the early stage of rickets, radiographs depict no pathology; however, chemical changes in blood serum can already be found at this time. [4, 8]
(See the images of rickets below.)
 Anteroposterior and lateral radiographs of the wrist of an 8-year-old boy with rickets demonstrates cupping and fraying of the metaphyseal region.
Anteroposterior and lateral radiographs of the wrist of an 8-year-old boy with rickets demonstrates cupping and fraying of the metaphyseal region.
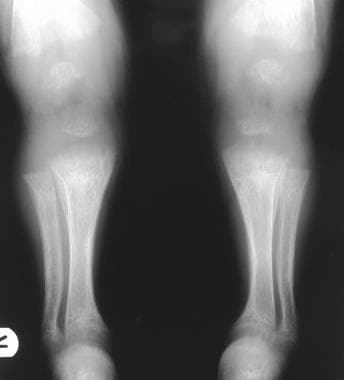
 Radiograph in a 4-year-old girl with rickets depicts bowing of the legs caused by loading.
Radiograph in a 4-year-old girl with rickets depicts bowing of the legs caused by loading.
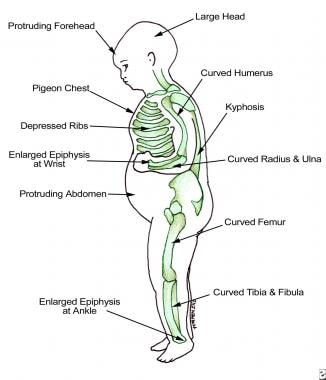
Clinical findings are related to the involved skeletal site, as shown in the image below.
See 21 Hidden Clues to Diagnosing Nutritional Deficiencies, a Critical Images slideshow, to help identify clues to conditions associated with malnutrition.
Radiography
Plain radiograph findings include the following:
-
Widening and cupping of the metaphyseal regions (see the image below)
 Anteroposterior and lateral radiographs of the wrist of an 8-year-old boy with rickets demonstrates cupping and fraying of the metaphyseal region.
Anteroposterior and lateral radiographs of the wrist of an 8-year-old boy with rickets demonstrates cupping and fraying of the metaphyseal region.
-
Fraying of the metaphysis (see the images below)
 Radiographs of the knee of a 3.6-year-old girl with hypophosphatemia depict severe fraying of the metaphysis.
Radiographs of the knee of a 3.6-year-old girl with hypophosphatemia depict severe fraying of the metaphysis.
 Radiograph in a 4-year-old girl with rickets depicts bowing of the legs caused by loading.
Radiograph in a 4-year-old girl with rickets depicts bowing of the legs caused by loading.
-
Craniotabes
-
Bowing of long bones (see the images below)
 Radiograph in a 4-year-old girl with rickets, focused on the knees. Image depicts the development of knock-knees.
Radiograph in a 4-year-old girl with rickets, focused on the knees. Image depicts the development of knock-knees.
 Radiograph of the proximal humerus in a 2.5-year-old girl who had a peripheral neuroectodermal tumor of the right brachial plexus. After treatment with ifosfamide, the patient developed rickets of the proximal femur. In this case, metastasis should be incorporated into the differential diagnosis.
Radiograph of the proximal humerus in a 2.5-year-old girl who had a peripheral neuroectodermal tumor of the right brachial plexus. After treatment with ifosfamide, the patient developed rickets of the proximal femur. In this case, metastasis should be incorporated into the differential diagnosis.
 Radiograph of the knees of an 11-year-old boy with treated vitamin D–resistant rickets. Image demonstrates bilateral multiple growth arrest lines and underdevelopment of the medial aspect of both the tibial plateau and the femoral condyle.
Radiograph of the knees of an 11-year-old boy with treated vitamin D–resistant rickets. Image demonstrates bilateral multiple growth arrest lines and underdevelopment of the medial aspect of both the tibial plateau and the femoral condyle.
-
Development of knock-knees, or genu valgum (see the image below)
 Radiograph of a leg with the patient in a standing position demonstrates knock-knees. The patient is an 11-year-old boy with treated vitamin D–resistant rickets.
Radiograph of a leg with the patient in a standing position demonstrates knock-knees. The patient is an 11-year-old boy with treated vitamin D–resistant rickets.
-
Development of scoliosis
-
Impression of the sacrum and femora into the pelvis, leading to a triradiate configuration of the pelvis
-
In healing rickets, the zones of provisional calcification become denser than the diaphysis. In addition, cupping of the metaphysis may become more apparent.





A useful mnemonic for remembering the findings of rickets is as follows:
-
Reaction of the periosteum (may occur)
-
Indistinct cortex
-
Coarse trabeculation
-
Knees, wrists, and ankles affected predominantly
-
Epiphyseal plates, widened and irregular
-
Tremendous metaphysis (cupping, fraying, splaying)
-
Spur (metaphyseal)
In more advanced stages of rickets, radiographic changes are pathognomonic; however, the underlying cause needs to be established using clinical and biochemical assessments. False-negative findings can occur in the early phase of disease.
-
Anteroposterior and lateral radiographs of the wrist of an 8-year-old boy with rickets demonstrates cupping and fraying of the metaphyseal region.
-
Radiographs of the knee of a 3.6-year-old girl with hypophosphatemia depict severe fraying of the metaphysis.
-
Radiograph in a 4-year-old girl with rickets depicts bowing of the legs caused by loading.
-
Radiograph in a 4-year-old girl with rickets, focused on the knees. Image depicts the development of knock-knees.
-
Radiograph of the proximal humerus in a 2.5-year-old girl who had a peripheral neuroectodermal tumor of the right brachial plexus. After treatment with ifosfamide, the patient developed rickets of the proximal femur. In this case, metastasis should be incorporated into the differential diagnosis.
-
Radiograph of the knees of an 11-year-old boy with treated vitamin D–resistant rickets. Image demonstrates bilateral multiple growth arrest lines and underdevelopment of the medial aspect of both the tibial plateau and the femoral condyle.
-
Radiograph of a leg with the patient in a standing position demonstrates knock-knees. The patient is an 11-year-old boy with treated vitamin D–resistant rickets.
-
Findings in patients with rickets.



