Practice Essentials
Fascioliasis is a waterborne and foodborne zoonotic disease caused by two parasites of class Trematoda, genus Fasciola; namely Fasciola hepatica and Fasciola gigantica. [1] (See the image below.) Humans are incidental hosts and become infected by ingesting contaminated watercress or water. The illness occurs worldwide, particularly in regions with intensive sheep or cattle production. Incidence of human infection has increased over the past 20 years. [2, 3, 4]
 Adult Fasciola hepatica fluke stained with carmine (30 mm by 13 mm). Courtesy of the CDC's DPDx, Division of Parasitic Diseases and Malaria.
Adult Fasciola hepatica fluke stained with carmine (30 mm by 13 mm). Courtesy of the CDC's DPDx, Division of Parasitic Diseases and Malaria.
Signs and symptoms
About 15% of infected patients are symptomatic; the majority are asymptomatic. Physical examination typically reveals no specific signs of infection. Abdominal tenderness may be general or may be localized to the right hypochondrium, right upper quadrant, gall bladder, mid epigastrium, or left upper quadrant.
See Presentation for more detail.
Diagnosis
Laboratory studies
About 50% of affected patients have an elevated erythrocyte sedimentation rate. Leukocytosis may occur.
Detection of fasciolid eggs in the stools of infected patients is the most definitive test for diagnosis. Antibody detection is useful during the acute phase of infection, as the acute manifestations of human fascioliasis may precede the appearance of eggs in the stool by several weeks.
Imaging studies
Endoscopic retrograde cholangiopancreatography (ERCP) is considered the gold standard technique of imaging of the biliary tract in patients with the chronic phase of infection.
See Workup for more detail.
Management
Triclabendazole, a benzimidazole derivative, has become the drug of choice for the treatment of fascioliasis. Nitazoxanide is a good alternative to triclabendazole, especially in the chronic stage of infection.
See Treatment and Medication for more detail.
Background
Fascioliasis is a waterborne and foodborne zoonotic disease caused by two parasites of class Trematoda, genus Fasciola; namely Fasciola hepatica and Fasciola gigantica. [1] Humans are incidental hosts and become infected by ingesting contaminated watercress or water. The illness occurs worldwide, particularly in regions with intensive sheep or cattle production. Incidence of human infection has increased over the past 20 years. [2, 3, 4]
Pathophysiology
Sheep, cattle and goats are the definitive hosts. Other alternate herbivore hosts are horses, pigs, buffaloes, donkeys, and pigs. The adult worms reside in the biliary passages of these hosts and are shed in their stools. [5]
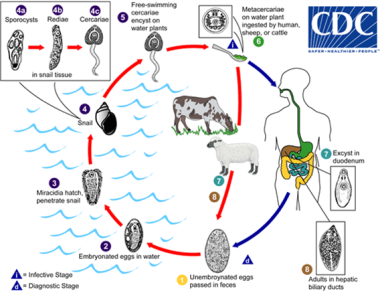 Life cycle of Fasciola hepatica. Immature Fasciola eggs are discharged in the biliary ducts and in the stool (1). Eggs become embryonated in water (2), eggs release miracidia (3), which invade a suitable snail intermediate host (4), including the genera Galba, Fossaria and Pseudosuccinea. In the snail, the parasites undergo several developmental stages (sporocysts (4a), rediae (4b), and cercariae (4c)). The cercariae are released from the snail (5) and encyst as metacercariae on aquatic vegetation or other surfaces. Mammals acquire the infection by eating vegetation containing metacercariae. Humans can become infected by ingesting metacercariae-containing freshwater plants, especially watercress (6). After ingestion, the metacercariae excyst in the duodenum (7) and migrate through the intestinal wall, the peritoneal cavity, and the liver parenchyma into the biliary ducts, where they develop into adult flukes (8). Courtesy of the CDC's DPDx, Division of Parasitic Diseases and Malaria.
Life cycle of Fasciola hepatica. Immature Fasciola eggs are discharged in the biliary ducts and in the stool (1). Eggs become embryonated in water (2), eggs release miracidia (3), which invade a suitable snail intermediate host (4), including the genera Galba, Fossaria and Pseudosuccinea. In the snail, the parasites undergo several developmental stages (sporocysts (4a), rediae (4b), and cercariae (4c)). The cercariae are released from the snail (5) and encyst as metacercariae on aquatic vegetation or other surfaces. Mammals acquire the infection by eating vegetation containing metacercariae. Humans can become infected by ingesting metacercariae-containing freshwater plants, especially watercress (6). After ingestion, the metacercariae excyst in the duodenum (7) and migrate through the intestinal wall, the peritoneal cavity, and the liver parenchyma into the biliary ducts, where they develop into adult flukes (8). Courtesy of the CDC's DPDx, Division of Parasitic Diseases and Malaria.
In humans, maturation from metacercariae into adult flukes takes approximately 3 to 4 months. The adult flukes (F hepatica: up to 30 mm by 13 mm; F gigantica: up to 75 mm) reside in the large biliary ducts of the mammalian host. F hepatica infects various animal species, mostly herbivores (plant-eating animals).
Etiology
The major risk factor is consumption of contaminated water plants or water. Many patients report consuming watercress. [6] Consumption of raw liver from infected sheep, goats, or cows is also a reported cause.
A study that applied a questionnaire and took fecal samples from 270 children in Peru reported that the risk factors for F hepatica were raising cattle, consumption of radishes, and chewing grass and that the prevalence in Baños del Inca district in Cajamarca, Peru was 6.30%. [7]
Epidemiology
United States statistics
F hepatica infection is the only form of fascioliasis reported in the United States and only few such cases are acquired within, mainly reported from Hawaiian Islands, California, and Florida. [8, 9] A large majority of the cases of fascioliasis are imported by travelers from Mexico, Puerto Rico, Haiti, Egypt, Thailand, Yemen, Peru, Portugal, Cape Verde, Ethiopia, Ireland, and Dominican Republic. [9] A few cases of fascioliasis were found in refugees from Southeast Asia living in the United States. [10]
Owing to the endemic prevalence of lymnaeid snails in the United States, domestically acquired cases of fascioliasis are expected to be increasingly reported in the future. [9]
Adult Fasciola hepatica fluke stained with carmine (30 mm by 13 mm). Courtesy of the CDC's DPDx, Division of Parasitic Diseases and Malaria.
 Fossaria bulamoides, a snail host for F hepatica in the western United States. Courtesy of the CDC's DPDx, Division of Parasitic Diseases and Malaria (Conchology, Inc, Mactan Island, Philippines).
Fossaria bulamoides, a snail host for F hepatica in the western United States. Courtesy of the CDC's DPDx, Division of Parasitic Diseases and Malaria (Conchology, Inc, Mactan Island, Philippines).
International statistics
Up to 17 million cases have been estimated to be affected with fascioliasis worldwide. [11, 12] F hepatica typically occurs worldwide in temperate regions, except Oceania. F gigantica causes outbreaks in tropical areas of Southern Asia, [13] Southeast Asia, and Africa. Infection is most prevalent in regions with intensive sheep and cattle production. Miracidia require temperate water to develop and hatch.
A meta-analysis found that the regions of the world with the highest prevalence are South America (9.0%) and Africa (4.8%). The estimated global prevalence of fascioliasis is 4.5%. [14]
Disease prevalence is particularly high in specific regions of Bolivia (65-92%), Ecuador (24-53%), Egypt (2-17%), and Peru (10%). [15, 16] As many as 68% of Bolivian children in hyperendemic areas have evidence of infection, as do 11% of Ethiopians who emigrated to Israel. An epidemic of fascioliasis in Iran was estimated to affect 10,000 people. [17]
In a study of approximately 3000 Egyptian children, 3% were infected. Many were severely anemic. Among individuals who presented with fever of unknown origin to an Egyptian hospital, 4% had F hepatica. F hepatica caused disease that formerly occurred in scattered endemic foci along the Nile River and has now spread throughout the Nile Valley.
Travelers to and immigrants from regions of high endemicity are most frequently affected, as illustrated by a survey of imported cases in the United Kingdom. [18]
A distinct syndrome of fascioliasis, termed halzoun in Lebanon and marrerra in the Sudan, can result from consuming raw livers of infected sheep, goats, or cows. The living fluke adheres to the posterior pharyngeal wall, causing severe pharyngitis and laryngeal edema. Similarly, disease can follow consumption of sashimi of bovine liver served in "Yakitori" bars in Japan, if the liver is contaminated with juvenile worms.
Race-, sex-, and age-related demographics
Race
Fascioliasis infection has no apparent racial predilection.
Sex
Approximately 60% of infections occur in males, which may reflect occupational, dietary, or recreational exposures.
Age
Although most reported patients are adults, fascioliasis appears to equally affect people of all ages. Some geographic difference is observed in the age-related incidence of the disease; for example, it is rarely reported in children in Turkey. In contrast, a study by Ahmad et al, which was conducted in Upper Egypt, found a high prevalence of fascioliasis among elementary school–aged children. [19]
Prognosis
Prognosis is excellent with adequate therapy. However, because of the large numbers of people infected worldwide, fascioliasis causes considerable morbidity. In children, fascioliasis is often associated with severe anemia, although it is seldom fatal.
Complications
Severe anemia and, less commonly, pancreatitis, occur in children more frequently than in adults.
Rare complications include ectopic foci of infection, hemoperitoneum, subcapsular hematoma, [20] hepatic mass, cholecystitis, ascending cholangitis, biliary obstruction, [21] hemobilia from ulceration of the biliary epithelium, gallstones, and sclerosing cholangitis.
Patient Education
Advise patients to avoid high-risk behaviors (ie, consumption of contaminated water plants, water, raw liver).
-
Life cycle of Fasciola hepatica. Immature Fasciola eggs are discharged in the biliary ducts and in the stool (1). Eggs become embryonated in water (2), eggs release miracidia (3), which invade a suitable snail intermediate host (4), including the genera Galba, Fossaria and Pseudosuccinea. In the snail, the parasites undergo several developmental stages (sporocysts (4a), rediae (4b), and cercariae (4c)). The cercariae are released from the snail (5) and encyst as metacercariae on aquatic vegetation or other surfaces. Mammals acquire the infection by eating vegetation containing metacercariae. Humans can become infected by ingesting metacercariae-containing freshwater plants, especially watercress (6). After ingestion, the metacercariae excyst in the duodenum (7) and migrate through the intestinal wall, the peritoneal cavity, and the liver parenchyma into the biliary ducts, where they develop into adult flukes (8). Courtesy of the CDC's DPDx, Division of Parasitic Diseases and Malaria.
-
Adult Fasciola hepatica fluke stained with carmine (30 mm by 13 mm). Courtesy of the CDC's DPDx, Division of Parasitic Diseases and Malaria.
-
Fossaria bulamoides, a snail host for F hepatica in the western United States. Courtesy of the CDC's DPDx, Division of Parasitic Diseases and Malaria (Conchology, Inc, Mactan Island, Philippines).
-
Fasciola hepatica egg in an unstained wet mount (400x magnification). F hepatica eggs are broadly ellipsoidal, operculated, and measure 130-150 μm by 60-90 μm. Courtesy of the CDC's DPDx, Division of Parasitic Diseases and Malaria.
-
Adult of F hepatica observed with ERCP imaging in the common bile duct of a human patient. Courtesy of the CDC's DPDx, Division of Parasitic Diseases and Malaria (Dr. Subhash Agal, Kokilaben Dhirubhai Ambani Hospital, Mumbai, India).







