Practice Essentials
Myelophthisis is a form of bone marrow failure that results from the destruction of bone marrow precursor cells and their stroma, which nurture these cells to maturation and differentiation.
Infiltrating lesions caused by nonhematopoietic cells invading bone marrow can result in varying degrees of cytopenia, including anemia, thrombocytopenia, neutropenia, and pancytopenia. [1] Bone marrow failure resulting from secondary infiltration is a possible cause of lack of blood cell production (as differentiated from a primary cause of failure). Manifestations range from a leukoerythroblastic picture [2] to the presence of a few teardrop-shaped red blood cells and early myeloid precursor cells in the peripheral blood smear. [3] (See the image below.) (See Etiology, Differentials, and Workup.)
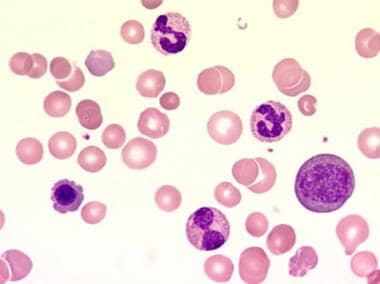 This blood film at 1000X magnification demonstrates a leukoerythroblastic blood picture with the presence of precursor cells of the myeloid and erythroid lineage. In addition, anisocytosis, poikilocytosis, and polychromasia can be seen. Courtesy of Ulrich Woermann, MD, Division of Instructional Media, Institute for Medical Education, University of Bern, Switzerland.
This blood film at 1000X magnification demonstrates a leukoerythroblastic blood picture with the presence of precursor cells of the myeloid and erythroid lineage. In addition, anisocytosis, poikilocytosis, and polychromasia can be seen. Courtesy of Ulrich Woermann, MD, Division of Instructional Media, Institute for Medical Education, University of Bern, Switzerland.
The most common causes of infiltrative myelopathy are as follows:
-
Lymphoproliferative malignancies (eg, lymphomas)
-
Disseminated granulomatous diseases (eg, miliary tuberculosis) [6]
-
Rare diseases (eg, Gaucher disease)
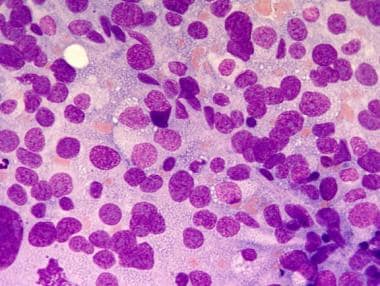 This bone marrow film at 400X magnification demonstrates carcinoma metastasis. Bone marrow cells are completely replaced by large carcinoma cells with clear nucleoli. Courtesy of Ulrich Woermann, MD, Division of Instructional Media, Institute for Medical Education, University of Bern, Switzerland.
This bone marrow film at 400X magnification demonstrates carcinoma metastasis. Bone marrow cells are completely replaced by large carcinoma cells with clear nucleoli. Courtesy of Ulrich Woermann, MD, Division of Instructional Media, Institute for Medical Education, University of Bern, Switzerland.
Go to Anemia, Chronic Anemia, Megaloblastic Anemia, Hemolytic Anemia, and Sideroblastic Anemias for complete information on these topics.
Etiology
Generally, in myelophthisic anemia, a form of fibrosis, occurs secondary to injury by nonhematopoietic cells or pathogens. This fibrosis destroys the normal hematopoietic cells and their supportive stromal cells. The bone marrow becomes infiltrated by collagen, reticulin, and other forms of fibrosis, which replace the normal, hematopoietic cells. The most common causes of extensive bone marrow infiltrative damage or invasion without much structural damage are discussed below. The expanding number and volume of pathologic cells and the release of suppressive cytokines can eventually lead to bone marrow failure without the characteristic morphologic features of myelophthisis.
Leukemic cells, such as those occurring in chronic leukemias in which the expanding cells are mature and coexist peacefully with the normal bone marrow cells, show no evidence of myelophthisis, and marrow damage does not occur.
In agnogenic and secondary myelofibrotic disorders, megakaryocytes release platelet-derived growth factors, which are fibroblastic stimulants for growth and proliferation. This leads to the consequences of bone marrow space reduction and to disruption of normal bone marrow architecture.
Agnogenic myeloid metaplasia is a stem cell abnormality associated with myeloproliferative diseases. It is related to an abnormal stem cell clone that stimulates increased myelofibrosis and damage. It progresses to acute leukemia and is associated with extramedullary hematopoiesis in the liver and spleen, causing hypertrophy of these organs.
Secondary myelofibrosis is due to implantation or invasion by malignant cancer cells that have metastasized because of implantation of blood-borne tumor cells from a distant cancer. The most common sources are cancers of the lung, breast, and prostate [7] and sarcomas.
Nonmalignant causes of myelophthisis include the following:
-
Inflammatory cells, miliary tuberculosis, and fungal infections
-
Macrophage proliferation in storage diseases, such as Gaucher disease
-
Necrosis in sickle cell disease and septicemia
-
Bone disease in congenital osteopetrosis
With regard to Gaucher disease, infiltration by cells with "onion-peel" cytoplasm, called Gaucher cells, is caused by a lipid storage disorder (ie, glucosylceramide lipidosis). Gaucher cells clog or infiltrate the bone marrow, spleen, and liver. This disorder is inherited.
Myelophthisic anemia may also be triggered by severe cobalamin deficiency. [8]
Epidemiology and Prognosis
Myelophthisis is observed more frequently in countries where access to medical care is difficult and diseases are allowed to progress to advanced stages. In the United States, infiltrative myelopathy occurs in less than 10% of cancer patients with metastatic disease.
Mortality is dependent on the underlying condition. [5] The leukoerythroblastic blood picture is often associated with imminent death in some extreme cases. Patients with varying degrees of cytopenia are at risk for infection or bleeding.
-
This blood film at 1000X magnification demonstrates a leukoerythroblastic blood picture with the presence of precursor cells of the myeloid and erythroid lineage. In addition, anisocytosis, poikilocytosis, and polychromasia can be seen. Courtesy of Ulrich Woermann, MD, Division of Instructional Media, Institute for Medical Education, University of Bern, Switzerland.
-
This bone marrow film at 400X magnification demonstrates carcinoma metastasis. Bone marrow cells are completely replaced by large carcinoma cells with clear nucleoli. Courtesy of Ulrich Woermann, MD, Division of Instructional Media, Institute for Medical Education, University of Bern, Switzerland.







