Background
Sulfite oxidase deficiency is an inborn error of the metabolism of sulfated amino acids. Individuals affected with sulfite oxidase deficiency most commonly present in the neonatal period with intractable seizures, characteristic dysmorphic features, and profound intellectual disability. Molybdenum cofactor deficiency, which affects the functioning of sulfite oxidase, leads to a similar phenotype.
Pathophysiology
Inherited defects in the sulfite oxidase enzyme can cause the phenotype of sulfite oxidase deficiency. However, many cases of this disorder are associated with deficiency of the molybdenum-containing pterin cofactor (molybdenum cofactor deficiency). Molybdenum cofactor is associated with the enzymes sulfite oxidase, xanthine dehydrogenase, and aldehyde oxidase (see the image below). [1]
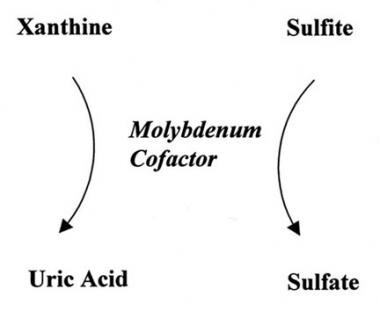
Sulfite oxidase is located in the mitochondrial intermembranous space and is involved in electron transport. It leads to oxidation of sulfite to sulfate. [2] The enzyme sulfite oxidase depends on the molybdenum-containing pterin cofactor, as do the enzymes xanthine dehydrogenase and aldehyde oxidase. Xanthine dehydrogenase catalyzes the hydroxylation of xanthine and hypoxanthine to produce uric acid. [3] Aldehyde oxidase hydroxylates hypoxanthine into xanthine and functions in detoxification. Deficiency of xanthine oxidase and aldehyde oxidase is not known to cause neurologic disease and may not produce symptoms. [4]
As sulfite oxidase deficiency and molybdenum cofactor deficiency have virtually identical phenotypes, the CNS toxicity appears to be secondary to loss of function of sulfite oxidase. Methionine and cysteine normally are metabolized to sulfite and then are oxidized to sulfate by the enzyme sulfite oxidase (see the image below).
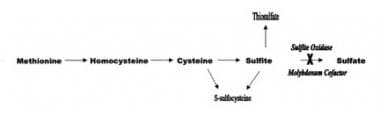 Sulfite oxidase deficiency and molybdenum cofactor deficiency in the metabolism of sulfated amino acids.
Sulfite oxidase deficiency and molybdenum cofactor deficiency in the metabolism of sulfated amino acids.
When sulfite oxidase is deficient, alternate metabolic pathways for sulfite are augmented, including formation of metabolites s-sulfocysteine and thiosulfate. S-sulfocysteine probably substitutes for cysteine in connective tissues. This substitution appears to weaken the zonule of the lens (a tissue normally rich in cysteine) and results in the characteristic dislocated lenses. The pathogenesis of the brain damage in those with sulfite oxidase deficiency is not known but may be related to sulfite accumulation or lack of sulfate in the CNS.
Epidemiology
Frequency
United States
The frequencies of sulfite oxidase deficiency and molybdenum cofactor deficiency are unknown; however, these disorders are probably underdiagnosed.
International
Worldwide, approximately 50 cases of sulfite oxidase deficiency have been reported. [4] The preponderance of reported cases in Europe and the United States most likely represents increased recognition in these countries. Closer to 100 cases of molybdenum cofactor deficiency have been reported. The estimated prevalence of molybdenum cofactor deficiency 1 per 100,000-200,000 newborns worldwide. [5]
Mortality/Morbidity
In most cases, sulfite oxidase deficiency is fatal in infancy or early childhood. Survivors of sulfite oxidase deficiency often have profound intellectual disability. Some later-onset cases with more favorable outcomes have been reported. Of note, some types of molybdenum cofactor deficiency have been responsive to treatment, leading to better longer-term outcomes.
Race
Molybdenum cofactor deficiency and sulfite oxidase deficiency are panethnic.
Sex
Both sexes are equally affected.
Age
Traditionally, infants with sulfite oxidase deficiency were reported to present in the neonatal period. [6] However, an increasing number of patients have been reported with later onset or deterioration after an intercurrent illness.
Prognosis
Most cases of sulfite oxidase deficiency are fatal in infancy or early childhood. The prognosis may be more variable for later-onset cases. Survivors of this disorder often have profound intellectual disability. Some later-onset cases with more favorable outcomes have been reported. Of note, some types of molybdenum cofactor deficiency have been responsive to treatment, leading to better longer-term outcomes. Individuals with molybdenum cofactor deficiency type A who are eligible for and treated early with cPMP replacement may have a better prognosis.
Patient Education
Sulfite oxidase deficiency is inherited in an autosomal-recessive manner. Two parents who are both carriers of pathogenic variants have a 25% recurrence risk for sulfite oxidase deficiency in future children. Genetic counseling is encouraged, including information about prenatal and preimplantation diagnosis to parents of individuals with this disorder.
-
Molybdenum cofactor deficiency.
-
Sulfite oxidase deficiency and molybdenum cofactor deficiency in the metabolism of sulfated amino acids.
-
Pictured is an infant with sulfite oxidase deficiency. Note the narrow bifrontal diameter and deep-set eyes.

