Background
Nocardiosis is an acute, subacute, or chronic infectious disease that occurs in cutaneous, pulmonary, and disseminated forms. Primary cutaneous nocardiosis manifests as cutaneous infection (cellulitis or abscess), lymphocutaneous infection (sporotrichoid nocardiosis), or subcutaneous infection (actinomycetoma). Pleuropulmonary nocardiosis manifests as an acute, subacute, or chronic pneumonitis, usually in immunocompromised hosts, although isolated cases have been reported in immunocompetent hosts. Disseminated nocardiosis may involve any organ however, lesions in the brain or meninges are most common.
Pathophysiology
Members of the genus Nocardia are aerobic actinomycetes that are ubiquitous saprophytes in soil, decaying organic matter, and fresh and salt water. Over 100 species of the genus Nocardia have been identified, more than half of which have been described during the last decade.
The taxonomy has been challenging and likely remains in evolution. [1, 2] Most human infections are due to members of the formerly called Nocardia asteroides complex. N asteroides complex was later separated into Nocardia abscessus, Nocardia brevicatena-paucivorans complex , Nocardia nova complex, Nocardia transvalensis complex, Nocardia farcinica, Nocardia asteroides sensu stricto, and Nocardia cyriacigeorgica; however, use of the term " N asteroides complex" is currently outdated because of the heterogenous group of organisms it includes. Nocardia species also cause infections in animals, including bovine mastitis and sporotrichoid nocardiosis in horses.
When observed microscopically, either in Gram-stained smears of clinical specimens or cultures or on histopathology in tissues, Nocardia organisms are delicate, branching, beaded, filamentous, gram-positive bacteria with a characteristic morphology to a trained observer.
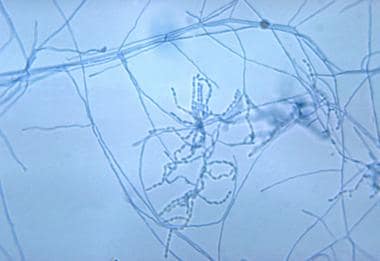
Nocardia are typically weakly acid-fast after traditional staining and positive on modified acid-fast staining, but this is not invariable.
The cutaneous, lymphocutaneous, and subcutaneous forms of nocardiosis arise from local traumatic inoculation. These infections are not necessarily associated with immunocompromised host states, but dissemination from these sites of inoculation is more likely in immunocompromised hosts, particularly those with impaired cell-mediated immunity. [3] Pleuropulmonary nocardiosis presumably arises from inhalation exposure. Disseminated nocardiosis results from hematogenous dissemination, usually from a pulmonary focus. Most persons with disseminated nocardiosis have underlying immunocompromising disease or are receiving immunosuppressive therapy.
Nocardiosis produces suppurative necrosis with frequent abscess formation at sites of infection.
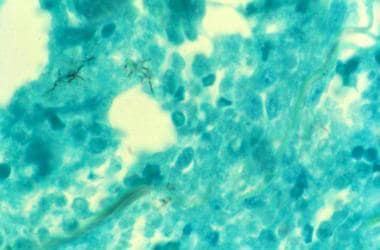 Photomicrograph of tissue biopsy stained with Gomori methenamine silver demonstrating acute inflammatory response and organisms compatible with Nocardia.
Photomicrograph of tissue biopsy stained with Gomori methenamine silver demonstrating acute inflammatory response and organisms compatible with Nocardia.
Disease manifestations of nocardiosis are determined by strain characteristics, inoculation site, tissue tropism, ability to survive initial neutrophilic leukocyte phagocytic attack, and the nature of the immune response. T-cell–mediated immunity is the principal protective immune response to nocardiosis. [3] Therefore, nocardiosis is most problematic in individuals with impaired T-cell–mediated immunity. [2]
Epidemiology
Frequency
United States
The estimated incidence of nocardiosis in the United States is 500-1000 cases per year. [4]
Clusters of nocardiosis have been described in hospitalized patients, related to contaminated fomites from construction or contaminated hands of staff.
International
No reliable estimates on the international frequency of nocardiosis are available.
Mortality/Morbidity
Nocardiosis has a variable prognosis, depending on the site of infection, extent of infection, and underlying host factors. [5]
Cure rates with appropriate therapy are approximately 100% in skin and soft-tissue infections.
Up to 90% percent of pleuropulmonary infections can be cured with appropriate therapy.
The cure rate in disseminated nocardiosis falls to 63%, while only half of the patients with brain abscess can be cured with therapy. [6]
Race
Nocardiosis has no apparent racial predilection.
Sex
Nocardiosis is more common in males than in females, with a male-to-female ratio of 3:1. This difference is likely related to exposure frequency rather than a gender difference in susceptibility.
Age
All ages are susceptible to nocardiosis. The mean age at diagnosis is in the fourth decade of life.
Prognosis
The one-year rate for all-cause mortality from nocardiosis in both immunocompetent and immunocompromised patients has been found to be 19-22%. [7, 8] Poor prognostic factors in nocardiosis patients are Nocardia CNS infections, recipients of solid-organ transplants, HIV/AIDS with advanced immunocompromised state, delayed diagnosis, and premature discontinuation of antimicrobial therapy. [9, 8]
Patient Education
Patients with nocardiosis must be educated about the need for protracted antimicrobial therapy.
Patients with nocardiosis should be informed of the potential adverse effects of protracted antimicrobial therapy and which circumstances require reporting to their physician promptly.
-
High-power microscopic appearance of Nocardia. Image courtesy of CDC.
-
Photomicrograph of tissue biopsy stained with Gomori methenamine silver demonstrating acute inflammatory response and organisms compatible with Nocardia.
-
Plain chest radiograph in a patient with nocardiosis. Image courtesy of Applied Radiology, Anderson Publishing, LTD.
-
Chest CT scan in a patient with pleuropulmonary nocardiosis. Image courtesy of Applied Radiology, Anderson Publishing, LTD.
-
Brain CT scan in a patient with nocardial brain abscess. Image courtesy of Applied Radiology, Anderson Publishing, LTD.





