Background
Aniridia is a congenital, hereditary, bilateral, extreme form of iris hypoplasia that may be associated with other ocular defects. [1, 2, 3, 4] It describes an extreme form of iris hypoplasia in which the iris appears absent on superficial clinical examination; however, gonioscopy shows the presence of the iris root. Aniridia is not just an isolated defect in iris development; it is a panocular disorder with macular and optic nerve hypoplasia, cataract, and corneal changes, anomalies that lead to decreased vision and nystagmus. Visual acuity generally is low but is unrelated to the degree of iris hypoplasia. Glaucoma is a secondary problem causing additional visual loss over time. [5]
Patients with aniridia usually lack a foveal reflex, indicating poor macular development. True aplasia of the optic nerve also can occur. All these patients need specialized management of each individual problem. Because of poor visual acuity and nystagmus, low vision aids are very helpful. Lifelong regular follow-up care is necessary for the early detection of any new problems, especially glaucoma, lens, and systemic problems, so that timely treatment is given. [6] Since the condition has a dominant transmission, proper genetic counseling should be obtained. Aniridia is shown in the images below.
Clinical manifestations
Clinical manifestations include the following:
Isolated aniridia
Aniridia in association with systemic defects
-
Genitourinary abnormalities
-
Intellectual disability [10]
-
Central nervous system problems such as olfactory and hearing difficulties, cognition and behavioral problems, or developmental delay in patients with isolated aniridia [11]
Aniridia in association with ocular defects [12, 11, 13]
-
Albinism
-
Ectopia lentis (50%)
-
Spontaneous lens dislocation
-
Cataract (50-85%)
-
Glaucoma (30-50%)
-
Nystagmus
-
Strabismus
-
Optic nerve hypoplasia (75%)
-
Optic nerve coloboma
-
Aniridia-associated keratopathy (AAK) (20%)
-
Foveal hypoplasia
-
Bilateral ptosis (%10)
-
Meibomian gland dysfunction
-
Microcornea
-
Persistent pupillary membrane
-
Aniridic fibrosis syndrome
Pathophysiology
The pathogenesis of aniridia is attributed to a primary developmental arrest of the neuroectoderm and a secondary alteration of all 3 neural crest waves of the mesenchyme. The functional development of the anterior segment is a complex interrelationship between the neural ectoderm and the neural crest waves of the mesenchyme. The pathogenesis may involve defective formation or excessive regression of various layers of the anterior segment caused by cellular or biochemical aberrations. This explains the combined anterior and posterior segment neural ectodermal and mesenchymal defects. The iris stroma is hypoplastic, indicating an altered third neural crest wave of mesenchyme.
The occurrence of aniridia is classified as the following:
-
Autosomal dominant, isolated congenital aniridia without systemic involvement [14]
-
Sporadic congenital aniridia; chromosome deletion of the short arm of chromosome 11, including band p13 (WAGR Syndrome) [15]
-
Autosomal recessive congenital aniridia (Gillespie Syndrome) [10]
The exact defect in iris morphogenesis giving rise to aniridia is unknown. Because the iris pigment epithelium, the iris musculature, the retina, and the optic nerve are derived from neuroectoderm, there may be a common embryologic origin for these anomalies. As an isolated ocular malformation, aniridia is an autosomal dominant disorder, which is caused by a mutation in the PAX6 (paired box gene family) gene. [16, 17, 18]
Patients with aniridia who have a positive family history are not at an increased risk for Wilms tumor. Two genetic loci for aniridia have been identified: one (AN1) on chromosome arm 2p and one (AN2) on chromosome 11.
Patients with aniridia without a positive family history have a 30% chance of developing Wilms tumor, and they represent new mutations for the autosomal dominant gene. About one third of such patients have a mutation that affects the WT and AN2 loci, causing the patient to develop Wilms tumor; the other two thirds of patients have a mutation of just the AN2 locus. Because of the high mortality from Wilms tumor, those patients with the WT and AN2 mutations have a low probability of reproducing, whereas those with just AN2 mutations have normal fertility and, hence, a 50% risk to pass the aniridia gene mutation to each child.
Epidemiology
Frequency
Aniridia is a rare disease with an incidence of 1.8 per 100,000 live births. [19] The incidence ranges from 1/60,000 to 1/100,000 live births. The autosomal dominant form accounts for about two thirds of cases. The sporadic form accounts for one third of cases. [20]
Mortality/Morbidity
All patients with aniridia are visually handicapped for a lifetime. This already reduced vision is threatened further by such complications as cataract and glaucoma. Patients with Wilms tumor have a reduced span of life.
Race
Aniridia has no racial predisposition.
Age
Congenital glaucoma and aniridia usually are not associated at birth. The glaucoma develops at either the preteen or the teenage level.
Significant cataracts may occur before puberty. The risk for cataract increases with age, with lens opacities observed in 50-85% of patients during the first 2 decades of life.
See Primary Congenital Glaucoma and Secondary Congenital Glaucoma.
Prognosis
The prognosis of aniridia varies from patient to patient.
Unmonitored and untreated elevated intraocular pressure may damage vision.
Cataract may require surgery.
Progressive corneal opacification may need corneal grafting.
Patient Education
Thoroughly educating the patient and parents about aniridia and the associated ocular anomalies and systemic problems is mandatory.
-
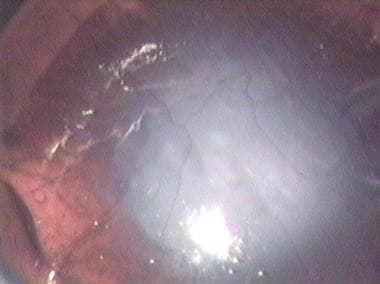
Aniridia with superiorly dislocated cataract.
-
Aniridia. Close-up of the superior limbus of same patient as in the image above to show pannus.
-
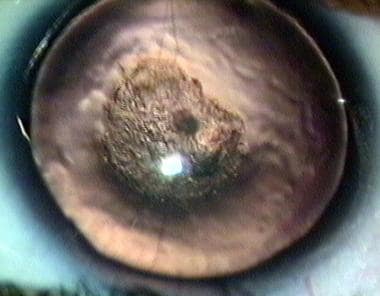
Aniridia with a vascularized corneal opacity in a young patient.
-
Centrally placed cataractous lens and aniridia in a pediatric patient.
-
Aniridia. 3-D image showing absence of the inferior half of the iris and absence of most of the anterior leaf of the iris in the upper half. In the less affected area, the iris is represented mostly by the posterior pigment epithelium. No choroidal coloboma was present.
-
Aniridia and aphakia following perforating injury.
-
Single piece intraocular lens inside the bag, in a case of aniridia.
-
Multipiece intraocular lens inside the bag, in a case of aniridia.
-
In-the-bag intraocular lens. The lens has been displaced superiorly.
-
Aniridia. A single piece nonfoldable lens has been implanted after placing an endocapsular ring. An endocapsular ring provides better chances of centration.
-
Partial traumatic aniridia. The lost iris gap has been covered by the use of a lens optic that is clear in the center and is opaque at the periphery. A scleral fixated lens has been used in this case.







