Practice Essentials
Liposarcoma is a malignancy of fat cells (see Pediatric Liposarcoma and Liposarcoma Imaging). In adults, it is the most common soft tissue sarcoma. Liposarcoma normally appears as a slowly enlarging, painless, nonulcerated submucosal mass in a middle-aged person, but some lesions grow rapidly and become ulcerated early.
Signs and symptoms
The 3 most common locations of involvement are the thighs, the retroperitoneum, and the inguinal region.
Liposarcoma usually appears as a well-circumscribed palpable mass as large as 10 cm in diameter. The mass tends to grow slowly over time. The lesion is commonly not tender on palpation. Diffuse abdominal enlargement may be observed in patients with retroperitoneal disease. Liposarcoma that resembles a skin tag has been reported but is an exceptionally rare event. [1]
Fascial compartmentalization may cause liposarcomas to have awkward discoid and fusiform shapes rather than smooth, round forms. Thus, liposarcoma can appear with an array of clinical morphologies and manifestations. Other aspects to note on physical examination are neurologic involvement and lymphadenopathy.
Pleomorphic liposarcoma is both uncommon and rarely occurs in the skin and subcutis. [2] They are most often located on an extremity, trunk, and head and neck and more often involve the subcutaneous, less so the subcutis or dermis. It may be evident as a painless pedunculated pink papulonodule. [3]
Diagnostics
See Workup for a full discussion.
Cytogenetics may be of value when diagnosing lipomatous tumors because different tumor types have different more or less specific chromosomal abnormalities. [4] The lipoblastoma, for example, often exhibits rearrangements of bands 8q11-13, and the gene PLAG1 has been implicated as the target of these chromosomal changes. Atypical lipomatous tumors may display gene amplifications within the 12q13-15 region, including HMG2A (high-mobility group protein 2a), YEATS4 (YEATS domain containing 4), and CPM (carboxypeptidase M). [5]
Imaging
CT scanning (see image below) is superior to MRI in detailing cortical bone erosion and tumor mineralization, whereas MRI is useful in providing views of the long axis of the limb and in depicting the fatty nature of the tumor.
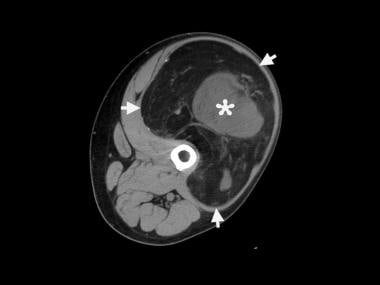 Computed tomography (CT) scan of a left thigh shows a huge mass (arrows) with predominant fat attenuation. The central soft-tissue component (asterisk) and thick, internal septations are consistent with liposarcoma.
Computed tomography (CT) scan of a left thigh shows a huge mass (arrows) with predominant fat attenuation. The central soft-tissue component (asterisk) and thick, internal septations are consistent with liposarcoma.
Most liposarcomas have well-defined and mostly lobulated margins. The well-differentiated liposarcomas are composed of mainly fat with septa or nodules. These tumors are hyperintense on T2-weighted images, and they demonstrate faint enhancement or no enhancement after the intravenous administration of contrast material.
Myxoid liposarcomas are homogeneous or mildly heterogeneous, and a pseudocapsule can be present. Pleomorphic types have a markedly heterogeneous internal structure. Both myxoid and pleomorphic lesions have moderate or marked heterogeneous enhancement after the administration of contrast material. Well-differentiated liposarcomas may be distinguished from the other types by their largely lipomatous appearance. The malignancy grade increases with the degree of tumor heterogeneity and contrast enhancement.
Angiography may demonstrate tumor malignancy on the basis of prominent vascularity; thus, angiography may be of value in planning surgical resection.
Chest radiography may be used as an initial screening for pulmonary metastases; however, the definitive test for detection of pulmonary metastases is chest CT scanning.
An early-phase bone scan may show a marked increase of radioisotopic uptake.
Risk assessment in liposarcoma patients can be based on [(18)F]fluorodeoxyglucose (FDG) PET imaging. [6] Although tumor grade and subtype are considered standard parameters for risk assessment in patients with liposarcoma, pretherapy tumor standardized uptake values obtained by FDG PET imaging was found to be a more useful parameter for risk assessment in liposarcoma compared with tumor grade or subtype. A maximum standardized uptake value of more than 3.6 was associated with significantly reduced disease-free survival and identified patients at high risk for developing early local recurrences or metastatic disease.
Also see Liposarcoma Imaging.
Management
The rationale for wide surgical excision of atypical lipomatous tumors is the prevention of recurrence and dedifferentiation.
Wide and deep surgical excision, along with local radiation and/or chemotherapy, may be necessary for high-grade lesions.
Given the favorable outcome with wide surgical excision alone, regardless of the histologic type of the tumor, some authors believe that adjuvant radiation therapy is unjustified.
Also see Treatment.
Background
Virchow first described liposarcoma in the 1860s.
The development of a liposarcoma from a preexisting benign lipoma is rare. Most cases arise de novo. Liposarcomas most frequently arise from the deep-seated stroma rather than the submucosal or subcutaneous fat. Dermal lesions are rare and may resemble pleomorphic fibroma. [7]
The most recent World Health Organization classification of soft tissue tumors recognizes 5 categories of liposarcomas: (1) well differentiated, which includes the adipocytic, sclerosing, and inflammatory subtypes; (2) dedifferentiated; (3) myxoid; (4) round cell; and (5) pleomorphic.
A spindle-cell variant of well-differentiated liposarcoma is also described. The concept that round-cell liposarcoma represents the high-grade counterpart of myxoid liposarcoma is generally accepted. Spindle-cell liposarcoma is a rare variant of an atypical lipomatous tumor (ie, well-differentiated liposarcoma), and it must be distinguished from a dedifferentiated liposarcoma with metastatic potential and a benign spindle-cell lipoma. [5] The advent of cytogenetic and molecular investigations has contributed to better categorization of this subset of mesenchymal neoplasms. Not only have they provided new insights into the biology of these tumors, but they have also validated the current classification schemes based on conventional morphologic observations. [8, 9, 10, 11]
Liposarcoma occurs in three main biologic forms: (1) well-differentiated liposarcoma; (2) myxoid and/or round cell; and (3) pleomorphic. The latter is a rare high-grade type with a high recurrence rate and poor prognosis. [12] Exceptionally, there may be a combination of morphologic types; these are classified as combined or mixed-type liposarcomas.
The anatomical distribution of liposarcoma appears to be partly related to the histologic type. Well-differentiated liposarcoma tends to occur in deep soft tissues of both the limbs and the retroperitoneum. Myxoid and/or round-cell liposarcomas and pleomorphic liposarcomas have a striking predilection for the limbs, and dedifferentiated liposarcoma occurs predominantly in the retroperitoneum. Although any liposarcoma subtype occasionally arises in the subcutis, involvement of the dermis appears to be exceedingly rare.
Pathophysiology
Liposarcoma is a lipogenic tumor of large deep-seated connective tissue spaces. Fusion proteins created by chromosomal abnormalities are key components of mesenchymal cancer development. An abnormality of band 12q13 has been associated with the development of liposarcomas. The most common chromosomal translocation is the FUS-CHOP fusion gene, which encodes a transcription factor necessary for adipocyte differentiation. These and other distinct genetic aberrations may aid in the diagnosis of particular liposarcoma subtypes, and they can potentially be targets that can be exploited therapeutically. [13]
Etiology
No well-established causative factor has been identified, although trauma has been implicated.
Epidemiology
Frequency
United States
Soft tissue sarcomas occur in approximately 5000 patients in the United States per year. Overall, liposarcomas account for less than 20% of all soft tissue sarcomas, and the average patient age at presentation is 50 years. However, in children, liposarcomas account for less than 5% of all soft tissue sarcomas; fewer than 60 cases in children have been reported.
International
With an annual incidence of 2.5 cases per million population, liposarcoma is the most common soft tissue sarcoma, accounting for approximately 17% of all soft tissue sarcomas and 3% of all liposarcomas in the head and neck region (usually the neck and the cheek). Oral involvement is rare; as of the year 2000, fewer than 50 oral cases had been reported. The trunk and the lower extremities are the most likely sites of tumor development.
Race and sex
No association with race or geography is known.
Liposarcomas are slightly more common in males than in females.
Age
The mean patient age at onset is 50 years. Although liposarcomas account for about 17% of all soft tissue sarcomas, they are involved in only 4% of childhood soft tissue sarcomas. Cases of liposarcoma are reported in young adults and teenagers, but cases in children are rare. [14]
Prognosis
The prognosis is affected by the type of liposarcoma present. In general, survival for extremity tumors is favorable. [15] The histologic grade of localized liposarcomas of the extremities may be the most important prognostic factor. [16]
The well-differentiated type and most myxoid types have favorable prognoses, with 100% and 88% 5-year survival rates, respectively. [17] However, these tumors are poorly circumscribed and locally recur after incomplete excision. Although they rarely metastasize, repeated local recurrences may cause the tumor to evolve into a higher grade of sarcoma or to dedifferentiate, in which case metastasis is possible. Between 1973 and 2015, 1756 patients with extremity myxoid liposarcomas were evaluated. The 5- and 10-year overall survival rates of the entire cohort were 86.4% and 75.9%, respectively. [18]
The form that a dermatologist is most likely to examine at biopsy is 1 of the 3 subtypes of a well-differentiated liposarcoma, that is, the lipomalike liposarcoma or atypical lipoma; the other 2, inflammatory and sclerosing, are less likely. [5] The clinical outcome of this subtype is best predicted by the anatomical location. In the subcutis, lipomalike liposarcomas are often cured with local excision. Lipomalike liposarcomas rarely recur, and they do not metastasize. Use of the term atypical lipomatous tumor, a less serious designation for atypical lipoma, has been suggested.
Round-cell and poorly differentiated types have a poor prognosis. Each has a 5-year survival rate of about 50% because they recur locally and tend to metastasize quickly and widely, especially in poorly differentiated liposarcomas. The lungs and the liver are the most common sites of metastasis.
Despite high-grade morphology, cutaneous liposarcomas have a favorable clinical prognosis.
For soft tissue sarcoma involving the popliteal fossa, despite a high rate of microscopically positive margins, the local recurrence rate reported is only 7%. [19]
Cutaneous and subcutaneous pleomorphic liposarcomas have a more favorable outcome compared with their deep-seated counterparts, a fact attributable to their small size and superficial location. [2]
-
Computed tomography (CT) scan of a left thigh shows a huge mass (arrows) with predominant fat attenuation. The central soft-tissue component (asterisk) and thick, internal septations are consistent with liposarcoma.






