Practice Essentials
Natural killer (NK)-cell lymphoma is a type of non-Hodgkin lymphoma (NHL). [1, 2] Most NHLs (90%) are of B-cell origin. In the past, the rarity of non–B-cell malignancies and their similar morphologic findings, coupled with the unavailability of cell markers, made it impossible to establish definitive classifications of subtypes of non–B-cell NHL.
This lack of knowledge also prevented clinicians from gathering meaningful information about the natural history of the disease and its prognosis. The unavailability of this information is demonstrated in previous classification systems, including the Lukes-Collins, Kiel, and Working Formulation systems, which did not identify subclasses of NK/T-cell malignancies.
Advances in tumor cell biology have led to the ability to subclassify NHL via the World Health Organization (WHO) classification of lymphomas (see below). This terminology will likely become more precise as our ability to genetically characterize these tumors improves. [3] Previous terms for NK-cell malignancies and other forms of non–B-cell NHL included lethal midline granuloma, angiocentric lymphoma, malignant granuloma, malignant midline reticulosis, and polymorphic reticulosis. These terms were based on clinical and pathologic characteristics of the diseases encountered.
Controversy still exists over the normal counterpart of NK-cell lymphoma. Whether NK-cell lymphoma represents the presence of a true NK cell or merely the presence of a T cell with abnormal cell markers is under debate. In the absence of unequivocal proof of the exact lineage of NK-cell lymphoma, many investigators prefer to use the term NK/T-cell lymphoma (NKTCL) when classifying this condition. Further understanding of its development and identification of more specific cell markers of NK and T cells will likely resolve this controversy in the future.
The peripheral T- and NK-cell lymphomas classified by the WHO have many subclasses (see below). The subgroupings, which primarily involve the head and neck region, include the nasal and nasal-type extranodal NKTCLs. The term extranodal is used because these forms of malignancies are found outside of the traditional lymph node groupings.
The nasal and nasal-type NKTCLs have distinct presentations and prognoses, and they are believed to have different pathogeneses. Otolaryngologists should understand the importance of differentiating NKTCL from other similar pathologic entities found in the head and neck region; the prognoses differ substantially.
World Health Organization classification of lymphomas
In the WHO lymphoma classification, B-cell neoplasms include the following:
-
Precursor B-lymphoblastic leukemia/lymphoma
-
Chronic lymphocytic leukemia/small lymphocytic lymphoma
-
Lymphoplasmacytic lymphoma
-
Plasma cell myeloma
-
Extraosseous plasmacytoma
-
Extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue (MALT)
-
Follicular lymphoma
-
Mantle cell lymphoma
-
Diffuse large B-cell lymphoma
-
Intravascular large B-cell lymphoma
B-cell proliferations of uncertain malignant potential include the following:
-
Lymphomatoid granulomatosis
-
Posttransplant lymphoproliferative disorder, polymorphic
T-cell and NK-cell neoplasms include the following:
-
Precursor T-lymphoblastic leukemia/lymphoma
-
Blastic NK-cell lymphoma
-
Adult T-cell leukemia/lymphoma
-
Extranodal NKTCL, nasal type
-
Subcutaneous panniculitislike T-cell lymphoma
-
Mycosis fungoides
-
Sézary syndrome
-
Primary cutaneous anaplastic large cell lymphoma
-
Peripheral T-cell lymphoma
-
Angioimmunoblastic T-cell lymphoma
-
Anaplastic large-cell lymphoma
T-cell proliferations of uncertain malignant potential include the following:
-
Lymphomatoid papulosis
-
Hodgkin lymphoma
-
Histiocytic and dendritic-cell neoplasms
-
Mastocytosis
Signs and symptoms of NK-cell lymphomas
Head and neck findings in NKTCL include the following:
-
Cranial neuropathies
-
Visual impairment
-
Orbital mass
-
Proptosis
-
Facial swelling and erythema (midline facial features)
-
Serous otitis media
-
Ulcerations of the palate, tonsil, nasopharynx, and larynx
-
Nasal mass
-
Neck mass
Workup in NK-cell lymphomas
The following laboratory studies should be performed:
-
Complete blood count (CBC) - This may reveal anemia or lymphocytopenia
-
Liver function tests, including assessment of lactic dehydrogenase (LDH) levels - Elevated LDH levels have been associated with poorer prognoses; these levels should be checked in every patient
-
Renal function tests
-
Uric acid and calcium levels
-
Epstein-Barr virus (EBV) titers
Imaging studies are obtained to determine the full extent of disease for staging purposes. Computed tomography (CT) scanning of the neck, chest, abdomen, and pelvis is indicated. Neck CT scanning is important for detecting skull base erosion and intracranial extension. [4, 5] Magnetic resonance imaging (MRI) of the head is performed in cases of suspected skull base invasion and intracranial extension. [4, 5]
Flexible nasopharyngoscopy with direct laryngoscopy should be performed to characterize the extent of the lesion.
Biopsy of the primary site should be done to characterize the morphology and to allow genetic studies (eg, for Epstein-Barr virus [EBV]) and immunohistochemical studies.
Management of NK-cell lymphomas
Early stage, localized NKTCL of the head and neck may be treated with local radiotherapy; however, monotherapy may result in high rates of local and distant recurrence (up to 49%). [6, 7] Currently recommended treatment includes CHOP (cyclophosphamide, doxorubicin, vincristine, prednisone) chemotherapy in conjunction with radiotherapy.
Surgical management of patients with NKTCL is limited to biopsy, stabilization of the airway if necessary, or debulking of disease.
Pathophysiology
Extranodal NKTCL manifests in the nasal cavity. Patients with this type tend to have earlier disease (stage I). However, later-stage presentations are observed, and the stage at presentation has an impact on the survival rate. Nasal NKTCLs are almost always (>95% of cases) associated with Epstein-Barr virus (EBV), irrespective of the ethnicity of the patient. The exact mechanism of malignant transformation via EBV has not been clearly elucidated. [8, 9, 10]
Extranodal nasal-type NKTCL demonstrates a predilection for the nasopharynx (see the image below), palate, skin, soft tissues, orbit, gastrointestinal (GI) tract, and testes. Secondary lymph nodes may be involved in some cases; a disseminated leukemic picture is even possible. Lymphomas that manifest outside of the nose have a strong association with EBV in Asian patients, but this strong association is not present in whites.
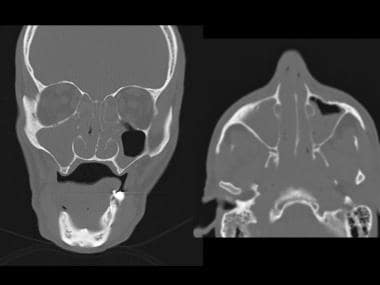 Coronal (left) and axial (right) CT scans of the sinus reveal severe pansinusitis with abnormal nasopharyngeal thickening, right facial edema and right temporal bone opacification.
Coronal (left) and axial (right) CT scans of the sinus reveal severe pansinusitis with abnormal nasopharyngeal thickening, right facial edema and right temporal bone opacification.
The pattern of involvement of the extranasal sites has been hypothesized to be related to the marker CD56. CD56 represents the neural cell adhesion molecule (NCAM) that has been shown to have homophilic binding properties. With the skin, GI tract, and testes expressing the CD56 marker in large amounts, the neoplastic cells travel to these areas and set up foci of disease. The skin is the most common site of dissemination in NKTCL.
Etiology
Risk factors for NKTCL are as follows:
-
Inherited immunodeficiencies – Klinefelter syndrome, Chédiak-Higashi syndrome, ataxia telangiectasia syndrome, Wiskott-Aldrich syndrome, and common variable immunodeficiency disease
-
Acquired immunodeficiency diseases – Iatrogenic immunosuppression, HIV-1 infection, and acquired hypogammaglobulinemia
-
Autoimmune disease – Sjögren syndrome, celiac sprue, rheumatoid arthritis, and systemic lupus erythematosus
-
Chemical or drug exposures – Phenytoin, dioxin, phenoxyl herbicides, irradiation, and prior chemotherapy or radiotherapy
-
Association with infectious agents – EBV, human T-cell leukemia/lymphoma virus-I, and ataxia telangiectasia syndrome
Epidemiology
NKTCL is very rare in whites; its prevalence is significantly higher in people of Asian descent. In Western populations, the prevalence of nasal lymphomas is estimated at 0.17-1.5% of all NHLs, 45% of which are thought to be NK-/T-cell in origin. Worldwide, NKTCL has a low prevalence, but it is much more prevalent in Asia, Mexico, and Central and South America. [11, 12, 13] Reported rates of nasal lymphoma in Hong Kong and South America range from 2.6% to 8% of all NHLs, of which 45% are thought to represent NKTCL.
Patients with NKTCL commonly present in their sixth decade of life, which is almost a decade younger than the age at which people with B-cell neoplasms present. However, the disease has been seen in both geriatric and pediatric populations. [14, 4] Men are more commonly affected with the disease than women, with a male-to-female ratio of almost 3:1. [14, 4, 12]
Using the Surveillance, Epidemiology, and End Results (SEER) Program database, Kommalapati et al determined that between 2001 and 2014, the US incidence of nasal NKTCL doubled, from 0.4 to 0.8 per 1,000,000 individuals. The incidence in Hispanic patients was significantly higher than that in non-Hispanic patients. [15]
A retrospective Brazilian study, by de Arruda JAA, of oral and oropharyngeal lymphomas found that mature T- and NK-cell neoplasms were the second most common group of these lymphomas (the most common being mature B-cell neoplasms [87.2%]). Moreover, extranodal NKTCLs made up the most frequent subtype of these neoplasms. [16]
Prognosis
Compared with other subtypes of lymphoma found in the head and neck region, NKTCL carries a much higher mortality and responds less well to traditional chemotherapy and radiotherapy regimens. [17] Overall, median survival time is reported as 12.5 months (although the aforementioned study by Kommalapati et al reported the median overall survival time for nasal NKTCL to be 20 months, with this period varying significantly with the disease’s primary site and NKTCL’s stage at diagnosis [15] ). Survival time for patients who present with a disseminated leukemic picture is reported to be less than 6 months. A complete response to primary treatment is reported in 56% of patients. Overall, the 2-year survival rate is 45%, and the 2-year disease-free survival (DFS) rate is reported at 31%.
A retrospective study by Su et al of 101 patients with extranodal NKTCL indicated that age 60 years or greater and the presence of Ann Arbor stage III/IV disease are independent risk factors for poor progression-free and overall survival. Median periods of progression-free and overall survival in the advanced-stage patients were 2.3 and 4.8 months, respectively. [18]
The poor survival rates and low rates of response to treatment in NKTCL are theorized to be secondary to the CD56 cell marker and the presence of a multidrug resistance (P-glycoprotein–positive) phenotype. CD56 is thought to facilitate tumor cell dissemination by virtue of its binding properties.
A study by Zhang et al indicated that higher levels of myeloid-derived suppressor cells (MDSCs), specifically, HLA-DR-CD33+CD11b+ MDSCs and CD14+ monocytic MDSCs, independently predict poor disease-free and overall survival in patients with extranodal NKTL. The MDSCs were found to suppress T-cell proliferation in these patients. [19]
On the other hand, a literature review by Chen et al indicated that the prognosis in extranodal NKTCL tends to be better when CD30, a tumor necrosis factor receptor superfamily member, is expressed. The investigators reported that CD30 expression is associated with a 41% relative decrease in hazard of death. [20]
NKTCLs have a higher local relapse rate (21.4%) than do either T-cell lymphomas presenting in the nasopharynx (5%) or B-cell lymphomas presenting in the nasopharynx (0%). Fewer recurrences in the cervical nodes are reported for NKTCLs (2.4%) than are reported for T-cell (10%) and B-cell (14.3%) malignancies.
Hemophagocytic syndrome, associated with fever, marked pancytopenia, hemophagocytic histiocytes in the bone marrow, and rapid liver function deterioration, is a devastating complication of NHL. This syndrome appears to be much more common in NKTCLs.
In a study involving 69 patients with early stage extranodal nasal-type NKTCL (58 with stage I and 11 with stage II) who received primary radiotherapy, high pretreatment Epstein-Barr virus (EBV)–DNA concentrations were associated with B symptoms, elevated lactic dehydrogenase (LDH) levels and a high International Prognostic Index score. [21] The investigators suggested that circulating EBV-DNA levels could serve both as a valuable biomarker of tumor load for accurate classification of early stage disease and as a prognostic factor.
Similarly, a literature review by Liu et al indicated that in patients with NKTCL, circulating EBV-DNA concentrations predict patient survival and treatment response. The investigators reported that overall and progression-free survival are poorer in individuals with both a high pretreatment EBV-DNA level and a detectable posttreatment concentration. Moreover, an apparent association was found between a high pretreatment level and a decreased treatment response. [22]
-
Coronal (left) and axial (right) CT scans of the sinus reveal severe pansinusitis with abnormal nasopharyngeal thickening, right facial edema and right temporal bone opacification.
-
MRI revealed a low, non enhancing T1 signal in the right maxillary, ethmoid and sphenoid sinuses. (left) A high and inhomogeneous T2 signal suggested tumor involvement and destruction of the middle and inferior turbinates. (right)
-
High-power photomicrograph of a nasopharyngeal mass that was diagnosed as natural killer (NK)–/T-cell lymphoma, nasal type. In this section stained with hematoxylin and eosin, a diffuse infiltrate of variably sized cells with irregularly shaped nuclei that contain coarsely granular chromatin is visible. In other areas of this tumor, necrosis and angiocentrism could be appreciated.
-
In this photomicrograph, immunohistochemical staining shows neoplastic cells to be positive for the pan T-cell antigen CD3 (positive cells have a brown tinge).
-
In this photomicrograph, immunohistochemical staining shows neoplastic cells to be positive for the natural killer (NK)–cell antigen CD56 (positive cells have a brown tinge).
-
In this photomicrograph, immunohistochemical staining shows neoplastic cells to be focally positive for granzyme B (positive cells have a brown tinge).
-
In this photomicrograph, in situ hybridization for Epstein-Barr virus RNA (EBER) shows positivity in neoplastic cells (positive cells have black nuclei).









