Practice Essentials
Achalasia is an esophageal motor disorder characterized by increased lower esophageal sphincter (LES) pressure, diminished-to-absent peristalsis in the distal portion of the esophagus composed of smooth muscle, and lack of a coordinated LES relaxation in response to swallowing. Patients with achalasia commonly present with dysphagia to solids and liquids, regurgitation unresponsive to proton pump inhibitors, and chest pain. [1, 2, 3, 4, 5, 6, 7, 8]
Endoscopy, barium esophagram, and esophageal manometry are well-established tests that can diagnose achalasia. Important diagnostic clues include retained saliva with a puckered gastroesophageal junction on endoscopy or a dilated esophagus with bird beaking on barium swallow. [7, 9, 10, 11]
Endoscopy can also help exclude pseudoachalasia or other obstruction that may mimic achalasia. Barium esophagram can serve as a complementary test when manometric findings are equivocal. [7, 9, 10]
The Chicago classification is a currently accepted system that separates classic achalasia into 3 clinically relevant subtypes. [12, 13] The manometric findings common to all types of achalasia include impaired relaxation of the LES (residual pressure or integrated relaxation pressure of ≥10 mmHg) and absent peristalsis in a patient without mechanical obstruction near the LES. The types are differentiated as follows:
-
Type I has 100% absent peristalsis and no significant esophageal pressurization.
-
Type II has 100% absent peristalsis with ≥20% of swallows with pan-esophageal pressurization to >30 mm Hg.
-
Type III has ≥20% of swallows with premature spastic contractions (distal latency of < 4.5 s).
(Barium swallow studies of achalasia are presented below.)
 Barium swallow study demonstrating characteristics of achalasia, including the bird's beak deformity and a dilated esophagus.
Barium swallow study demonstrating characteristics of achalasia, including the bird's beak deformity and a dilated esophagus.

 Detail of a barium swallow study demonstrating the classic bird's beak deformity of the distal esophagus.
Detail of a barium swallow study demonstrating the classic bird's beak deformity of the distal esophagus.
Primary achalasia is the most common subtype and is associated with loss of ganglion cells in the esophageal myenteric plexus. These important inhibitory neurons induce LES relaxation and coordinate proximal-to-distal peristaltic contraction of the esophagus. Secondary achalasia is relatively uncommon. This condition exists when a process other than intrinsic disease of the esophageal myenteric plexus is the etiology. Examples of maladies causing secondary achalasia include certain malignancies, diabetes mellitus, and Chagas disease.
The radiologic examination of choice in the diagnosis of achalasia is a barium swallow study performed under fluoroscopic guidance. [14, 15] A diagnosis of achalasia supported by the results of radiologic studies must always be confirmed by performing upper gastrointestinal endoscopy and esophageal manometry. These tests allow the direct evaluation and inspection of the esophageal mucosa and an objective measurement of esophageal contractility. [16, 17, 18, 5, 6]
Normal findings on a barium swallow study do not completely exclude achalasia, especially in the condition's early stages. This situation is when esophageal manometry is most valuable, because the physiologic derangements associated with achalasia precede the development of the anatomic findings discernible by using radiographic studies.
Treatment options for achalasia include pharmacologic, mechanical, botulinum toxin, and surgical-based therapies.
Guidelines
The American College of Gastroenterology (ACG) has published guidelines on the diagnosis and management of achalasia, including the following [9] :
-
Patients who are initially suspected of having GERD but do not respond to acid-suppressive therapy should be evaluated for achalasia.
-
The ACG recommends the use of esophageal pressure topography over conventional line tracing to diagnose achalasia.
-
The ACG notes that using the Chicago Classification to classify achalasia may aid both prognosis and treatment because type II is associated with very good outcomes and type III is associated with more extensive myotomy.
The ACG in their guidelines noted that the functional lumen imaging probe (FLIP) can complement high-resolution manometry (HRM) for the diagnosis of esophageal motility disorders, including achalasia. The FLIP device can depict the pressure geometry relationship in a simulated 3D model and may help in equivocal cases when high-resolution manometry fails to diagnose achalasia. [9, 10, 19, 20, 21, 22]
Guidelines published by the United European Gastroenterology and European Society of Neurogastroenterology and Motility include the following [23] :
-
Recommend the use of high-resolution manometry (with topographical pressure presentation) to diagnose achalasia in adult patients with suspected achalasia.
-
Suggest using a barium esophagram to diagnose achalasia if manometry is unavailable. Suggest using timed barium esophagram, if available, over standard barium esophagram.
-
Suggest against diagnosing achalasia solely by endoscopy.
-
Suggest performing endoscopy in all patients with symptoms of achalasia to exclude other diseases.
-
Suggest additional testing with CT or endoscopic ultrasound only in those patients in whom malignant pseudoachalasia is suspected.
-
Patients who have recurrent or persistent dysphagia after initial treatment should undergo repeat evaluation with timed barium esophagram with or without esophageal manometry.
-
Repeat endoscopy should be considered in patients with recurrent dysphagia.
Radiography
Plain chest radiographs occasionally offer clues in the diagnosis of achalasia. A double mediastinal stripe is occasionally depicted. An air-fluid level can be seen in the esophagus; this is frequently retrocardiac. Because of the paucity of air progressing through the hypertensive LES, the gastric air bubble may be small or absent. [24]
Radiologic features of achalasia may be difficult to demonstrate, especially early in the disease process. Chest radiographic findings have low sensitivity and specificity for the diagnosis of achalasia. If suspected, achalasia should be confirmed with other radiologic examinations, such as barium swallow study under fluoroscopy, and with upper gastrointestinal endoscopy and manometry. [17, 5, 6]
Features of achalasia depicted at barium study under fluoroscopic guidance include the following (see also the images below):
-
Failure of peristalsis to clear the esophagus of barium with the patient in the recumbent position.
-
Antegrade and retrograde motion of barium in the esophagus secondary to uncoordinated, nonpropulsive, tertiary contractions.
-
Pooling or stasis of barium in the esophagus when the esophagus has become atonic or noncontractile (which occurs late in the course of disease).
-
LES relaxation that is incomplete and not coordinated with esophageal contraction.
-
Dilation of the esophageal body, which is typically maximal in the distal esophagus.
-
Tapering of the barium column at the unrelaxed LES, resulting in the bird beak sign.
-
Associated epiphrenic diverticula (possible finding).
Barium swallow study demonstrating characteristics of achalasia, including the bird's beak deformity and a dilated esophagus.
Detail of a barium swallow study demonstrating the classic bird's beak deformity of the distal esophagus.
According to Schima and coworkers, approximately 90% of patients undergoing barium swallow examination for suspected achalasia have some esophageal dilation and a classic bird beak deformity. [25]
A study from El-Takli and colleagues contradicts this claim. [26] These investigators reviewed the barium-contrast radiographs of 51 patients with manometrically diagnosed achalasia. In only 58% of these studies was achalasia mentioned as a diagnostic possibility by the interpreting radiologist. The radiographs were then provided to an expert gastrointestinal radiologist, mixed in with normal control studies. This expert determined that typical radiologic features of achalasia were absent in 50% of the studies performed on achalasia patients. The authors concluded that barium-contrast radiography is not sensitive for the diagnosis of achalasia, frequently due to the lack of characteristic and detectable radiologic features.
A study by Kostic et al—in which preliminary data were gathered on timed barium esophagograms in patients with achalasia, as well as in normal controls—indicated that further studies are necessary before the clinical usefulness of timed barium esophagograms can be confirmed. [27] Subjects were fasted and then given 250 mL of low-density barium sulfate suspension orally. Radiographs were made 1, 2, and 5 minutes after the start of barium administration. The height and width of the barium column and the rate of change over time were recorded.
The study was repeated in all subjects after an approximate 1-week interval. The controls uniformly achieved complete esophageal emptying within 2 minutes. The height and width of the barium column and the rate of esophageal emptying were all markedly abnormal in the achalasia patients. The static data were very reproducible between studies, but the functional (esophageal emptying) data were not, with a coefficient of correlation of only 0.50.
False positives/negatives
No normal variants exist; however, several disease processes can mimic achalasia on chest radiographs or barium swallow studies. These include colon adenocarcinoma, esophageal carcinoma, gastric carcinoma, non–small cell lung cancer, thoracic scleroderma, amyloidosis, Chagas disease, collagen-vascular disease, and lymphoma.
According to Gockel and colleagues, pseudoachalasia, caused by carcinomas or other disease processes or by iatrogenic conditions involving the cardia and gastroesophageal junction, may be indistinguishable from achalasia when conventional endoscopic, manometric, and radiologic diagnostic means are used. [28] In their report, the authors found that pseudoachalasia was caused by primary malignancies in 53.9%, secondary malignancies in 14.9%, and benign lesions in 12.6% of the 264 cases in the series. The remainder of the cases (11.9%) were due to sequelae of operations involving the distal esophagus or proximal stomach.
Esophageal motor abnormalities can result from tumor infiltration of the esophageal wall and associated nerve damage. If mucosal irregularity or mass effect is present at the tapered gastroesophageal junction, pseudoachalasia should be considered. The use of amyl nitrite can often be helpful, as the LES relaxes in achalasia but remains fixed in pseudoachalasia.
Computed Tomography
Computed tomography (CT) scanning with oral contrast enhancement may demonstrate the gross structural esophageal abnormalities associated with achalasia, especially dilatation, which is seen in advanced stages. However, CT findings are nonspecific, and the diagnosis of achalasia cannot be made using CT alone. CT scanning may be indicated in the workup of patients with suspected pseudoachalasia. CT findings should always be confirmed by means of barium swallow study with fluoroscopy, upper gastrointestinal endoscopy, and esophageal manometry.
Disease processes that can mimic achalasia include the following:
-
Colon adenocarcinoma
-
Esophageal carcinoma
-
Gastric carcinoma
-
Non–small cell lung cancer
-
Thoracic scleroderma
-
Amyloidosis
-
Chagas disease
-
Collagen-vascular disease
-
Lymphoma
Ultrasonography
Ultrasonography is not useful in establishing the primary diagnosis of achalasia. [29] However, Eckhardt et al investigated its utility in the differentiation of true achalasia from pseudoachalasia. [30] The authors performed transabdominal ultrasonography in subjects with achalasia (N = 28), in those with pseudoachalasia (ie, neoplasms of the gastric cardia, N = 13), and in 28 age- and sex-matched controls. They found the sensitivity and specificity rates for ultrasonography in the diagnosis of pseudoachalasia to be 100% and 82%, respectively.
Mittal reported on the utility of high-frequency intraluminal esophageal ultrasonography in various esophageal motor disorders, including achalasia, diffuse esophageal spasm, and nutcracker esophagus. [31] Hypertrophy and asynchrony of the longitudinal and circular muscle layers can be identified. Sustained contraction of the longitudinal muscle layer has been shown to correlate with symptoms such as chest pain and heartburn.
-
Barium swallow study demonstrating characteristics of achalasia, including the bird's beak deformity and a dilated esophagus.
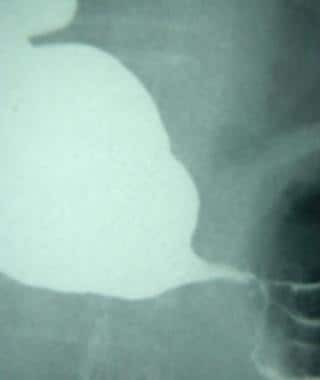
-
Lateral view from a barium swallow study demonstrating a dilated esophagus.
-
Detail of a barium swallow study demonstrating the classic bird's beak deformity of the distal esophagus.





