Practice Essentials
Sternal fractures are predominantly associated with deceleration injuries and blunt anterior chest trauma (incidence of 3-6.8% in motor vehicle collisions). Consider the diagnosis on the basis of the mechanism of injury. Direct trauma is the most common cause of injury (eg, motor vehicle accidents, sports, and falls). [1, 2, 3] Sternal fractures are associated with thoracic or lumbar vertebral fractures. Severe pain associated with sternal fractures can lead to impaired ventilation, low partial pressure of arterial oxygen, or the need for noninvasive or invasive ventilation with an endotracheal tube, thereby involving significant morbidity. [4]
Fractures usually occur at the body or the manubrium. Lateral chest radiograph is considered the gold standard for making the diagnosis, because fracture and displacement or dislocation occurs in the sagittal plane. An anteroposterior chest radiograph can be helpful in detecting other injuries, such as rib fracture, pulmonary contusion, hemothorax, and pneumothorax. Ultrasonography demonstrates sternal fractures with as much sensitivity as plain radiography and can accurately identify related hematomas and pleural effusions, but ultrasound is not accurate in identifying the degree of displacement of sternal fractures. [5, 6, 7, 8]
(See the images below.)

Most sternal fractures are caused by blunt anterior chest trauma. Insufficiency fractures caused by abnormally decreased bone density or weakened bone can occur spontaneously in patients with osteoporosis or osteopenia (particularly in older persons, especially women), those on long-term steroid therapy, or those with severe thoracic kyphosis. Cardiopulmonary resuscitation commonly causes rib and sternal fractures.
With increased use of seat belts and shoulder restraints, the incidence of sternal fracture has increased, but overall severity of injuries has decreased. Presumably, incidence has increased because all of the deceleration forces are concentrated into a nonelastic 2-inch strap that transmits this force directly to the sternum. [9] Effects of airbags on incidence of sternal fractures are not fully known, though literature suggests a decreased incidence when these are deployed.
Almost all patients complain of localized sternal pain. Pain may be more diffuse in patients with insufficiency fractures and may lead to a more extensive differential diagnosis for chest pain in older persons.
Sternal fracture is considered a marker for significant transmission of energy. Management of isolated sternal fractures is usually nonoperative, with surgery reserved for displaced fractures or cases of respiratory insufficiency. However, management may become challenging when these fractures are associated with other significant trauma. [10]
Consider at least an observation admission for elderly persons with chest wall fractures because these patients are at increased risk for respiratory compromise and atelectasis.
Pathophysiology
Most sternal fractures are caused by blunt anterior chest trauma, although stress fractures have been noted in golfers, weight lifters, and other participants in noncontact sports. Insufficiency fractures caused by abnormally decreased bone density or weakened bone can occur spontaneously in patients with osteoporosis or osteopenia (particularly in older persons, especially women), those on long-term steroid therapy, or those with severe thoracic kyphosis. Cardiopulmonary resuscitation commonly causes rib and sternal fractures, something that must be considered during the recovery process from the illness that led to the cardiac arrest.
Fractures usually occur at the body or the manubrium. In one study of 79 patients with sternal fracture, 13 (16.5%) had a fracture of the manubrium, 10 caused by seat-belt injury. In 3 cases, stabilization was performed, and follow-up showed sufficient consolidation without complications. [11]
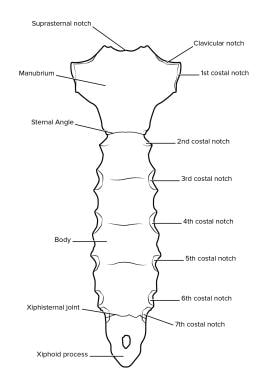
(Surface anatomy of the sternum is shown in the illustration below.)
Epidemiology
Motor vehicle collisions account for 60-90% of sternal fractures. [12] Most of these are in older vehicles in which a seat belt is used but no airbag deploys. [13] Those who are unrestrained generally sustain injury from ejection from the vehicle or impact with the steering wheel or dashboard. Direct impact sports, falls, vehicle-to-pedestrian accidents, and assaults account for most of the rest. Spontaneous fractures and stress fractures are rare. Occurrence of sternal fracture has tripled with the use of vehicular shoulder restraints, likely secondary to deceleration forces concentrated directly to the sternum. [14]
Sternal fractures are slightly more common in females than in males, possibly because of shoulder restraint positioning; however, the difference is small. Sternal fractures are more common in patients older than 50 years, possibly because of a weaker or inelastic bony thorax. Because of the elasticity of their chest walls, children less commonly have sternal fractures; however, when present, the underlying injuries may be more severe. [15, 16, 17, 18]
Because of the lack of substantial change in size or shape of the sternum between ages 30 and 100 years, the increased incidence of sternal fracture in the elderly may be the result of cortical thickness or bone mineral density changes in the sternum, as opposed to changes in morphology. [13]
Prognosis
The prognosis is excellent for isolated sternal fractures. Most patients recover completely over a period of several weeks. In the absence of other injuries or severe pain, patients with isolated sternal fractures do not need admission to hospital. [19] In rare cases of nonunion and chronic sternal pain, surgical fixation can be considered.
The mortality rate from isolated sternal fracture is extremely low. Mortality associated with sternal fracture is 0.7%. Death and morbidity are related almost entirely to associated injuries, such as aortic disruption, cardiac contusion, and pulmonary contusion, or to unrelated injuries to the abdomen or head sustained in the accident, with reported mortality of 25-45%. [19]
-
Posterior surface of the sternum.
-
Lateral radiograph shows a complete displaced fracture of the sternum (arrow).









