Background
Microsporidiosis (also known as microsporidiasis) is caused by infection with microsporidia, which are obligately intracellular, spore-forming parasites that belong to the phylum Microspora and the order Microsporida. Microsporidia are eukaryotic organisms that contain 70S ribosomes but lack mitochondria, peroxisomes, Golgi membranes, and other typically eukaryotic organelles. The phylum Microspora contains over 1700 species. [1] They are ubiquitous organisms with an extensive host range, particularly rodents [2] alongside honeybees, fish, mosquitoes, ticks, grasshoppers, rabbits, dogs, and other fur-bearing mammals. [3] Species identified as causing microsporidiosis in humans include the following:
-
Enterocytozoon bieneusi
-
Encephalitozoon hellem
-
Encephalitozoon intestinalis (previously Septata intestinalis)
-
Encephalitozoon cuniculi
-
Pleistophora species
-
Trachipleistophora hominis
-
Trachipleistophora anthropophthera
-
Nosema bombycis
-
Nosema connori (as seen in the image below)
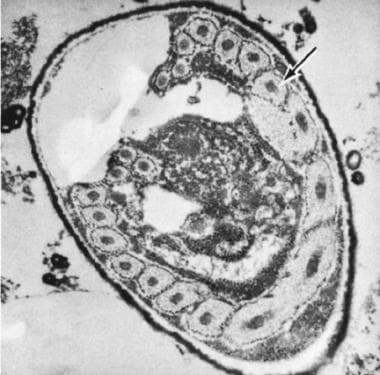 Electron micrograph (X30,000) of Nosema connori in diaphragm showing a coiled polar filament (arrow). Courtesy of the Armed Forces Institute of Pathology (AFIP 71-11521-4).
Electron micrograph (X30,000) of Nosema connori in diaphragm showing a coiled polar filament (arrow). Courtesy of the Armed Forces Institute of Pathology (AFIP 71-11521-4).
-
Nosema ocularum
-
Brachiola vesicularum
-
Vittaforma corneae (previously Nosema corneum)
-
Microsporidium ceylonensis
-
Microsporidium africanum
-
Brachiola algerae

Currently, most cases of human microsporidiosis are associated with HIV infection or other forms of immunosuppression, particularly in organ transplant recipients and those undergoing chemotherapy; however, cases have been reported in immunocompetent individuals. [4, 5, 6] Bukreyeva et al reported 2 cases of E bieneusi microsporidiosis in patients who had undergone allogeneic hematopoietic stem cell transplantation. Fumagillin treatment was successful in both cases. [7]
See Common Intestinal Parasites, a Critical Images slideshow, to help make an accurate diagnosis.
Pathophysiology
Humans acquire microsporidiosis through ingestion or inhalation of microsporidia spores. Studies have isolated Encephalitozoon species in the urinary tract in those with disseminated infections, suggesting that sexual transmission is possible. The spore is the infective form. Spores are environmentally resistant and are surrounded by an outer electron-dense glycoprotein layer and an electron-lucent endospore layer composed primarily of chitin. The spore extrudes its polar tubule and injects the infective sporoplasm into the host cell. Once inside the cell, it multiplies by binary fission or schizogony. Development can occur directly inside the host cell cytoplasm or inside parasitophorous vacuoles. As mature spores develop and accumulate, the cell expands and eventually ruptures, releasing the spores.
Epidemiology
Frequency
United States
Currently, most cases of microsporidiosis are reported in immunosuppressed adults, especially those with HIV-related immunosuppression. Studies have found that E bieneusi infection of small intestinal enterocytes is detected in 15-34% of patients with AIDS with chronic diarrhea and no other identified causes.
E bieneusi infection also has been found in renal transplant recipients with chronic weight loss and diarrhea. [5] A case of fatal myositis due to B algerae infection has been documented in a woman with diabetes and rheumatoid arthritis who had been prescribed infliximab. [8, 9, 10]
International
Microsporidia have a worldwide distribution. Cases of microsporidiosis have been reported in both developed and developing countries and among both immunosuppressed and immunocompetent individuals. Microsporidiosis has been reported in the Americas, Asia, Europe, and Africa.
Mortality/Morbidity
Clinical symptoms and manifestations of microsporidiosis depend on the infecting species and the host's immune status. Microsporidial keratoconjunctivitis has been identified in healthy immunocompetent individuals, and the use of topical steroids may have been the initial predisposing factor in 1 case series. [11] The individuals in this case series exhibited unilateral punctate epithelial involvement of the cornea. V corneae infection was identified as a cause of unilateral stromal keratitis in a case report by Font et al, and topical steroid use had preceded the diagnosis. [12]
Bilateral punctate epithelial involvement of the cornea is the typical manifestation of ocular microsporidiosis in immunocompromised individuals.
Most cases of intestinal and disseminated microsporidiosis in patients infected with HIV are reported in those who are severely immunocompromised (CD4 < 100/µL); in these patients, morbidity can be significant. E bieneusi infections often result in protracted debilitating illness with diarrhea, which may last several months. E bieneusi infections carry a mortality of up to 56%. In addition to chronic diarrhea, malabsorption and wasting can occur in persons with AIDS. E bieneusi is responsible for more than 90% of intestinal microsporidiosis cases in this population; E intestinalis accounts for the remainder.
Reports of E bieneusi infections are increasing among travelers and residents of tropical countries who do not have HIV infection. E intestinalis infection associated with chronic diarrhea has been reported in immunocompetent travelers.
E bieneusi usually is found only in enterocytes. E intestinalis is more invasive and produces disseminated disease involving the small and large intestines, gallbladder, urinary tract epithelium, and respiratory tract epithelium. Biliary tract involvement that progresses to cholangitis and cholecystitis is common in patients with AIDS who have E bieneusi infection.
Myositis due to Pleistophora infection has been documented.
Race
Microsporidiosis has no known racial predilection.
Sex
Microsporidiosis has no known gender predilection.
Age
Microsporidiosis has no known age predilection.
Prognosis
Most patients who develop intestinal microsporidiosis are severely immunosuppressed; therefore, the prognosis usually is poor in these patients.
Diarrhea generally resolves spontaneously in immunocompetent patients who develop microsporidiosis.
Patient Education
Counsel patients regarding meticulous handwashing to help decrease the risk for opportunistic infections.
-
Electron micrograph (X30,000) of Nosema connori in diaphragm showing a coiled polar filament (arrow). Courtesy of the Armed Forces Institute of Pathology (AFIP 71-11521-4).





