Practice Essentials
Acute glomerulonephritis following streptococcal infection is a type III hypersensitivity reaction characterized by the sudden appearance of hematuria, proteinuria, red blood cell casts in the urine, edema, and hypertension with or without oliguria. [1, 2, 3] (See the image below.) Poststreptococcal glomerulonephritis was first recognized as a complication of the convalescence period of scarlet fever in the 18th century. [4] A link between hemolytic streptococci and acute glomerulonephritis was recognized in the 20th century.
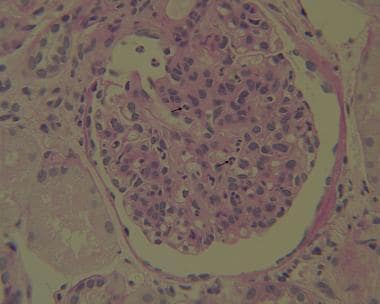 Kidney biopsy from a 7-year-old child with acute poststreptococcal glomerulonephritis. Periodic acid–Schiff stain (at 40x) shows the intracapillary and occasional mesangial neutrophil (arrows). Courtesy of Laura Kidd, MD, Pathology and Laboratory Medicine, Tulane University Medical School.
Kidney biopsy from a 7-year-old child with acute poststreptococcal glomerulonephritis. Periodic acid–Schiff stain (at 40x) shows the intracapillary and occasional mesangial neutrophil (arrows). Courtesy of Laura Kidd, MD, Pathology and Laboratory Medicine, Tulane University Medical School.
Although the incidence of poststreptococcal glomerulonephritis has declined in the United States, it remains high in other parts of the world, especially in areas with tropical climates where skin infections are common. [5, 6]
The workup in patients with suspected acute poststreptococcal glomerulonephritis includes tests to provide evidence of preceding streptococcal infection, kidney function studies, and serologic studies (see Workup). The major goal of treatment is to control edema and blood pressure (see Treatment and Medication).
See also Acute Poststreptococcal Glomerulonephritis, Acute Glomerulonephritis, and Emergent Management of Acute Glomerulonephritis.
Pathophysiology
Poststreptococcal glomerulonephritis follows infection with only certain strains of streptococci, designated as nephritogenic. The offending organisms have virtually always been group A streptococci. Acute poststreptococcal glomerulonephritis (APSGN) follows pyodermatitis with group A streptococci that have the surface antigen M protein types 47, 49, 55, 2, 60, and 57 and throat infection with streptococci that have M types 1, 2, 4, 3, 25, 49, and 12. Less often, group C streptococci (ie, Streptococcus zooepidemicus) may be involved. [7]
Many morphologic, clinical, and serologic features suggest that APSGN is an immune complex disorder in which an immune complex containing a streptococcal antigen is deposited in the affected glomeruli. The size of glomerular basement membrane (GBM) pores and the molecular size of the streptococcus-Ig complex are also important determinants. The molecular size of the streptococcus-Ig complex is about 15 nm (10 nm for streptococcus group A and 5 nm for immunoglobulin). The GBM pore sizes in children and adults are 2-3 nm and 4-4.5 nm, respectively. Therefore, the immune complex molecule can be more easily rodded into the glomerulus in children than in adults and, thus, may explain the higher frequency of APSGN in children than in adults.
Stamatiades et al determined that in PSGN and other type III hypersensitivity reactions, vascular endothelial cells in the kidney actively transport circulating immune complexes from the capillaries to the peritubular interstitial space, where they are detected and scavenged by resident macrophages. Uptake of the immune complexes by the resident macrophages triggers the release of pro-inflammatory cytokines, which in turn results in recruitment of monocytes and neutrophils into the kidney from the circulation. [8]
Two antigens isolated from nephritogenic streptococci are commonly implicated in APSGN: streptococcal pyrogenic exotoxin B (SPEB) and nephritis-associated plasmin receptor (NAPlr). [9, 10] Both SPEB and NAPlr bind plasmin, protecting it from physiological inhibitors, and thus could cause chemotaxis of inflammatory cells and degradation of glomerular basement membranes. Both can be found in the glomeruli of APSGN tissues [10] .
In addition to streptococcal antigens, rheumatoid factor, cryoglobulins, and antineutrophil cytoplasmic serum antibodies are present in some of these patients. The pathogenic significance of this autoimmune response is not defined.
There are also host susceptibility factors. In one study, HLA-DRB1*03011 was reported to be found at a significantly higher frequency in 32 unrelated patients with APSGN as compared to 380 healthy individuals. [11]
Etiology
Acute poststreptococcal glomerulonephritis (APSGN) follows infection with only certain strains of streptococci designated as nephritogenic. The offending organisms are virtually always group A streptococci. APSGN follows pyodermatitis with streptococci M types 47, 49, 55, 2, 60, and 57 and throat infection with streptococci M types 1, 2, 4, 3, 25, 49, and 12.
Less commonly, group C streptococcal infection may result in APSGN. Clusters of cases linked to infection with Streptococcus zooepidemicus have occurred in Brazil, England, and Romania. S zooepidemicus is an emerging opportunistic pathogen that is part of the normal respiratory and intestinal flora of horses. [12]
Epidemiology
The incidence of clinically detectable glomerulonephritis during an epidemic is up to 10% of children with pharyngitis and 25% of children with impetigo. One study reported a change in the epidemiology of APSGN and found that pharyngitis has replaced impetigo as the predominant cause of APSGN. [13]
APSGN can occur sporadically or epidemically. The incidence seems to be decreasing in the United States and Europe, but sporadic cases of the disease continue to be reported from all over the world. The prevalence of nephritis varies considerably among persons with sporadic infections with nephritogenic streptococci. The reason for this variability is not known.
A systematic review by Jackson et al demonstrated significant variation in the global incidence of APSGN, with the highest incidence of 239 per 10,000 in Australian Aborigines and lowest incidence of 0.04 in 100,000 in an Italian study of people younger than 60 years. [14]
Epidemic poststreptococcal glomerulonephritis occurs mainly in developing countries in areas such as Africa, the West Indies, and the Middle East. Reasons for this changing epidemiology relate to the nutritional status of the community, the more liberal use of antibiotic prophylaxis, and possibly the change in the nephritogenic potential of streptococci. Among epidemic infections with nephritogenic streptococci, the apparent clinical attack rate is 10-12%. [5, 6]
Studies suggest that indigenous populations—including Native Americans, Pacific Islanders, and Aboriginal Australians—have increased susceptibility to APSGN. Limm-Chan and colleagues reported that Hawaii has a higher incidence of APSGN (4 cases per 100,000 population) than most developed countries. Of the reported cases, 62% were in Pacific Islanders, although they represent only 10% of the population. [15] In a study of 322 cases of APSGN in Australia, 94% were among Aboriginal Australians, who make up 30% of the population. [16]
Clinical cases of APSGN are twice as common in males than in females. If subclinical disease is considered, both sexes are affected equally. The familial incidence rate is nearly 40%, but no genetic marker has been identified. This condition typically affects children aged 2-12 years. A large series reported that 5% of patients are younger than 2 years and 10% are older than 40 years.
Prognosis
In children, the immediate prognosis is excellent. [5] Early death is extremely rare in children (< 1%) but is significantly more common in adults (25%). This is secondary to congestive heart failure and azotemia. Congestive heart failure is more common in adults (43%) than in children (< 5%). Nephrotic-range proteinuria is also more common in adults (20%) than in children (4-10%). Approximately 83% of adults have azotemia, compared with 25-40% of children.
Six cohort studies report case fatality rates from APSGN, with three revealing a case fatality rate of 0%, two studies from India reporting a case fatality rate of 1.4% and 2%, and one study from Turkey reporting a case fatality rate of 0.08%. [14]
The long-term prognosis is debatable. Fewer than 1% of children have elevated serum creatinine values after 10-15 years of follow-up. Adults who develop massive proteinuria often have the garlandlike pattern of immune deposits. Their prognosis is worse; approximately 25% progress to chronic kidney disease.
Adult patients with type 2 diabetes mellitus also have a worse prognosis . Case reports describe lack of remission, with continued hematuria and proteinuria resulting in end-stage renal disease. [17]
The long-term prognosis of children with APSGN has been the subject of several studies. Pooled data of studies published prior to 2000 with 5- to 18-year follow-up indicate abnormal urinalysis in 17.4%, proteinuria in 13.8%, hypertension in 13.8%, and azotemia in 1.3%. [18] A study from Australia demonstrated that APSGN can add to the burden of chronic kidney disease. [19] Araki and colleagues reported a case in a 15-year old boy with Alport syndrome that accelerated to end-stage kidney disease 15 months after the onset of APSGN. [20]
Group C streptococcal infection, although rare, has a worse prognosis for adults. A 20-year follow-up of 47 adult patients with APSGN following group C streptococcal infection reported a high rate of hypertension (72%) and chronic kidney disease (53%). [21]
Complications in the acute phase include the following:
-
Congestive heart failure
-
Azotemia
-
Early death secondary to congestive heart failure and azotemia
Complications in the chronic phase include the following:
-
Nephrotic-range proteinuria
-
Chronic kidney disease and end-stage renal disease
Patient Education
Patients with skin infections should know the importance of personal hygiene. In epidemics, all close personal contacts and family members should be told to seek medical attention for prophylactic treatment of streptococcal infections.
For patient education resources, see Blood in the Urine (Hematuria) and Strep Throat.
-
Kidney biopsy from a 7-year-old child with acute poststreptococcal glomerulonephritis. Periodic acid–Schiff stain (at 40x) shows the intracapillary and occasional mesangial neutrophil (arrows). Courtesy of Laura Kidd, MD, Pathology and Laboratory Medicine, Tulane University Medical School.
-
Kidney biopsy from a 7-year-old child with acute poststreptococcal glomerulonephritis. Periodic acid–Schiff stain (at 40x) shows the intracapillary and occasional mesangial neutrophil (arrows). Courtesy of Laura Kidd, MD, Pathology and Laboratory Medicine, Tulane University Medical School.
-
Kidney biopsy from a 7-year-old child with acute poststreptococcal glomerulonephritis. Electron microscopy image shows rare large subepithelial deposits, or “humps” (arrows). Courtesy of Laura Kidd, MD, Pathology and Laboratory Medicine, Tulane University Medical School.
-
Kidney biopsy from a 7-year-old child with acute poststreptococcal glomerulonephritis. Electron microscopy image shows rare large subepithelial deposits, or “humps” (arrows). Courtesy of Laura Kidd, MD, Pathology and Laboratory Medicine, Tulane University Medical School.
-
Kidney biopsy from a 7-year-old child with acute poststreptococcal glomerulonephritis. Immunofluorescence (C3) shows a granular capillary and mesangial staining pattern with segmental areas of “lumpy-bumpy” staining (white arrows). Courtesy of Laura Kidd, MD, Pathology and Laboratory Medicine, Tulane University Medical School.






