Practice Essentials
Neurocysticercosis is the result of accidental ingestion of eggs of Taenia solium (ie, pork tapeworm), usually due to contamination of food by people with taeniasis. In developing countries, neurocysticercosis is the most common parasitic disease of the nervous system and is the main cause of acquired epilepsy. In the United States, neurocysticercosis is mainly a disease of immigrants.
Signs and symptoms
Clinical manifestations of neurocysticercosis vary with the locations of the lesions, the number of parasites, and the host's immune response. [1] Many patients are asymptomatic. Possible symptomatic presentations include the following:
-
Epilepsy: Most common presentation (70%) [2]
-
Headache, dizziness
-
Stroke
-
Neuropsychiatric dysfunction
Onset of most symptoms is usually subacute to chronic, but seizures present acutely
Abnormal physical findings, which occur in 20% or less of patients with neurocysticercosis, depend on where the cyst is located in the nervous system and include the following:
-
Cognitive decline
-
Dysarthria
-
Extraocular movement palsy or paresis
-
Hemiparesis or hemiplegia, which may be related to stroke, or Todd paralysis
-
Hemisensory loss
-
Movement disorders
-
Hyper/hyporeflexia
-
Gait disturbances
-
Meningeal signs
See Clinical Presentation for more detail.
Diagnosis
Neurocysticercosis is commonly diagnosed with the routine use of diagnostic methods such as computed tomography (CT) and magnetic resonance imaging (MRI) of the brain.
Imaging studies
CT findings vary as follows, depending on the stage of evolution of the infestation:
-
Vesicular stage (viable larva): Hypodense, nonenhancing lesions
-
Colloidal stage (larval degeneration): Hypodense/isodense lesions with peripheral enhancement and perilesional edema
-
Nodular-granular stage: Nodular-enhancing lesions
-
Cysticercotic encephalitis: Diffuse edema, collapsed ventricles, and multiple enhancing parenchymal lesions
-
Active parenchymal stage: The scolex within a cyst may appear as a hyperdense dot
-
Calcified stage: When the parasite dies, nodular parenchymal calcifications are seen (see the image below)
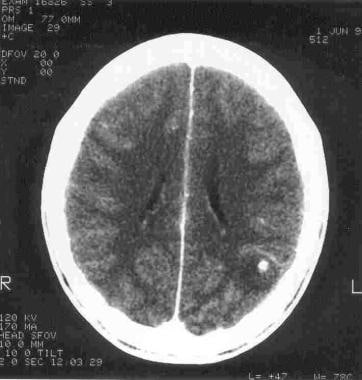 Computed tomographic (CT) scan of the brain in a patient who presented with an episode of generalized tonic-clonic seizure. Note the calcified lesion in the left parieto-occipital region. Subsequent evaluation confirmed the diagnosis of neurocysticercosis.
Computed tomographic (CT) scan of the brain in a patient who presented with an episode of generalized tonic-clonic seizure. Note the calcified lesion in the left parieto-occipital region. Subsequent evaluation confirmed the diagnosis of neurocysticercosis.

MRI is the imaging modality of choice for neurocysticercosis, especially for evaluation of intraventricular and cisternal/subarachnoidal cysts. Findings on MRI include the following:
-
Vesicular stage: Cysts follow the CSF signal; T2 hyperintense scolex may be seen, with no edema and usually no enhancement
-
Colloidal stage: Cysts are hyperintense to the CSF; there is surrounding edema, and the cyst wall enhances
-
Nodular-granular stage: The cyst wall thickens and retracts, there is a decrease in edema, and nodular or ring enhancement is present
Lab studies
CSF analysis for neurocysticercosis is indicated in every patient presenting with new-onset seizures or neurologic deficit in whom neuroimaging shows a solitary lesion but does not offer a definitive diagnosis. CSF is contraindicated in cases of large cysts causing severe edema and displacement of brain structures, as well as in lesions causing obstructive hydrocephalus.
CSF findings include the following:
-
Mononuclear pleocytosis
-
Normal or low glucose levels
-
Elevated protein levels
-
High IgG index
-
Oligoclonal bands, in some cases
-
Eosinophilia (5-500 cells/µL); however, this also occurs in neurosyphilis and CNS tuberculosis [3]
-
CSF ELISA for neurocysticercosis has a sensitivity of 50% and a specificity of 65%
Other tests are as follows:
-
Stool examination: 10-15% of neurocysticercosis patients have taeniasis
-
Brain biopsy: Necessary only in extreme cases
See Workup for more detail.
Management
Treatment of neurocysticercosis depends upon the viability of the cyst and its complications. [4] If the parasite is dead, the approach is as follows:
-
Treatment is directed primarily against the symptoms
-
Anticonvulsants are used for management of seizures; monotherapy is usually sufficient
-
Duration of the treatment remains undefined
If the parasite is viable or active, treatment varies as follows:
-
Patients with vasculitis, arachnoiditis, or encephalitis: A course of steroids or immunosuppressants is recommended before the use of anticysticercal drugs
-
Antiparasitic treatment [5] with albendazole is also useful in cysticercosis of the racemose type (ie, multiple cysts in the basal cisterns)
-
Patients with parenchymal, subarachnoid, or spinal cysts and without complications (eg, chronic epilepsy, headaches, neurologic deficits related to strokes, and hydrocephalus): anticysticercal treatment can be considered, with the concomitant use of steroids
-
Multiple trials with anticysticercal treatment may be required for giant subarachnoid cysts
-
Patients with seizures due to viable parenchymal cysts: antiparasitic therapy [6]
Indications for surgical intervention and recommended procedures are as follows:
-
Hydrocephalus due to an intraventricular cyst: Placement of a ventricular shunt, followed by surgical extirpation of the cyst and subsequent medical treatment [7]
-
Multiple cysts in the subarachnoid space (ie, the racemose form): Urgent surgical extirpation
-
Obstruction due to arachnoiditis: Placement of a ventricular shunt followed by administration of steroids and subsequent medical therapy
See Treatment and Medication for more detail.
Background
Neurocysticercosis (NCC) is the most common parasitic disease of the nervous system and is the main cause of acquired epilepsy in developing countries. It has also been a problem in industrialized countries because of the immigration of tapeworm carriers from areas of endemic disease. [8, 9]
Neurocysticercosis can be acquired via fecal-oral contact with carriers of the adult tapeworm Taenia solium. This usually indicates the presence of a tapeworm carrier in the immediate environment (ie, household) or by accidental ingestion of contaminated food. Cases of auto-ingestion, in which persons with taeniasis may ingest the eggs of T solium into their intestine, have been reported.
An example of an image of human neurocysticercosis is provided below.
 Massive nonencephalitic neurocysticercosis. Photo courtesy of Cysticercosis Working Group in Peru.
Massive nonencephalitic neurocysticercosis. Photo courtesy of Cysticercosis Working Group in Peru.
See also Neuroimaging in Neurocysticercosis.
Pathophysiology
Neurocysticercosis is the result of accidental ingestion of eggs of Taenia solium (ie, pork tapeworm), usually due to contamination of food by people with taeniasis. T solium has a 2-host biologic cycle, with humans as the definitive hosts carrying the intestinal tapeworm, and pigs as the normal intermediate hosts harboring the larvae or cysticerci. This parasite has a head (scolex) with 4 suckers and a double crown of hooks, an unsegmented neck, and a large body with several hundreds of hermaphrodite proglottids.
Cysticerci are ingested by humans through poorly cooked infected pork. Cysts evaginate in the small intestine, attach to the wall by its suckers and hooks, and develop strobila or chains of proglottids. From the distal end of the strobila, fertile eggs are excreted into the gravid proglottids. Up to 60,000 eggs may be contained in a proglottid.
Pigs ingest stool contaminated with Taenia eggs, the embryos actively cross the intestinal wall, get into the bloodstream, and are transported to most tissues, where they reside as cysticerci. Larvae are found most commonly in the central nervous system (CNS), but they can also be located in the eye, muscle, or subcutaneous or other tissues.
Epidemiology
Neurocysticercosis is the most common parasitic infection of the central nervous system (CNS). Approximately 2.5 million people worldwide carry the adult tapeworm, and many more are infected with cysticerci.
In the United States, neurocysticercosis is mainly a disease of immigrants, and the disease is prevalent in the states of California, Texas, and New Mexico. Neurocysticercosis represents a major cause of morbidity among the Hispanic population. Although most of the cases have been diagnosed in persons of Hispanic origin, the incidence is increasing in nonendemic countries because of travel to zones of endemic disease. Native cases have also been reported, presumably because of ingestion of infected food that was handled by carriers of T solium.
The incidence of neurocysticercosis has been steadily increasing in the United States. Although still mostly prevalent in the southwestern United States, imported cases have been reported throughout the country.
Globally, neurocysticercosis is endemic in Central and South America, sub-Saharan Africa, and in some regions of the Far East, including the Indian subcontinent, Indonesia, and China, reaching an incidence of 3.6% in some regions. This disease is rare in Eastern and Central Europe, in North America (with the exception of Mexico), and in Australia, Japan, and New Zealand, as well as in Israel and in the Muslim countries of Africa and Asia.
Cysticercosis can be seen in immigrant populations with a relatively high frequency, as in the US Southwest and South Africa, and subcutaneous cysticercosis is more common in Asian populations than in other peoples of other areas of endemic disease. It is not clear whether this is due to variations in parasite strain or to those in the host.
Although neurocysticercosis appears to affect men and women equally, there is some evidence to suggest that inflammation around the parasites may be more severe in women than in men. [10] In addition, despite the fact that neurocysticercosis appears to be the most frequent cause of seizures in children [11] and adults (peak incidence, 30-40 y), the exact incidence in children is not known.
Prognosis
In most patients with neurocysticercosis, the prognosis is good. Associated seizures seem to improve after treatment with anticysticercal drugs and, once treated, the seizures are controlled by a first-line antiepileptic agent. Duration of treatment, however, is not defined.
No figures are available for the burden of mortality associated with neurocysticercosis. However, the racemose [12] form of this disease—which appears macroscopically as groups of cysticerci, often in clusters that resemble bunches of grapes located in the subarachnoid space—is associated with poor prognosis and elevated mortality rate (>20%).
Neurocysticercosis-associated epilepsy is an important cause of neurologic morbidity, [13] and chronic epilepsy is one of the most frequent complications of neurocysticercosis. Others include headaches, neurologic deficits related to strokes, and hydrocephalus. Patients with complications such as hydrocephalus, large cysts, multiple lesions with edema, chronic meningitis, and vasculitis are acutely ill and do not respond very well to treatment. Frequently, they have complications due to medical and surgical therapy.
Patient Education
Neurocysticercosis is a major public health problem in developing countries and is emerging as an increasingly important condition in regions in which the disease is not endemic. Comprehensive programs of long-term intervention involve appropriate legislation, health education, modernization of swine husbandry practices, improvement of efficiency and coverage of meat inspection, provision of adequate sanitary facilities, and measures to detect and treat human tapeworm carriers.
Political and economic realities in many communities where T solium is endemic today provide little hope that all these goals can be achieved in the near future. However, short-term approaches can be effective in the long-term, and these include educational campaigns in personal hygiene and general sanitation within the disease-endemic area.
Note that the usual restrictions for patients with epilepsy would be applicable for patients with neurocysticercosis presenting with seizures.
-
Massive nonencephalitic neurocysticercosis. Photo courtesy of Cysticercosis Working Group in Peru.
-
Computed tomographic (CT) scan of the brain in a patient who presented with an episode of generalized tonic-clonic seizure. Note the calcified lesion in the left parieto-occipital region. Subsequent evaluation confirmed the diagnosis of neurocysticercosis.
-
T2-weighted magnetic resonance image (MRI) of the brain showing the presence of increased signal as a result of edema in the right frontal region; subsequent studies found a cysticercus in that location.
-
Magnetic resonance image (MRI) of the brain in a patient who presented with an episode of generalized tonic-clonic seizure. Note the cyst in the left parieto-occipital region with perilesional edema.






