Practice Essentials
Norovirus, formerly referred to as Norwalk virus, is a very contagious virus that causes acute gastroenteritis. People of all ages can get infected and sick with norovirus. The most common symptoms of norovirus are diarrhea, vomiting, nausea, and stomach pain. Other symptoms include fever, headache, and body ache. About 50% of cases of foodborne gastroenteritis in United States are caused by norovirus. Worldwide, about 1 out of every 5 cases of acute gastroenteritis is caused by norovirus.
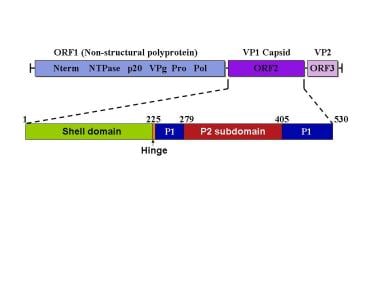
The image below depicts the norovirus genomic structure and capsid domains.
Signs and symptoms
Symptomatic norovirus gastroenteritis typically develops 12-48 hours after ingestion of contaminated food or water or after contact with an infected individual. Symptoms typically last for 24-72 hours.
Symptoms include the following:
-
Nausea and vomiting (profuse, nonbloody, nonbilious)
-
Watery diarrhea (nonbloody)
-
Abdominal cramps
-
Headaches
-
Low-grade fever
-
Myalgias and malaise
Focal tenderness and peritoneal signs are absent in abdominal examination. Vital signs in norovirus gastroenteritis include the following:
-
Low-grade fever
-
Tachycardia
-
Possible hypotension with volume depletion
See Clinical Presentation for more detail.
Diagnosis
Laboratory studies
Norovirus infection can be detected via the following studies:
-
Immune electron microscopy: Immune serum is used to aggregate virus in stool samples to aid detection
-
Antigen detection immunoassay: Has high sensitivity but low specificity because of reactivity with antigenic variants and homologous viruses
-
Nucleic acid amplification: Highly sensitive and specific [1]
Serum antibody titers can be detected within 2 weeks of illness. During norovirus infection, immunoglobulin M (IgM) to norovirus has been found to be more specific than IgG. [2]
Imaging studies
Imaging for isolated, uncomplicated gastroenteritis is not required. In patients with severe symptoms in whom acute abdomen is suspected and in those with preexisting disorders such as inflammatory bowel disease, abdominal radiography or computed tomography scanning should be performed.
New strain
In January 2013, the US Centers for Disease Control and Prevention (CDC) reported that a new norovirus strain, GII.4 Sydney, which was first detected in Australia, had spread to the United States. During the last 4 months of 2012, GII.4 Sydney accounted for 53% of 266 norovirus outbreaks in the United States, with roughly half of them having resulted from direct person-to-person transmission and another 20% having been foodborne. In general, GII.4 strains are associated with higher rates of hospitalization and death. [3, 4]
See Workup for more detail.
Management
Treatment of norovirus gastroenteritis includes the following:
-
Oral fluid and electrolyte replacement: Generally adequate for the treatment of norovirus infections
-
Intravenous fluid and electrolyte resuscitation: May be necessary in cases of severe volume depletion
-
Antiemetics: For relief of nausea and vomiting
-
Analgesics: For relief of myalgias and headache
-
Antiperistaltic agents: Should generally be avoided in cases of infectious diarrhea but can be considered in patients with severe diarrhea
See Treatment and Medication for more detail.
Background
Norwalk virus was officially renamed norovirus by the International Committee on Taxonomy of Viruses in 2002. The virions contain a single-stranded RNA molecule in round to hexagonal capsids that are 35-39 nm in diameter, with icosahedral symmetry. The surface structure of the capsid is a regular pattern with distinctive features and 32 cup-shaped depressions. [5, 6]
Norovirus was first recognized as a cause of gastroenteritis in 1972, when it was detected in stool samples collected from infected elementary school students and contacts during an outbreak in Norwalk, Ohio, in 1968. It was declared a member of the Caliciviridae family of viruses in 1993. [7] It now is considered the most common cause of epidemic nonbacterial gastroenteritis in the world.
In the 1970s and 1980s, typing of Norwalk-like virus (NLV) relied solely on immunologic methods involving human clinical samples as the source of antigens and antibodies. These methods had serious limitations in accuracy and reproducibility and never provided a reliable scheme for antigenic classification of strains. In the 1990s, however, newer molecular techniques to amplify, sequence, and express the genome of NLV strains allowed researchers to genetically and antigenically characterize NLV strains. [8]
The norovirus genus contains more than 40 different strains that are divided into 5 genogroups based on sequence similarity. Viruses in genogroups I, II, and IV are primarily human pathogens, although genogroup II contains a porcine-specific virus. Viruses in genogroup III and V infect bovine and murine species, respectively. Each genogroup is further subdivided into genoclusters based on sequence similarity. [9]
The genome consists of single-stranded RNA of 7.3-7.7 kilobases. It encodes 3 open reading frames (ORFs). ORF 1 is the largest (approximately 1700 amino acids) and expressed as a nonstructural polyprotein precursor that is cleaved by the viral 3C-like protease. ORF 2 encodes the viral capsid (550 amino acids) and contains the shell and protruding domains. ORF 3 encodes a small basic protein of unknown function. See the image below.
Pathophysiology
Noroviruses are transmitted person to person via direct contact, exposure to aerosols, or fecal–oral routes. Noroviruses are highly contagious, with infection requiring fewer than 10 virions (ID50 = 10 virions), leading to disease in 50% of inoculated individuals. The virus is extremely stable in the environment and resists freezing temperatures, heat (up to 60°C), disinfection with chlorine, acidic conditions, vinegar, alcohol, antiseptic hand solutions, and high sugar concentrations. The incubation period is approximately 1-2 days, and symptoms typically last 1-3 days (or longer in immunocompromised individuals). Viral shedding occurs for up to 3 weeks following infection. [10]
Noroviruses bind polymorphic histoblood group antigens (HBGAs) that putatively serve as receptors or cofactors for infection. Strains from different genoclusters bind various HBGAs: Genogroup I viruses preferentially bind blood group A and O antigens, while genogroup II viruses predominantly bind A and B antigens. [11] Individual norovirus strains may be capable of infecting only a subset of the human population, although the diverse binding profiles found within genogroup I and genogroup II viruses likely collectively make nearly all individuals susceptible to norovirus infection. [10] Recurrent infections can occur throughout life because of the great diversity of norovirus strains and the lack of cross-strain or long-term immunity.
Infection is characterized by damage to the microvilli in the small intestine. Upon microscopic investigation, villi are found to be blunted, although the mucosa and epithelium remain intact. [12] A recent study demonstrated increased epithelial cell apoptosis and damage to tight junction proteins. [13] Diarrhea is induced by D-xylose and fat malabsorption, with enzymatic dysfunction observed at the brush border, along with leak flux and anion secretion. [13, 14] Vomiting is related to virus-mediated changes in gastric motility and delayed gastric emptying. Notably, no histopathologic lesions can be identified in the gastric mucosa of infected patients. [15] Noroviruses do not invade the colon, so fecal leukocytes typically are absent, and hematochezia is rare.
Epidemiology
Frequency
United States
According to a Centers for Disease Control and Prevention (CDC) report updated in March 2021, most norovirus outbreaks in the United States happen from November to April. In years when there is a new strain of the virus, there can be 50% more norovirus illness.
Each year, on average in the United States, norovirus causes [41] :
-
900 deaths, mostly among adults aged 65 and older
-
109,000 hospitalizations
-
465,000 emergency department visits, mostly in young children
-
2,270,000 outpatient clinic visits annually, mostly in young children
-
19 to 21 million cases of vomiting and diarrhea illnesses
Multistate outbreak of norovirus illnesses linked to raw oysters from Texas has been reported as of April 11, 2023. [40] Another multistate outbreak of norovirus illnesses linked to raw oysters from British Columbia was reported as of June, 2022.
Outbreaks have been reported in restaurants, health care facilities, schools, resorts, cruise ships, military ships, and barracks. Viral transmission occurs year-round, with a higher incidence of disease in winter months in temperate climates. [18]
International
Data regarding outbreaks in developing nations are not well quantified, but the outbreak rate in other industrial nations is similar to that of the United States.
Mortality/Morbidity
Norovirus gastroenteritis typically lasts 24-72 hours, with remission occurring without sequelae. Death is extremely rare, except in individuals particularly vulnerable to profound volume depletion.
Age
Norovirus gastroenteritis can occur in individuals of all ages. Studies using norovirus recombinant antigen have suggested an increase in antibody prevalence with advancing age. In 1 study, the prevalence of norovirus immunoglobulin G (IgG) rose during school-aged years, reaching a peak of 70% in persons aged 11-16 years. [19] It should be noted, however, that not all infected individuals sustain detectable antibody responses.
Prognosis
Norovirus gastroenteritis is a self-limiting disease with an excellent prognosis in otherwise healthy individuals.
Patient Education
Patients with norovirus infection should be educated on personal and environmental hygiene, including avoiding/eliminating contaminated foods and water. Ill individuals should refrain from attending school or work.
-
Hematoxylin and eosin stain of duodenal epithelium.
-
The norovirus genomic structure and capsid domains.






