Overview
Orbital compartment syndrome is an ocular emergency that requires expedient diagnosis and management to prevent blindness. The orbit is a closed compartment created by strong periosteum connections of the orbital septum. An expansive process posterior to the orbital septum leads to rapid expansion in orbital volume and subsequent increase in orbital pressure. Untreated, orbital compartment syndrome results in ischemia of the optic nerve and retina. [1] For more information, see Acute Orbital Compartment Syndrome.
The most common causes of orbital compartment syndrome include retrobulbar hemorrhage from trauma (especially if in hypocoagulable state), [2] retrobulbar anesthetic injection, and eyelid surgery. Spontaneous retrobulbar hemorrhage due to venous anomalies, atherosclerosis, intraorbital aneurysm of the ophthalmic artery, hemophilia, leukemia, von Willebrand disease, and hypertension are uncommon but also have been described. Other causes include prolonged prone positioning, [3] orbital cellulitis (with or without subperiosteal abscess), expanding tumor, orbital emphysema (patient blows nose after a blowout fracture), orbital inflammatory syndrome, and aggressive fluid resuscitation in patients with burns due to third-spacing of fluid in the orbit. [4, 5]
Patients with increased orbital pressure present with pain, proptosis, decreased vision, dyschromatopsia, diplopia, limited extraocular movements, ecchymosis around the eye, bloody chemosis, increased intraocular pressure (IOP), resistance to retropulsion, and a relative afferent pupillary defect.
The lateral and medial canthal tendons attach the eyelids to the orbital rim and are in continuity with the orbital septum, which limits anterior displacement of the globe. [6] Orbital pressure can be relieved with an emergent lateral canthotomy and cantholysis. [7] Without decompression, increased orbital pressure can cause irreversible vision loss due to direct compressive optic neuropathy, central retinal artery occlusion, compression of optic nerve blood supply, or ischemic optic neuropathy from stretching of blood vessels. [8] This loss of vision may occur in as little as 90-120 minutes. [9, 10] Early recognition and prompt treatment are essential for vision loss prevention. [11] Knowledge of this potentially sight-saving procedure is important for clinicians, especially those in remote areas where access to an ophthalmologist is not readily available. [12] Cases of prehospital lateral canthotomy and cantholysis performed by licensed and credentialed individuals, as well as lateral canthotomy and cantholysis completed with improvised tools, have been reported. [13, 14, 15]
Relevant anatomy
The orbit, which protects the globe, is shaped like a cone with four walls. Seven bones conjoin to form the orbital structure, as shown in the image below.
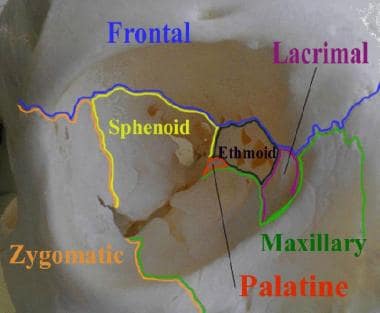 This image of the right orbit shows the 7 bones that contribute to its structure.
This image of the right orbit shows the 7 bones that contribute to its structure.
The lateral orbital wall is formed by the greater wing of the sphenoid and the zygoma. The lateral canthal tendon is a condensation of the superior and inferior crura that insert at the lateral orbital tubercle (Whitnall tubercle) 3 mm posterior to the lateral orbital rim. The lateral canthal tendon is cut during lateral canthotomy and the inferior crus is cut during cantholysis.
For more information about the relevant anatomy, see Orbit Anatomy and Eye Globe Anatomy.
Indications
Lateral canthotomy and cantholysis should be performed for ocular compartment syndrome (most commonly caused by retrobulbar hemorrhage) with acute loss of visual acuity, relative afferent pupillary defect, increased IOP, and proptosis. [16] In the unconscious or uncooperative patient, an IOP greater than 40 mm Hg, especially with a relative afferent pupillary defect, is an indication for lateral canthotomy (normal IOP is 10-21 mm Hg). [17]
Lateral canthotomy may be considered in patients with retrobulbar hemorrhage along with any of the following: ophthalmoplegia, cherry-red macula, retinal venous congestion, optic nerve head pallor, and severe eye pain.
Glaucoma drops decrease intraocular pressure but are not useful for treating orbital compartment syndrome because they do not directly affect intraorbital pressure.
Prompt (< 90-120 minutes) completion of lateral canthotomy and cantholysis is associated with better visual outcomes, although delayed treatment (up to 3 hours) has still yielded some visual recovery after lateral canthotomy/cantholysis. Therefore, all patients with acute ocular compartment syndrome should be considered for prompt lateral canthotomy and cantholysis. [4, 18]
Contraindications
Suspected globe rupture is a relative contraindication to lateral canthotomy. Signs of globe rupture include hyphema; a peaked, teardrop-shaped, or otherwise irregularly shaped pupil; exposed uveal tissue, which appears brownish; and extraocular movement restriction that is greatest in the direction of the rupture. Subtle signs of globe rupture include subconjunctival hemorrhage, enophthalmos, or a conjunctival laceration. For more information, see Medscape Reference article Globe Rupture.
Anesthesia
Local anesthesia (lidocaine 1-2% with epinephrine) is injected at the lateral canthus subcutaneously, taking care to point the needle away from the globe. Additional anesthetic may be supplemented during the procedure but usually is unnecessary. In patients on anticoagulants, this initial bolus is helpful.
Equipment
Equipment needed for the procedure includes the following:
-
Sterile gloves, face shield, gown (if desired)
-
Lidocaine 1-2% with epinephrine
-
Syringe with 27- to 30-gauge needle
-
Sterile drape
-
Normal saline for irrigation
-
Straight hemostat (cautery, if available)
-
Sterile iris or suture scissors or curved Stevens scissors
-
Forceps with ≥0.3-mm teeth
Positioning
The patient should be supine with the head of the bed elevated 10-15°. Unexpected patient head movement can result in iatrogenic injury, including accidental globe puncture. In patients with altered mental state, taping or restraining the head with help from an assistant may be required. Extremely uncooperative patients may require sedation or, rarely, general anesthesia.
Technique
Confirm the affected eye and perform a repeat examination, noting findings of unilateral proptosis, an afferent pupillary defect, decreased visual acuity, and an intraocular pressure (IOP) of 40 mm Hg or higher.
Irrigate the eye with normal saline to clear away debris that may enter the eye or interfere with the procedure
Provide adequate anesthesia by injecting 1 mL of lidocaine 1-2% with epinephrine into the lateral canthal area. Direct the needle tip toward the lateral orbital rim and begin injecting when the needle touches bone. The combination of lidocaine with epinephrine assists with hemostasis and local anesthesia.
Use a straight hemostat to clamp (crimp) the skin at the lateral corner of the patient's eye. Clamp the skin all the way down to the orbital rim for 1-2 minutes. Clamping facilitates hemostasis and marks the location where the incision is to be made. See video below.
Use forceps to pick up the skin near the lower lateral lid near the lashes.
Use the scissors to make approximately a 1-cm incision beginning at the lateral canthus of the eye and extending laterally outward toward the lateral orbital rim. See video below.
This incision is insufficient alone; therefore, proceed to cantholysis.
Apply continuous traction on the lower lid and palpate the lateral canthus tendon. The author prefers to pull the lid away from the globe. Others retract the lid superolaterally.
With the scissors directed along the lateral orbital rim (pointing away from the globe), palpate and dissect the inferior crus of the lateral canthus tendon and cut it. To aid with palpation, the inferior crus can be “strummed” with a pair of closed scissors before cutting it. [3] See video below.
If this procedure is insufficient (ie, IOP remains >40 mm Hg), the superior portion of the lateral tendon can be dissected and then cut, taking care to avoid the lacrimal gland. See video below.
Pearls
Orbital compartment syndrome is an ocular emergency that requires early recognition and treatment to prevent blindness.
Some key points to keep in mind include the following:
-
Treatment should not be delayed to obtain imaging.
-
The essential component that relieves the orbital pressure is the cantholysis, not the canthotomy.
-
Maintain firm retraction on the lower lid; if procedure is adequate, the lower lid should elevate completely off the globe.
-
The eyelid wound may bleed profusely, but there is very little drainage from the retrobulbar hematoma itself. [20]
-
Tonometry and globe palpation are contraindicated in patients with an open globe injury.
-
If inferior cantholysis does not decrease the orbital pressure, complete release of the inferior canthal tendon should be confirmed before proceeding to superior cantholysis. If the latter does not decrease the intraocular pressure, orbital decompression should be considered.
Whenever feasible, seek emergent consultation with an ophthalmologist when this procedure is performed.
The relative afferent pupillary defect, or Marcus Gunn pupil, is tested using the swinging flashlight test. The result is positive when the affected pupil appears to dilate in response to light (the other normal pupil also dilates when light is shone in the affected eye). Both pupils constrict when the light is shone in the normal eye. The Marcus Gunn pupil results from injury to the afferent fibers of cranial nerve II of the defective eye, whereas the efferent signals from cranial nerve III of the normal eye are uninjured.
For more information, see the Medscape Reference article Neuro-Ophthalmic Examination.
Complications
Complications include incomplete cantholysis, iatrogenic injury to the globe or lateral rectus, lower eyelid ectropion, ptosis due to damage to the levator aponeurosis, which is located superiorly2030; and injury to the lacrimal gland and lacrimal artery, which also lie superiorly. Less common complications include bleeding and infection. Extensive cantholysis may result in ectropion. [20] Irreversible vision loss can occur if ischemia time is greater than 90-120 minutes.
If there is corneal exposure, lubricating ointment and a plastic moisture chamber (eg, Tegaderm patch) can be applied without pressure on the globe. Do not apply cotton patches or pressure patches over a proptotic globe.
Accurate Tonometry in the Emergency Department
Despite best attempts to obtain an accurate intraocular pressure measurement in the emergency department, the tonometry reading occasionally is high because of a challenge in opening the swollen eyelids. In this case, a paperclip could be fashioned to create an eyelid retractor and avoid inadvertently compressing the globe while opening tight eyelids.
Questions & Answers
Overview
What is orbital compartment syndrome?
Which anatomy is relevant to lateral canthotomy and cantholysis?
What are the indications for lateral canthotomy and cantholysis?
What are the contraindications for lateral canthotomy and cantholysis?
What is the role of anesthesia in the performance of lateral canthotomy and cantholysis?
What equipment is needed to perform lateral canthotomy and cantholysis?
How are patients positioned prior to performing a lateral canthotomy and cantholysis?
How is a lateral canthotomy and cantholysis performed?
What are pearls for performing lateral canthotomy and cantholysis?
What are the possible complications of lateral canthotomy and cantholysis?
-
Crimping the lateral orbital canthus to mark where to cut the skin.
-
Cutting the lateral canthus.
-
Cutting the inferior canthal ligament/tendon.
-
Verifying laxity of the lower lid after inferior cantholysis.
-
This image of the right orbit shows the 7 bones that contribute to its structure.