Overview of Ventricular Arrhythmias
Ventricular arrhythmia (VA) may be an isolated and completely benign finding in children, a marker of serious systemic disease or myopathy, or a mechanism for syncope and sudden cardiac death (SCD).
Isolated premature ventricular contractions (PVCs) are reasonably common. They occur with low daily frequency in as many as 40% of persons with apparently normal hearts. [1, 2, 3, 4] PVCs occur with increased frequency in more than 60% of patients with some types of repaired congenital heart disease (CHD).
By comparison, sustained VA is much less frequent. Although sustained VA can occur in apparently normal hearts, approximately 50% of patients have either CHD or myopathy. An increasingly sophisticated molecular understanding of the role of electrical myopathies, including ion-channel defects such as long QT syndrome (LQTS), offers increased insight into the nature of some of these diseases.
Clinical choices regarding imaging and therapy primarily focus on the potential mortality risks associated with the specific clinical setting. The incidence of SCD in pediatric patients is low. Even among patients with known heart disease, clinical decisions are challenging because of the potential risks of potent antiarrhythmic medications and of nonpharmacologic therapy (eg, catheter ablation, implantable antitachycardia pacemakers and/or defibrillators).
The prognosis cannot be generalized; it must be individualized and based on the underlying diagnosis.
Go to Ventricular Tachycardia for complete information on this topic.
Patient education
Patients with VA and their families must know how to perform cardiopulmonary resuscitation (CPR) and how to contact local emergency medical services (EMS) to promptly begin therapy or prevent excessive therapy, as warranted. Not all patients need a home ambulatory external defibrillator (AED).
For patient education information, see the Heart Center, as well as Tetralogy of Fallot.
Pathophysiology of VA
Reentrant, automatic, or triggered mechanisms may cause ventricular arrhythmia (VA), just as these mechanisms cause supraventricular tachycardia (SVT) and other arrhythmias. Each of these mechanisms can occur in structurally and functionally normal hearts. Both myopericarditis and many forms of cardiomyopathy increase the potential for VAs. Myocardial tumors result in mechanical stresses that facilitate arrhythmias.
Reentrant arrhythmia
Reentrant arrhythmia depends on a circuit, often caused by surgical scar, fibrosis, or fatty degeneration. These areas of functionally abnormal tissue foster the conditions necessary for reentry. These conditions permit a zone of slow conduction, a line of functional unidirectional block, and a circuit that allows circus rhythm to continue.
Pediatric patients with surgical ventricular scars, such as those with postoperative ventricular tachycardia (VT) after repair of tetralogy of Fallot, are commonly cited examples of this mechanism. Chaotic rhythms (eg, ventricular fibrillation) are also examples of reentry mechanisms.
In clinical practice, reentrant rhythms are triggered by premature beats, and the tachycardia is often terminated with direct-current (DC) cardioversion. An abrupt onset and a generally stable rate are other characteristics of reentrant rhythms.
Automatic rhythms
Automatic rhythms are more common than reentrant rhythms in pediatric patients with apparently normal hearts and are caused by abnormal cellular automaticity. The most frequent automatic rhythm is caused by increased spontaneous depolarization of phase 4 of the cardiac action potential.
Abnormal automaticity, in turn, may be the result of metabolic derangement, or the automaticity may be idiopathic. Metabolic derangements that may result in abnormal automaticity include hypokalemia, hypomagnesemia, and local cellular abnormalities (eg, inflammation from myocarditis). High atrial rates suppress, but do not eliminate, automatic VT. These rates vary with the autonomic state, often in complicated fashions. A benign accelerated idioventricular rhythm is an example of an autonomic mechanism.
At a cellular level, ion-channel defects, such as LQTS, allow abnormal cellular automaticity to trigger potentially fatal polymorphic VT, also known as torsade de pointes. Catecholaminergic polymorphic ventricular tachycardia (CPVT) is an increasingly recognized disorder, typically of the ryanodine receptor, characterized by exertionally triggered rapid atrial and ventricular tachycardia and ventricular fibrillation. Triggered arrhythmia may also play a role in poisoning by antiarrhythmic drugs (eg, digoxin). Go to Torsade de Pointes for complete information on this topic.
Epidemiology of VA
United States statistics
The frequency of ventricular arrhythmia (VA) entirely depends on the underlying substrate.
Large pediatric referral centers may encounter 3-5 patients with sustained VT each year. [5] The incidence of low-grade ectopy is notably increased in patients with CHD or cardiac myopathies.
Among patients with CHD, this incidence is concentrated among those who have had ventricular incisions (eg, ventricular septal defects, D-transposition with ventricular septal defects, tetralogy of Fallot) and aortic stenosis; as many as two thirds of patients in this population have some ectopy. This incidence appears to be increased in older patients, probably among those undergoing repair relatively late in life and with techniques used before the mid 1980s.
Although individual underlying myopathies are rare, each contributes to the overall incidence of VA. Hypertrophic cardiomyopathy (HCM) is most common, with a frequency as high as 0.02-0.2% of the population, although the population-based frequency among young people is generally lower. [6] Ion-channel defects (eg, LQTS) are less common; the frequency is difficult to quantitate but is probably approximately 1 case per 5000-10,000 persons. Despite the rarity of these conditions, each has an annual mortality risk as high as 3-5%.
International statistics
The etiology of VA varies internationally. Chagas disease (trypanosomiasis) is an epidemic cause of dilated cardiomyopathy in Brazil and in other regions of South America.
In Europe, a heritable arrhythmogenic right ventricular dysplasia (ARVD) may be a leading cause of sudden death and VT in young people, particularly younger adults. The difference in perceived frequency likely results from a combination of genetic factors, variable definitions of ARVD, and differences in regional recognition of this entity.
Population factors in VA
No significant sex differences have been reported in overall incidence or severity of VA, though patterns of distribution of different LQTS genotypes may vary by sex. In addition, the implications of LQTS, HCM, ARVD, and other genetic cardiac defects appear to have some sex specificity.
Population-based studies in children have been relatively small but demonstrated a biphasic peak of simple ventricular ectopy in apparently healthy infants. This rate decreases during preschool and elementary school ages and increases with adolescence. As patients move into adult life, the incidence of ventricular ectopy continues to steadily increase (see the image below).
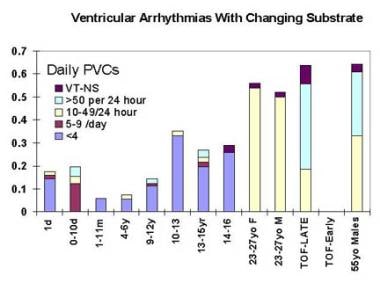 Ventricular arrhythmias with changing substrate. TOF = Tetralogy of Fallot; LATE = Repaired after age 4 years, follow-up after age 12 years. EARLY = Repair before age 1 year, follow-up at age 1 year and age 5 years.
Ventricular arrhythmias with changing substrate. TOF = Tetralogy of Fallot; LATE = Repaired after age 4 years, follow-up after age 12 years. EARLY = Repair before age 1 year, follow-up at age 1 year and age 5 years.
Although as many as 15% of infants and 40% of adolescents have infrequent ventricular ectopy, high-grade ectopy and VT are notably infrequent.
The incidence of VA is somewhat bimodal in patients without structural heart disease. Infants and adolescents have more cases of VA than do toddlers and younger school-aged children. The nature and classification of these cases also differs with age.
In patients with repaired CHD, incidence of VA is notably increased among older adolescents and young adults. This increase may reflect the management approach taken when these patients were younger, the long period after open-heart repair, and/or the influence of autonomic changes on the heart during adolescence.
Sudden cardiac death risk
The overwhelming majority of pediatric patients evaluated for nonsustained VA have no symptoms or only nonspecific palpitations. Obvious concerns include risk of cardiac syncope or SCD. This risk is low, except in selected patients with organic heart disease, for whom the annual risk of sudden death may be as high as 3% for those with sustained VT. The frequency distribution of sudden death in CHD overlaps with that of ventricular ectopy (see the image below).
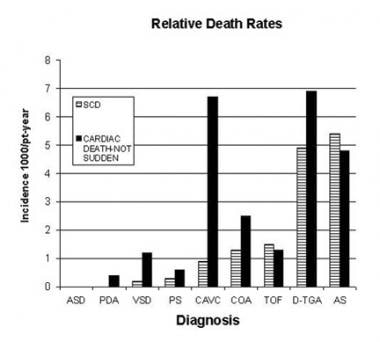 Relative sudden death (arrhythmia) and overall mortality rates for representative types of congenital heart disease. ASD = Atrial septal defect; PDA = Patent ductus arteriosus; VSD = Ventricular septal defect; PS = Valvar pulmonary stenosis; CAVC = Common atrioventricular canal defect; COA = Aortic coarctation; TOF = Tetralogy of Fallot; D-TGA = D-transposition of the great vessels, primarily using atrial switch; AS = Aortic stenosis.
Relative sudden death (arrhythmia) and overall mortality rates for representative types of congenital heart disease. ASD = Atrial septal defect; PDA = Patent ductus arteriosus; VSD = Ventricular septal defect; PS = Valvar pulmonary stenosis; CAVC = Common atrioventricular canal defect; COA = Aortic coarctation; TOF = Tetralogy of Fallot; D-TGA = D-transposition of the great vessels, primarily using atrial switch; AS = Aortic stenosis.
Much concern regarding VA focuses on identifying preventable causes of SCD. The annual incidence of SCD in most clinically defined subgroups of pediatric patients is low. Nonselected pediatric populations have exceptionally low mortality rates (approximately 1-5 deaths per 100,000 patient-years).
In contrast, the annual sudden death rate in the general adult population is 1-3 deaths per 1000 patient-years; the annual mortality rate in adult survivors of myocardial infarction with depressed ventricular function and inducible, nonsuppressible VT is 20%.
For older patients with palliated heart disease or genetic arrhythmias, the risks are higher, although the rate is still usually no more than 1-3% annually. Issues of predicting low-frequency disease—difficult issues in any setting—are magnified in the population with CHD and particularly in the overall pediatric population. Current data suggest that impaired ventricular function and symptoms are both critical risk factors in identifying those patients in whom ventricular arrhythmias are more likely to be either a cause of cardiac arrest or marker of vulnerability. The converse is also true, that for simple heart disease with good ventricular function, overall mortality rates in adolescence and young adulthood are very low, in the range of 0.1% per year or lower.
Among infants and children with minimal symptoms and normal ventricular function (and even very frequent VA, including VT), most have spontaneous resolution of their arrhythmia, with little intercurrent morbidity. [7, 8, 9, 10, 11]
Data about the influence of race in pediatric SCD are limited. Incidences of some heritable myopathies vary by ethnic group. Despite these variations, most diagnoses should be considered in all ethnic groups.
The incidence of LQTS appears to be decreased in blacks, and ARVD appears most frequent in patients of southern European ancestry. Although Brugada syndrome has been identified in many ethnic groups, it is identical to the sudden unexpected nocturnal death syndrome identified in men of Southeast Asian ancestry.
Clinical Presentation
Patient history
The following historical details raise particular concern for ventricular arrhythmia (VA):
-
Presence and severity of symptoms
-
Presence of symptoms with exercise
-
Previous cardiac diagnoses and procedures
-
Family medical history suggestive of inherited disease
-
Potential for recent medication or recreational drug use
In the pediatric population, neurally mediated syncope is so common—and life-threatening arrhythmia is so rare—that investigations of VA in patients with syncope are often unrevealing. Details of the history and family history can direct additional, extensive investigation. Diagnostic findings such as "class II" genetic mutations, which may represent pathologic findings, or nonreproducible findings during intracardiac studies may represent false positives.
A family history of sudden death before age 40 years should raise suspicions, even if the cause was an apparent accident. Numerous familial low-incidence cardiomyopathies have arrhythmia as an important symptom. These cardiomyopathies are characterized by several phenotypes and variable penetrance. When a potentially genetic disorder is identified, careful family investigation can identify other affected families members. The reported yields vary but may approach 50%.
Precipitating events may include the following:
-
Use of prescription or recreational drugs (eg, cocaine)
-
Skeletal myopathy
-
Recent surgical procedures
-
Central lines (eg, direct mechanical ectopy)
-
Recent illnesses (eg, potential for myocarditis); fever may be a potent trigger for VA associated with Brugada syndrome [12]
Prescription drugs that may precipitate VA include tricyclic antidepressants (especially in overdose), and antiarrhythmia medications. Web sites that offer useful references about other drugs that affect repolarization include the following:
-
The initial 1998 American Heart Association (AHA) Scientific Statement, Cardiovascular Monitoring of Children and Adolescents Receiving Psychotropic Drugs
Newer documents have included a comprehensive review of pediatric arrhythmia risks and suggest a more controversial screening practice. These include Cardiovascular Monitoring of Children and Adolescents With Heart Disease Receiving Medications for Attention Deficit/Hyperactivity Disorder. This approach has not been endorsed by either the American or Canadian Pediatric Societies.
Physical examination
Perform a detailed cardiac examination. Focus on clinically apparent arrhythmia and physical signs of heart failure or structural heart disease. Normal results do not exclude serious or life-threatening disease.
In the general physical examination, particularly focus on evidence of occult or apparent skeletal myopathy, neurocutaneous syndromes, rickets, and previous procedures.
Syncope
Apparent cardiac syncope consistently increases the potential of identifying a life-threatening disease that requires active management. Cardiac syncope, in contrast to typical neurally mediated syncope, is characterized by abrupt onset associated with exercise, clinically significant injury, incontinence, seizure, and rapid recovery when arrhythmia is transient.
Palpitations are common in both neurally mediated and cardiac syncope. During benign episodes, these palpitations are often described as hard beats at lower rates, compared with the rapid pulse identified when tachycardia triggers syncope.
Syncope in the presence of known or apparent heart disease should be presumed to represent a potentially serious arrhythmia until proven otherwise. New onset of syncope and VAs may be particularly worrisome.
Near-syncope or dizziness
The vast majority of patients with episodic dizziness, light-headedness, or other presyncopal symptoms have benign or self-limited diagnoses. Clinical correlation is critical when presyncopal symptoms are associated with ventricular ectopy or other arrhythmia.
Palpitations
Patients with isolated premature ventricular contractions (PVCs) and those with sustained arrhythmia may report symptomatic palpitations. Particularly with PVCs, the postextrasystolic beat may have an increased stroke volume.
Of note, many patients do not report any symptoms and cannot identify when they are having ventricular beats. Like syncope, palpitations frequently occur in patients without significant arrhythmia. Ambulatory ECGs (eg, those recorded with Holter or memory-looping event monitors) are critical tools to correlate symptoms and rhythm.
Chest pain
Most chest pain is clearly of musculoskeletal origin (costochondritis). Physical examination in these cases reveals reproducible point tenderness and no clinical suggestion of heart disease.
Another common scenario is atypical chest pain, which is described as brief, sharp, and stabbing. This finding is poorly correlated with exercise and not correlated with the ECG.
Chest pain may represent a marker of hypertrophic cardiomyopathy (HCM) or relatively common diagnoses. Typical angina is extremely rare.
Sudden cardiac death (SCD) and rare cases of coronary artery disease are clearly related in some way. VA may be secondary to Kawasaki disease, multisystem inflammatory syndrome in children (MIS-C) with COVID-19, [13] congenital coronary anomalies, or typical angina.
Pediatric chest pain is typically poorly defined and may include arrhythmia symptoms, pulmonary symptoms, or GI symptoms in addition to anxiety. In pediatric patients, unlike older adults, the serious cardiac causes of chest pain are all rare, which influences both the need for additional testing and the yield of that testing.
Sustained and nonsustained VT
Sustained VT is defined as consecutive ventricular rhythm longer than 30 seconds at rates faster than 110-120 bpm or a comparable arrhythmia requiring urgent cardioversion.
Nonsustained VT includes 3 or more consecutive beats lasting less than 30 seconds. High-grade ventricular ectopy is the VA classification that includes combinations of ventricular couplets and polyform premature ventricular contractions (PVCs), which are more frequent than isolated PVCs and less sustained than VT.
Nonstructural heart disease
Long QT syndrome is a familial ion-channel defect caused by a microdeletion; deletions in chromosomes 3, 4, 7, 11, and 21 have been identified. Although each defect is unique, they share a tendency to abnormal repolarization and an increased risk of sudden death associated with torsade de points.
High-dose beta-blockade has been a mainstay therapy for years. Novel approaches with atrial pacing, implantable cardioverter/defibrillators (ICDs), and gene-specific ion-channel manipulation may help certain patients.
Arrhythmogenic right ventricular cardiomyopathy (ARVC) is the most frequent diagnosis in southern Europeans who die during exercise. This complex and heterogeneous myopathy is associated with fatty degeneration (replacement) of the right ventricular myocardium and inducible VA.
Hypertrophic cardiomyopathy (HCM) may result in SCD, apparently mediated by VT, in young people. High-grade ectopy, as shown on Holter monitoring, is an apparent risk factor for SCD in adults with HCM; however, this finding provides little assistance to pediatric patients. Correlation in genotype-positive families with HCM suggests that as many as a quarter of children and adolescents with mild or early forms of HCM may be missed during ECG screening. [14]
Arrhythmia and mortality risks associated with hypertrophic cardiomyopathy vary widely. Data from population-based pediatric studies and the pediatric cardiomyopathy registry suggest that the risk for older children and adolescents with HCM is 1% per year or less. [6] Infants and those with inborn errors of metabolism represent patients with notably increased risk.
Brugada syndrome represents another identifiable genetic defect (of the sodium channel) that causes VAs. Patients with this syndrome tend to present with a pattern of right bundle-branch block (RBBB) on resting ECG and ST-segment elevation. Both fever and a full stomach may be important triggers of the pattern, and fever is a frequent contributor to childhood events. [12, 15, 16]
Catecholaminergic polymorphic VT is yet another identifiable ion-channel defect that occurs on a relatively frequent familial basis, with recurrent polymorphic VT, a normal resting ECG, and normal repolarization. Genetic studies have identified patients and families with mutations in the ryanodine receptor, among other gene defects. These patients often have atrial and junctional arrhythmias along with relative sinus bradycardia.
Acute myocarditis
Acute viral myocarditis with depressed ventricular function and active inflammation, whatever the etiology, can cause ventricular ectopy and VT. Short-term drug therapy to suppress arrhythmia is indicated while myocarditis is managed.
In cases with profound ventricular dysfunction, urgent transfer for consideration of mechanical support may be life saving.
Arrhythmias may persist well after the hemodynamic dysfunction has resolved.
Occult or focal myocarditis
Although infrequent, cases of focal or occult myocarditis associated with VA have been well documented. Some patients with frequent ectopy or idiopathic VT may also have subclinical myocarditis. Functional imaging studies and endomyocardial biopsy may help identify these patients.
Idiopathic arrhythmias
Idiopathic arrhythmias have characteristic patterns but occur in patients who do not have the diagnoses outlined above.
Benign arrhythmia is always diagnosed with caution on the basis of the symptoms, family history, echocardiogram, response to and rate of exercise, morphology, and persistence of the arrhythmia.
Idiopathic arrhythmias include the following:
-
Isolated PVCs
-
Right ventricular outflow tract VT
-
RBBB VT
-
Accelerated idioventricular rhythm
Infrequent, isolated PVCs, particularly with a trigger such as anesthesia or an intracardiac catheter, require little investigation. PVCs notably more frequent than expected for the patient's age may warrant investigation to seek evidence of sustained arrhythmia.
Right ventricular outflow tract VT is frequently asymptomatic. This arrhythmia has a left bundle-branch block (LBBB) morphology, often-repetitive salvos of VT, possibly subtle MRI findings, and low-to-absent mortality. Arrhythmogenic right ventricular cardiomyopathy (ARVC) is often a difficult diagnostic challenge. Even in families with clear, genetically mediated ARVC, the phenotype is often silent during the pediatric period.
RBBB VT may be automatic. Some occurrences may be reentrant VT triggered by atrial pacing or atrial premature beats. This clearly triggered pattern is more likely to be associated with the left ventricular hemifascicles. This arrhythmia is seen in patients of all ages. RBBB VTs often respond to intravenous verapamil therapy. [17]
Accelerated idioventricular rhythm is typically seen in infants and young children, accelerated idioventricular rhythm rates are slightly faster than sinus beats. LBBB is usually seen, suggesting a right ventricular focus. No mortality has been reported with this condition, and therapy is infrequently needed. Carefully observe affected infants for evidence of increasing VT or decreasing function.
Congenital heart disease
PVCs are seen in as many as two thirds of adolescents and young adults with moderate-to-severe valvar aortic stenosis or repaired tetralogy of Fallot. PVCs are also seen in some patients with ventricular septal defects and in patients with irreparable heart disease, especially those with pulmonary hypertension. In the absence of symptoms, these findings are best interpreted by understanding the hemodynamics of the underlying illness.
The classifications of nonsustained and sustained VT in patients with CHD are identical to those of patients with structurally normal hearts. These classifications should be considered in the context of the patient's symptoms and current hemodynamic status.
The presence of clinical VT and, in some settings, VT induced during electrophysiologic testing, may be independent of other hemodynamic defects in predicting the risk of cardiac arrest and mortality. Careful consultation and evaluation is appropriate.
Tetralogy of Fallot, the defect most commonly associated with spontaneous or induced monomorphic VT, the occurrence of VT is strongly associated with increasing age, increasing age at initial repair, and residual hemodynamic defects. Management choices are complex and may include drug therapy, ICD therapy, ablation, or management of residual hemodynamic issues.
Complications
The most devastating risk is sudden cardiac death or aborted sudden death with subsequent hypoxic-ischemic brain injury. Incessant arrhythmia may induce reversible myopathy, and even transient arrhythmic events produce syncope that results in traumatic injury.
Etiology of VA
Mechanical causes of ventricular arrhythmias (VAs) include the following:
-
Intraventricular catheters
-
Myocardial tumors
Metabolic causes of VAs include the following:
-
Acidemia
-
Hypoxia
-
Fever
-
Hypomagnesemia
Pharmacologic causes of VAs include the following:
-
Digoxin toxicity
-
Proarrhythmia
-
Most antiarrhythmia drugs (especially classes I-A, I-C, III)
-
Positive inotropes and chronotropes (eg dopamine, isoproterenol)
-
Other drug toxicity
-
Anesthesia
Inflammatory causes of VAs include the following:
-
Other myocarditis
-
Electrical myopathies that may cause VAs include the following:
-
Long QT syndrome
-
Brugada syndrome
-
Multisystem inflammatory syndrome in children (MIS-C) with COVID-19
-
Catecholaminergic polymorphic ventricular tachycardia (VT)
Other causes of VAs include the following:
-
Dilated or hypertrophic cardiomyopathy - Muscular dystrophy, IHSS
-
Genetic disorders
-
Structural cardiac disorders - Congenital heart disease (CHD)
-
Neoplasms(eg, rhabdomyoma)
Differential Diagnosis for VA
Problems to be considered in diagnosing ventricular arrhythmia (VA) include the following:
-
Premature ventricular beats
-
Ventricular tachycardia
-
Idioventricular, ventricular, or escape beats or rhythm
-
Supraventricular tachycardia with aberration
-
Supraventricular tachycardia with fixed interventricular conduction defect
-
Supraventricular tachycardia with bystander pre-excitation
-
Antidromic reciprocating tachycardia
-
Pacemaker-mediated tachycardia
There are relatively well-defined algorithms for helping sort through this differential from standard ECGs in older adults. These algorithms are less reliable in pediatric patients, in whom a higher frequency of stable wide complex tachycardia will turn out to be SVT. [18]
See the image below.
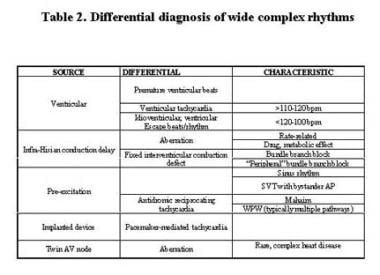 Differential diagnosis of wide-complex rhythms. AV = atrioventricular; SVT = supraventricular tachycardia; WPW = Wolff-Parkinson White syndrome.
Differential diagnosis of wide-complex rhythms. AV = atrioventricular; SVT = supraventricular tachycardia; WPW = Wolff-Parkinson White syndrome.
Electrocardiography
An ECG with a rhythm strip allows for a rapid initial analysis of the morphology, frequency, and electrical substrate of suspected arrhythmia. ECG helps to exclude supraventricular tachycardia (SVT) or atrial arrhythmias with fixed bundle-branch block (BBB) or rate-dependent aberrancy. Leads aVF, V1, and V6 provide sufficient data to classify BBB morphology and estimate frontal-plane axes.
In combination with ambulatory or bedside monitoring systems, ECG provides sufficient data for initial diagnosis of most ventricular arrhythmias (VAs).
Holter monitoring
A 24-hour Holter evaluation provides a quantitative daily snapshot of ventricular ectopy. In patients with suspected cardiac syncope, pay particular attention to QT intervals and T-wave changes for hints of underlying disease. The Holter QTc and ECG measurement of QTc do not have a 1:1 correlation; good data are not available regarding absolute QT/QTc measurements using the rapid sweep speed and high gain typically used in Holter monitoring.
Memory-looping event monitoring
Episodic correlation is best performed by using a memory-looping event monitoring system. Some memory-looping monitors are worn and make continuous recordings. These devices record and hold the waveform before patients activate them.
Other nonlooping "memo" versions are not worn continuously. These systems do not record continuously. Instead, they are activated on symptom onset and, therefore, frequently miss the symptomatic event. They are quite effective in patients with sustained arrhythmias.
Memory-looping systems are preferable for assessment of nonsustained arrhythmias or evanescent symptoms because they can capture the start of a rhythm and because they are most likely to be recording during symptoms. The yield on either system declines rapidly after 2-3 weeks of use.
New surgically implantable, subcutaneous systems may allow for the correlation of symptoms and rhythms in selected patients. [19, 20] Continuous multilead home telemetry is now marketed as a way in increasing the yield of ambulatory monitoring. [21]
Exercise ECG
Exercise typically suppresses benign arrhythmia. In contrast, increasing arrhythmia density and complexity with exercise suggests more problematic mechanisms.
Repeated exercise tests may help in assessing the adequacy of medication and other therapeutic choices. Treadmill exercise is generally more effective at recreating arrhythmias and permits more effective evaluation of blood pressure adaptation in hypertrophic cardiomyopathy (HCM), syncope, and other clinical scenarios.
Overall, exercise testing enhances the sensitivity of ECG monitoring, although it has uncertain reproducibility and specificity.
In adults with decreased left ventricular function, the presence of microvolt T-wave alternans is strongly associated with both ventricular arrhythmias and sudden cardiac arrest. In the pediatric population, although T-wave alternans do seem to be associated with serious VAs, other variables offer more information. In both populations, the absence of microvolt T-wave alternans appears to help select patients at lower risk. [22] Reimbursement and technical issues have limited the use of the test.
Signal-averaged ECGs
Commercial systems permit relatively easy acquisition of signal-averaged ECGs and identification of late potentials. Many high-risk patients with CHD have BBBs or paced rhythms, making the test invalid. Like T-wave alternans, the test is not widely used, with the exception of longitudinal evaluation of patients with suspected ARVC.
Laboratory Studies
Acute symptomatic or sustained VA generally warrants relatively intensive laboratory investigation. Nevertheless, the yield of these tests is typically low when the history, physical findings, and other aspects of the patient's presentation do not suggest specific findings. Most of these studies are omitted in patients with asymptomatic arrhythmia with apparently normal hearts.
Serum electrolyte determinations
Hyperkalemia and hypokalemia, regardless of their cause, are associated with increasing ventricular ectopy and may affect repolarization. Severe hypocalcemia, as seen in rickets, can prolong QT intervals and permit polymorphic ventricular tachycardia (VT).
Hypomagnesemia may be clinically important in patients with cardiac conditions during the immediate postoperative period and in certain other settings.
Toxicology
Administration of multiple therapeutic drugs or abuse of recreational drugs can trigger VA. Pay particular attention to tricyclic antidepressant overdose, use of drugs that may affect the potassium channel (eg, cisapride), and stimulant ingestion.
Thyroid function testing
Although typically associated with other clinical features of hyperthyroidism, elevated thyroxine levels may increase a patient's underlying arrhythmia or may trigger a new arrhythmia. Pay particular attention to thyroid function in patients with a history of amiodarone use.
Other laboratory studies
Other laboratory data, including transaminases and bilirubin levels, may be required to make decisions about drug therapy. Both arterial blood gases and central venous oxygen saturations may help in assessing the hemodynamic severity of arrhythmia in some patients. See the Oxygen Content of Venous Blood calculator.
Genetic testing is now commercially available for many of the genes related to hypertrophic cardiomyopathy (HCM), long QT syndrome (LQTS), Brugada syndrome, and catecholaminergic polymorphic VT. Even with clear clinical diagnoses, as many as 30% of patients with LQTS have negative results on genetic testing, and as many as 80% of patients with Brugada syndrome have negative results on testing.
Limited testing is also available for arrhythmogenic right ventricular cardiomyopathy(ARVC). Updated genetic testing data are summarized on the GeneTest Web site. Some insurers do not cover these tests, which can result in prohibitively expensive charges.
Perform family screening when the results of initial patient assessment suggest familial disease (eg, HCM, LQTS). Genetic testing is exceptionally valuable when evaluating an extended family where the gene is clearly identified and testing can be narrowly focused.
For an individual patient with clinical ambiguity genetic testing remains a tool that often requires detailed judgment. With LQTS, a significant number of mutations are reported that have not been demonstrated to have adverse clinical or cellular electrophysiology effects.
Imaging Studies
Chest radiography
Chest radiography allows for a rapid assessment of ventricular dilatation, pulmonary venous pressure, and mechanical influences (eg, intracardiac catheters). With ready access to echocardiography, the importance of chest radiography has decreased.
Echocardiography
All patients with clinically significant ectopy should undergo a complete echocardiographic examination, ideally in a laboratory skilled in examining children. The following specific details may be sought:
-
Ventricular function (on sinus beats)
-
Wall thickness and chamber dimensions
-
Proximal coronary artery pattern, including efforts to visualize Doppler flow
-
Tumors
-
Structural heart disease
Cardiac MRI
The use of magnetic resonance imaging (MRI) is evolving. Although indications for MRI are uncertain, cardiac MRI is used primarily to assess arrhythmogenic right ventricular dysplasia (ARVD) myocarditis utilizing intravenous gadolinium and tumors. However, data from critical analysis suggest that MRI may result in overdiagnosis of ARVD. [23] Not surprisingly, the test is quite reasonable in adult patients who already meet Task Force Criteria for arrhythmogenic right ventricular cardiomyopathy (ARVC). [24]
When the rhythm is irregular, gating may be insufficient to acquire adequate images. Specific techniques involving delayed enhancement may improve discrimination.
The role of MRI is particularly challenging in patients with a low previous probability of the disease [25] and in younger patients whose fibrofatty infiltrate may not have progressed. [26]
Cardiac Catheterization
Cardiac catheterization is generally reserved for patients with severe symptoms or arrhythmia in whom adequate diagnosis and risk assessment are impossible with noninvasive testing. The asymptomatic patient with infrequent arrhythmias and normal ventricular function or the patient with a clear diagnostic pattern does not routinely need catheterization and invasive EP testing.
Patients with ventricular ectopic rhythms, particularly those with depressed function, may have myocarditis that warrants therapy.
Although echocardiography and other noninvasive tests are excellent, catheterization provides a measurement of hemodynamics in patients with VA who undergo catheterization for other indications.
Except in selected patients with premature coronary artery disease (eg, after heart transplantation), the primary issue is whether abnormalities are present in the origin of the coronaries and in their proximal course. Selective coronary angiography is often necessary to address this issue. Echocardiography, high-resolution CT, and cardiac MRI are excellent noninvasive imaging tools to visualize the proximal coronary arteries.
Right ventriculography may help to diagnose arrhythmogenic right ventricular dysplasia (ARVD) and facilitate mapping studies.
Programmed Electrical Stimulation
Programmed atrial and ventricular stimulation are reasonably effective in reproducing reentrant VA. For patients with CHD, [27, 28] suspected Brugada syndrome, or suspected arrhythmogenic right ventricular dysplasia (ARVD), programmed stimulation may assist in risk stratification or diagnosis.
Voltage mapping in ARVD may assist in identifying areas of low amplitude ventricular signals in the right ventricular free wall and septum that represent substrates for reentry.
Intracardiac recordings and the use of temporary or esophageal wires allow for a firm diagnosis when surface ECGs are unclear.
Programmed stimulation is typically not useful for triggering or excluding automatic ventricular rhythms, which are most common in childhood and adolescence.
Other Studies
Drug challenges
Selected patients may be given serial trials of drugs to either provoke or suppress arrhythmia.
Histologic findings
Histologic findings depend on the ultimate diagnosis. Many patients with serious arrhythmia have entirely normal results on light and electron microscopy. Fibrosis or inflammation may influence therapy.
Treatment of VA
Therapy may not be needed in asymptomatic patients whose VT patterns suggest a low risk of sudden death. Symptoms or a clinically significant short-term risk of SCD frequently warrants admission for evaluation and consideration of therapeutic options.
Initial therapy for ventricular fibrillation is immediate, unsynchronized direct current (DC) defibrillation. Data suggest that a brief (ie, 90 s) period of chest compressions may improve survival when ventricular fibrillation is witnessed, but immediate defibrillation is the therapy of choice. Do not waste time on other aspects of resuscitation before initial defibrillation unless defibrillation is unavailable.
Identify and target potential substrates for arrhythmia-specific therapy.
Optimal inpatient management is performed with secure vascular access and continuous cardiac monitoring. In the ideal case, cardiac monitoring systems are connected to a central monitoring station in a cardiac care unit or ICU. Simple bedside monitors with high-rate and low-rate alarms are inadequate to monitor patients with the potential for unstable VA. For unstable patients, conduct simultaneous evaluation and therapy.
For hemodynamically stable patients, evaluation is followed by serial drug therapy. Diagnostic or therapeutic catheterization also may be performed.
Pharmacologic therapy
Although antiarrhythmic drug therapy can suppress spontaneous arrhythmia and although it may help individual patients, some of these medications have resulted in increased mortality rates in selected adult and pediatric patients. Mortality rates typically increase when the overall risk of the arrhythmia is less than the proarrhythmia risk of the drug. Estimates of both are problematic in pediatrics.
Although digoxin is approved for use in infants, it lacks specific antiarrhythmic properties that aid in the control of most ventricular arrhythmias. All other agents, despite the current use, are not approved for use in young children.
Antiarrhythmic drug therapy is further complicated because no single drug is ideal in all settings. Beta-blockade, with intravenous (IV) esmolol or any of the oral (PO) preparations, is a good initial choice for nearly all forms of VA. In addition, it has few absolute contraindications in the treatment of serious arrhythmia.
Other medications have important limitations. Many are negative inotropes and all have important drug and metabolic interactions. [29] Use of verapamil in children younger than 1 year is associated with infrequent episodes of cardiovascular collapse and death. Procainamide is an excellent choice for incessant reentrant VA in many settings, but it may exacerbate long QT syndrome (LQTS).
Oral agents in Vaughn-Williams class I-A (eg, quinidine, procainamide), class I-C (eg, flecainide, propafenone), or class III (eg, sotalol, amiodarone) can cause ventricular proarrhythmia and suppress clinical arrhythmia while increasing mortality rates in selected populations.
Amiodarone is generally reserved for potentially life-threatening VA. Both IV and oral amiodarone may have important noncardiac adverse effects. Make therapeutic decisions carefully after consulting with an experienced pediatric cardiologist (electrophysiologist).
Intravenous amiodarone in infants and young children deserves particular attention. The medication’s broad efficacy and ready availability has increased its popularity in managing sustained arrhythmias in the ICU and emergency setting. A prospective tiered dose pediatric trial showed good efficacy but a nearly 50% incidence of major adverse events. [30]
Neonates may have relatively frequent episodes of nonsustained ventricular tachycardia or, more precisely, accelerated idioventricular rhythm (AIVR). Although thorough noninvasive evaluation with monitoring and echocardiography is warranted, the risk of mortality is probably zero. Similarly, the risks associated with many forms of VA are quite low in the patient without cardiomyopathy or a probable ion-channel defect.
In both of these settings, avoiding therapy with potentially risky drugs and then choosing an agent that is more effective at decreasing arrhythmias on ambulatory monitoring may be important.
Beta-blockers
Propranolol, atenolol, nadolol, and esmolol are the beta-blockers most frequently used to manage VA. They appear to be particularly effective in treating patients with VA, LQTS, or HCM. Other agents may be useful; sotalol, propafenone, and amiodarone have beta-blocking properties. Beta-blockers have not been associated with ventricular proarrhythmia; this is a major advantage of this class compared with other agents, particularly class I and III agents. Base the choice between beta-blockers on the duration of action, selectivity, and preparation.
Class I antiarrhythmics
This class of agents has complex actions. The drugs primarily block sodium channels, decreasing conduction velocity (QRS widening). Only IV procainamide and lidocaine are presented here. Quinidine, the initial drug in this class, is associated with excessive ventricular proarrhythmia in most patient groups.
Propafenone, disopyramide, flecainide, and other agents may have a role in long-term therapy in some patients. Some children, and adults with ischemic heart disease have increased mortality rates while taking these medications despite apparent control of their arrhythmia. Interesting data suggest that flecainide may offer specific therapy for some patients with CPVT. [31]
Surgical Treatment
Selected patients require highly individualized interventional procedures, such as the following:
-
Excisional biopsy
-
Implantable cardioverter/defibrillators
-
Radiofrequency catheter ablation or cryoablation
-
Left cervical sympathectomy
-
Myocardial tumor resection
Incessant VT is sometimes secondary to focal lipoid cardiomyopathy, isolated fibromas, or hamartomas. In selected patients, surgical excision may be both diagnostic and therapeutic. [32]
ICDs have revolutionized the care of adults with high-risk VT after myocardial infarction. ICDs are increasingly used in high-risk pediatric patients. [33, 34, 35] Transvenous systems have been used in patients who weigh as little as 20 kg. In highly selective situations, toddlers and large infants have received epicardial systems implanted through a sternotomy. [36] Creative, hybrid approaches are further increasing clinicians' willingness to use ICDs in young patients (see the image below).
 Novel pacemaker implantable cardioverter/defibrillator (ICD) in a 14-kg, 3-year-old patient with a long QT, a history of 2:1 block, and an SCN5A mutation. Two bipolar epicardial sew-on leads are used for atrial and ventricular pacing and sensing. A standard single-coil, 45-cm ICD lead is placed along the posterior pericardium and is secured by using the extendable screw. The pacing/sensing portion of that lead is capped and left in the pocket.
Novel pacemaker implantable cardioverter/defibrillator (ICD) in a 14-kg, 3-year-old patient with a long QT, a history of 2:1 block, and an SCN5A mutation. Two bipolar epicardial sew-on leads are used for atrial and ventricular pacing and sensing. A standard single-coil, 45-cm ICD lead is placed along the posterior pericardium and is secured by using the extendable screw. The pacing/sensing portion of that lead is capped and left in the pocket.
Both catheter-directed radiofrequency ablation and intraoperative resection or cryoablation of VT foci have been successful with monomorphic VTs; however, their use is unproved for patients with polymorphic VT.
Unlike supraventricular arrhythmias, for which catheter ablation has a more than 95% success rate, VT ablation in pediatric patients and in patients with CHD has a success rate of about 60%. [37, 38] Both a lack of arrhythmia and proximity to the bundle of His limit the ability to provide effective therapy. [39, 17, 40]
For many years, left cervical sympathectomy was performed for refractory long QT syndrome. The use of video-assisted/minimally invasive techniques has increased the use of this therapy for patients with long QT, CPVT, and recurrent symptomatic arrhythmias. Often this is subsequent to ICD placement. [41, 42, 43]
Consultations
Primary care physicians may certainly observe patients with infrequent asymptomatic premature ventricular contractions (PVCs), often with a 24-hour Holter evaluation, to confirm the frequency and severity of arrhythmia. For most other patients with VA more complex than this, prompt referral and direct communication with a pediatric cardiologist is indicated. Referral facilitates appropriate testing and decision making about evaluating the patient on an inpatient or outpatient basis.
The patterns and relative risks of arrhythmia in adult and pediatric patients differ substantially. Whenever feasible, a cardiologist with specific training and expertise in pediatric heart disease should evaluate the patient. Expedite referral when any of the following indications are present:
-
Symptoms of syncope or apparent heart failure
-
Family history of premature death or seizures
-
History or physical suggesting structural heart disease or heart failure
-
Arrhythmia triggered by medications
-
Arrhythmia triggered by recreational drugs
-
Nonsustained or sustained VT
-
History of cardiac surgery or known heart disease, even if it is apparently repaired
Diet
Diet is rarely is a factor in VA. Diuretic use or abuse, anorexia, or chronic diarrhea can induce hypokalemia, which exacerbates VA. Primary or dietary rickets rarely produces sufficient hypocalcemia to cause QT prolongation and a risk of arrhythmia.
Activity
The updated 2005 Bethesda conference offers a useful initial set of recommendations for patients with ventricular ectopy. [44]
In the absence of detailed investigations and referral, the activity of patients with PVCs that are more than isolated is typically restricted to low-static or low-dynamic activities. Similar restrictions are recommended for those with clinically significant ectopy and most forms of heart disease or symptoms. Patients whose findings on subsequent investigation suggest benign VT often may resume their full activities.
Detailed recommendations for both patients with inherited heart disease and those with CHD have been updated in the 36th Bethesda Conference. [45]
Exercise represents a paradox because its long-term health benefits may lower the overall incidence of cardiac events, but the instantaneous risk of cardiac events appears to increase during or immediately after exertion. Some patients with prolonged-QT syndrome have drowned, particularly after diving into cold water, presumably because they developed ventricular fibrillation.
Elite athletes, particularly males, may have an athletic heart syndrome that can include mildly increased left ventricular mass with normal left ventricular cavity dimensions. One third of these patients have more than 100 premature ventricular beats per 24 hours with other higher-grade ectopy, including couplets and nonsustained VT.
Further inpatient care
Admit patients with new and unprotected symptoms of apparent cardiac syncope to a monitored setting to ensure their safety during evaluation.
Perform intracardiac procedures, some of which may be performed as same-day admissions. Revise or place implantable defibrillators. Initiate antiarrhythmic therapy.
Further outpatient care
Patients with conditions beyond asymptomatic, isolated, premature ventricular beats should receive episodic monitoring of their clinical status. They may require repeated assessment of ventricular function with echocardiography, repeated Holter or event monitoring, and monitoring for drug effects when drugs are used.
Device-based therapy requires a follow-up system to evaluate and manage the consequences and complications of therapy.
Transfer
Patients with apparent cardiac syncope and VA require prompt evaluation by a cardiologist. Transfer the patient to a setting that can ensure adequate monitoring, skilled nursing, and an experienced pediatric cardiology team.
Deterrence
For many rhythms, complete suppression is neither warranted nor advisable. Carefully monitor the administration of drugs that affect repolarization (eg, cisapride, major antipsychotics, tricyclic antidepressants) because monitoring may decrease the risk of torsade de pointes in patients taking these medications.
Prudent preventive measures for patients with VA include avoiding known triggers and sustained drug use, especially recreational drug use.
Therapy with beta-blockers and possibly other medications may help decrease the risk in patients with HCM and in symptomatic patients with LQTS. No particular therapy clearly prolongs survival in high-risk patients with dilated cardiomyopathy or CHD.
-
Relative sudden death (arrhythmia) and overall mortality rates for representative types of congenital heart disease. ASD = Atrial septal defect; PDA = Patent ductus arteriosus; VSD = Ventricular septal defect; PS = Valvar pulmonary stenosis; CAVC = Common atrioventricular canal defect; COA = Aortic coarctation; TOF = Tetralogy of Fallot; D-TGA = D-transposition of the great vessels, primarily using atrial switch; AS = Aortic stenosis.
-
Ventricular arrhythmias with changing substrate. TOF = Tetralogy of Fallot; LATE = Repaired after age 4 years, follow-up after age 12 years. EARLY = Repair before age 1 year, follow-up at age 1 year and age 5 years.
-
Differential diagnosis of wide-complex rhythms. AV = atrioventricular; SVT = supraventricular tachycardia; WPW = Wolff-Parkinson White syndrome.
-
Novel pacemaker implantable cardioverter/defibrillator (ICD) in a 14-kg, 3-year-old patient with a long QT, a history of 2:1 block, and an SCN5A mutation. Two bipolar epicardial sew-on leads are used for atrial and ventricular pacing and sensing. A standard single-coil, 45-cm ICD lead is placed along the posterior pericardium and is secured by using the extendable screw. The pacing/sensing portion of that lead is capped and left in the pocket.
-
ECG in a 12-year-old boy.
Tables

What would you like to print?
- Overview of Ventricular Arrhythmias
- Pathophysiology of VA
- Epidemiology of VA
- Presentation
- Etiology of VA
- Differential Diagnosis for VA
- Electrocardiography
- Laboratory Studies
- Imaging Studies
- Cardiac Catheterization
- Programmed Electrical Stimulation
- Other Studies
- Treatment of VA
- Show All
- Media Gallery
- References




