Practice Essentials
Refsum disease (RD) is a neurocutaneous syndrome that is characterized biochemically by the accumulation of phytanic acid in plasma and tissues. Patients with RD are unable to degrade phytanic acid because of a deficient activity of phytanoyl-CoA hydroxylase (PhyH), a peroxisomal enzyme catalyzing the first step of phytanic acid alpha-oxidation. RD can be classified as a peroxisome biogenesis disorder. This category is inherited as an autosomal recessive trait and is characterized by altered peroxisome assembly, resulting in multiple peroxisome enzyme deficiencies, complex developmental sequelae, and progressive disabilities. [1, 2] Infantile RD is a peroxisome biogenesis disorder. [3]
Signs and symptoms
Symptoms develop progressively and slowly with neurologic (eg, mild peripheral intermittent neuropathy, tinnitus, anosmia) and ophthalmic (eg, failing vision, night blindness as a result of progressive retinitis pigmentosa) manifestations.
Ichthyosis may accompany, but most often follows, the occurrence of the above symptoms.
Pertinent physical findings include neurologic, ophthalmic, cardiac, and skin defects.
Neurologic/ophthalmologic signs are as follows (see image below):
-
Partial intermittent sensorimotor polyneuropathy
-
Cataract
-
Nystagmus
-
Retinitis pigmentosa
-
Anosmia
-
Concentric constriction of the visual fields
-
Sensorineural deafness
-
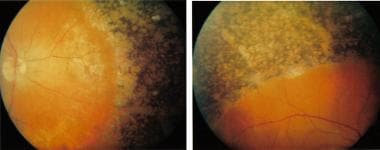 Extensive perivascular "bone spicule" pigmentation seen in both fundi. Courtesy of Hari Jayaram, via Wikimedia Commons.
Extensive perivascular "bone spicule" pigmentation seen in both fundi. Courtesy of Hari Jayaram, via Wikimedia Commons.

Signs resulting from cerebellar ataxia are as follows:
-
Progressive weakness
-
Foot drop
-
Loss of balance
Cardiomyopathy with a serious conduction defect is a life-threatening sign. [4, 5]
Hepatic/renal symptoms are clinically silent despite fatty degeneration.
An ichthyosiform desquamation occurs, resembling a mild acquired ichthyosis vulgaris with a fine, white scaling that is noticeable over the lower trunk but also affects the limbs. Ichthyotic symptoms may range from mild hyperkeratosis of the palms and soles to severe scaling of lamellar ichthyosis type observed on the trunk.
Skeletal defects (noticed in some patients) are not related directly to phytanic acid levels. These defects occur in 35-75% of cases. The knees, elbows, and short tubular bones of the hands and feet are affected (see image below); in particular, the terminal phalanx of the thumb also is affected. Enamel defects have been described in a case report. [6]
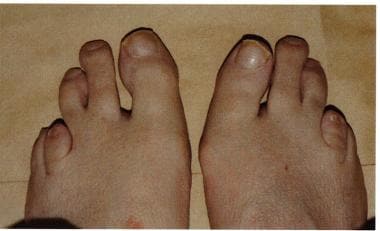 Abnormal second and third toes with a shortened fourth metatarsal. Courtesy of Hari Jayaram, via Wikimedia Commons.
Abnormal second and third toes with a shortened fourth metatarsal. Courtesy of Hari Jayaram, via Wikimedia Commons.
Diagnostics
Also see Workup.
In Refsum disease (RD), the phytanic acid level in the blood is increased. The normal range is equal to or less than 0.2 mg/dL; however, phytanic acid levels are 10-50 mg/dL or even higher in patients with RD.
Cerebrospinal fluid (CSF) shows an albuminocytologic dissociation with a protein level of 100-600 mg/dL.
Low-density lipoprotein (LDL) and high-density lipoprotein (HDL) cholesterol levels are decreased.
Routine laboratory investigations of blood and urine do not reveal any consistent diagnostic abnormalities.
Management
Also see Treatment and Medication.
The following 3 forms of medical care are used for Refsum disease (RD):
-
Diet (see Diet)
-
A phytanic acid-restricted diet and combination docosahexaenoic acid and cholic acid therapy may inhibit disease progression. [7]
-
Plasmapheresis: The main indication for plasmapheresis in patients with RD is a severe or rapidly worsening clinical condition. [8] A minor indication is failure of dietary management to reduce a high plasma phytanic acid level. [9] Cascade filtration may be an alternative for plasmapheresis. It is as efficient as plasmapheresis and eliminates the need for albumin replacement. [10]
-
Local dermatologic drugs to soften the skin (see Medication)
Although there is no cure, phytanate levels in RD patients can be reduced by plasmapheresis and a strict diet. [11]
Pharmacological up-regulation of the omega-oxidation of phytanic acid may form the basis of the new treatment strategy for adult RD in the near future. [12]
Background
Refsum first described this disease in 1946. Peripheral polyneuropathy, cerebellar ataxia, retinitis pigmentosa, and ichthyosis are the major clinical components. The symptoms evolve slowly and insidiously from childhood through adolescence and early adulthood.
Pathophysiology
Refsum disease is a recessive disorder characterized by defective peroxisomal alpha-oxidation of phytanic acid. [13, 14, 15] Consequently, this unusual, exogenous C20-branched-chain (3,7,11,15-tetramethylhexadecanoic acid) fatty acid accumulates in blood and tissues. It is almost exclusively of exogenous origin and is delivered mainly from dietary plant chlorophyll and, to a lesser extent, from animal sources. Blood levels of phytanic acid are increased in patients with Refsum disease. These levels are 10-50 mg/dL, whereas normal values are less than or equal to 0.2 mg/dL, and account for 5-30% of serum lipids. Fatty acid‒mediated neurodegeneration merits further scrutiny. [16]
Phytanic acid replaces other fatty acids, including such essential ones as linoleic and arachidonic acids, in lipid moieties of various tissues. [17] This situation leads to an essential fatty acid deficiency, which is associated with the development of ichthyosis. [18] A Refsum disease gene, phytanoyl-CoA hydroxylase (PHYH), has been localized to band 10p13 between the markers D10S226 and D10S223. [19] Refsum disease is genetically heterogeneous, with up to 55% of cases not being linked to the PAHX gene locus at D10S547 to D10S223. Some patients have been found to carry a defect in perforin 7 (PEX7 defect). [20, 21]
Based on the above, it was proposed that adult Refsum disease could be divided into types 1 and 2, depending on which gene is defective. [22] Thus, Refsum disease, like other peroxisomal diseases, is a heterogeneous syndrome. Recently, a mouse model for Refsum disease (Phyh knockout mouse by targeted disruption of the PHYH gene). In humans, the PHYH gene is about 21 kb and consists of 9 exons and 8 introns. It encodes a protein of 38.6 kd. [23]
An infantile form of Refsum disease also exists and is an autosomal recessive disorder of peroxisomal biogenesis, leading to many biochemical abnormalities, including elevated plasma concentration of phytanic acid, pristanic acid, very long chain fatty acids, and C27 bile acids. The disease presents in the first year of life and manifests with developmental delay, visual and hearing disturbances, and dysmorphic features. Ichthyosis is an unusual symptom. [24, 25]
Etiology
Refsum disease is caused by mutations in the phytanoyl-CoA hydroxylase (PHYH) and the PTS2 receptor (PEX7) genes. This disorder is inherited in an autosomal recessive mode. A single peroxisomal enzyme defect that causes deficiency of alpha-oxidation leads to accumulation of phytanic acid in blood and tissues of patients with Refsum disease. The cytotoxic effect of phytanic acid seems to be due to a combined action of Ca2+ regulation, mitochondrial depolarization, and increased reactive oxygen species generation in brain cells.
Epidemiology
Refsum disease is rare, with just 60 cases published worldwide. No racial predominance is reported. Only male cases were reported initially; however, now, neither sex predominates.
Classic Refsum disease manifests in children aged 2-7 years; however, diagnosis usually is delayed until early adulthood. However, a patient was described with rare late-onset adult disease first evident at age 72 years. [26] Infantile Refsum disease makes its appearance in early infancy.
Prognosis
Prognosis in untreated patients generally is poor. Dysfunction of myelinated nerve fibers and the cardiac conduction system leads to central and peripheral neuropathic symptoms, impaired vision, and cardiac arrhythmias. The latter frequently are the cause of death. Reversible vestibular neuropathy has been described. [27]
In early diagnosed and treated cases, phytanic acid decreases slowly, followed by improvement of the skin scaling and, to a variable degree, reversal of recent neurological signs. Retention of vision and hearing are reported. Attenuation of neurologic, ophthalmologic, and cardiac symptoms requires constant adherence to a suitable diet and plasmapheresis.
-
Extensive perivascular "bone spicule" pigmentation seen in both fundi. Courtesy of Hari Jayaram, via Wikimedia Commons.
-
Abnormal second and third toes with a shortened fourth metatarsal. Courtesy of Hari Jayaram, via Wikimedia Commons.




