Background
Endocardial cushion defects, more commonly known as atrioventricular (AV) canal or septal defects, include a range of defects characterized by involvement of the atrial septum, the ventricular septum, and one or both of the AV valves.
These defects can be classified by several methods. A distinction generally is made between partial and complete defects. A complete AV septal defect indicates the presence of both atrial and ventricular septal defects with a common AV valve (see image below). A partial defect indicates atrial septal involvement with separate mitral and tricuspid valve orifices.
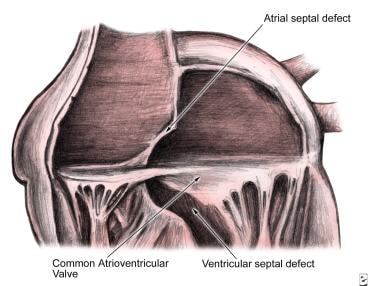 Endocardial Cushion Defects (Atrioventricular Canal Defects, Atrioventricular Septal Defects). Anatomy of the endocardial cushion defect (ie, complete form); note the common atrioventricular valve straddling the atrial septal and ventricular septal defects.
Endocardial Cushion Defects (Atrioventricular Canal Defects, Atrioventricular Septal Defects). Anatomy of the endocardial cushion defect (ie, complete form); note the common atrioventricular valve straddling the atrial septal and ventricular septal defects.
AV canal defects arise from abnormal development of the endocardial cushions. In these patients, the superior and inferior cushions do not close completely. An interatrial communication is left at the lower portion of the atrial septum. This is called an ostium primum defect. The failure of the endocardial cushions to fuse results in an abnormally low position of the AV valves and an abnormally high position of the aortic valve. A portion of the AV valves originates from the endocardial cushions, and their improper fusion results in anterior and posterior components to the mitral valve leaflet. [1]
Patient education
Parents must be instructed to ensure that antibiotic prophylaxis for dental procedures is instituted for the child. Good dental hygiene for the child is imperative.
Pathophysiology
Predominant left-to-right shunting of blood through the heart occurs in patients with endocardial cushion defects (atrioventricular [AV] canal or septal defects). In patients with partial defects, this occurs through the ostium primum atrial septal defect. When a complete endocardial cushion defect is present, a large ventricular septal defect as well as valvular insufficiency may develop, resulting in volume overload of both the left and right ventricles associated with heart failure in early life. In patients with long-standing pulmonary overload, pulmonary vascular disease may develop and congestive heart failure (CHF) symptoms may improve. This improvement is a poor prognostic indicator because it heralds the development of right-to-left shunting and irreversible pulmonary hypertension (ie, Eisenmenger syndrome). [2]
Etiology
Genetics
The characteristic pattern of the endocardial cushion defect (atrioventricular [AV] canal or septal defect) has been attributed to trisomy 21 and Down syndrome in some cases. Some evidence exists that a critical region of chromosome band 21q22 may contribute particularly to the cardiac malformation in this syndrome.
Other chromosomal abnormalities also can result in AV septal defects, in particular, deletion of 8p, partial 10q monosomy, partial 13q monosomy, ring 22 14 q+, and 1p+3p-.
In most cases of significant chromosomal aberration, AV septal defects are associated with other noncardiac congenital defects. However, isolated AV septal defects can be transmitted in families as an autosomal dominant trait.
Linkage analyses have suggested a locus for autosomal dominant AV septal defects on chromosome 1p but no specific gene defect has yet been identified.
Growth factor aberrations
In the developing fetus, cardiac tissue formation is dependent upon appropriate growth factor stimulation including transforming growth factor beta and platelet-derived growth factor. Alterations in the concentration or efficacy of these factors during embryogenesis can contribute to the cardiac malformations.
Epidemiology
United States data
The frequency rate of endocardial cushion defect (atrioventricular [AV] canal or septal defects) is about 3% of children with congenital heart disease. Sixty to seventy percent of these defects are of the complete form. More than half of those affected with the complete form have Down syndrome.
International data
The frequency rate is about 3% of children who have congenital heart disease. Data from a Canadian study indicated that by 2010, adults accounted for two thirds of patients with congenital heart disease in the general population. [3]
Race-, sex-, and age-related demographics
No racial predilection is apparent. Girls are affected slightly more frequently than boys.
Endocardial cushion defect is a congenital defect present at birth. The severity of the symptom complex and presentation is dependent directly upon the severity of the defect and the presence of mitral insufficiency.
Prognosis
The long-term results of surgical correction for endocardial cushion defect (atrioventricular [AV] canal or septal defect) depend upon the degree of preoperative pulmonary vascular disease and upon the amount of residual AV valve regurgitation. If the pulmonary vasculature is protected and the amount of valvular regurgitation is reduced substantially, prognosis is good. When severe pulmonary vascular disease is present preoperatively, morbidity and mortality rates are high. Complete heart block and arrhythmias may occur after correction, and their incidence increases with age. As the patient grows older, mitral valve replacement may be needed.
The surgical mortality rate in patients with partial endocardial cushion defects is 0-6%, while that for the complete defect ranges from 3-10%.
Morbidity/mortality
Patients with only ostium primum atrial septal defect and minimal insufficiency of the left AV valve (ie, mitral valve) do well without treatment during infancy, childhood, and adolescence. During adulthood, these patients develop symptoms of CHF and atrial arrhythmia.
Patients with septal defects and mitral valve insufficiency develop CHF early in life, with high rates of morbidity and mortality if the valvular insufficiency is pronounced. Patients with a complete defect develop CHF in infancy, with frequent respiratory infections and poor weight gain.
The American Heart Association issued recommendations intended to optimize the neurodevelopmental outcomes of children with congenital heart disease. [4] The recommendations included (1) using the medical home model of care to manage children with chronic conditions (eg, congenital heart disease) and to stratify them by risk (low and high) for neurodevelopmental disorder/disability at every medical home visit; (2) following the AAP guidelines for screening/surveillance, evaluation, and intervention in children with congenital heart disease; and (3) referral for patients at high risk of neurodevelopmental disorder/disability to formal developmental and medical evaluation as well as early intervention/childhood special education services. [4]
Complications
Since synthetic material is used to repair the atrial and ventricular septal defect, the child is at risk of infection. Other potential complications include complete heart block, ventricular arrhythmia, and AV valve stenosis and/or insufficiency.
-
Endocardial Cushion Defects (Atrioventricular Canal Defects, Atrioventricular Septal Defects). Anatomy of the endocardial cushion defect (ie, complete form); note the common atrioventricular valve straddling the atrial septal and ventricular septal defects.
-
Endocardial Cushion Defects (Atrioventricular Canal Defects, Atrioventricular Septal Defects). Repair of the endocardial cushion defect. The patch is covering the ostium primum atrial septal defect.





