Background
Tolosa-Hunt syndrome (THS) is a painful ophthalmoplegia caused by nonspecific inflammation of the cavernous sinus or superior orbital fissure. In 2004, the International Headache Society provided a definition of the diagnostic criteria, which included granuloma. [1] See the image below.
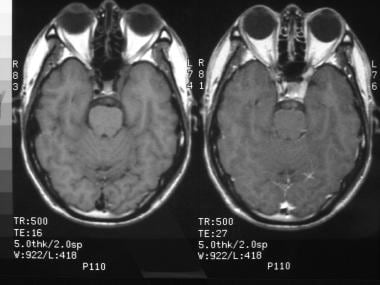 MRI of a 40-year-old man with severe periorbital pain ocular sinister (OS; ie, left eye), complete oculomotor nerve palsy OS, and partial abducens nerve palsy OS. Axial imaging without (left) and with (right) enhancement demonstrates nonspecific fullness involving the left cavernous sinus, consistent with Tolosa-Hunt syndrome within the context of the history. Treatment with steroids produced complete resolution of symptoms. Image courtesy of Eric Eggenberger, DO.
MRI of a 40-year-old man with severe periorbital pain ocular sinister (OS; ie, left eye), complete oculomotor nerve palsy OS, and partial abducens nerve palsy OS. Axial imaging without (left) and with (right) enhancement demonstrates nonspecific fullness involving the left cavernous sinus, consistent with Tolosa-Hunt syndrome within the context of the history. Treatment with steroids produced complete resolution of symptoms. Image courtesy of Eric Eggenberger, DO.
Pathophysiology
Nonspecific inflammation (noncaseating granulomatous or nongranulomatous) within the cavernous sinus or superior orbital fissure is the cause of the constant pain, which characterizes the onset of this disorder. Ophthalmoparesis or disordered eye movements occur when cranial nerves III, IV, and VI are damaged by granulomatous inflammation. Pupillary dysfunction may be present and is related to injury to the sympathetic fibers in the cavernous portion of ICA or parasympathetic fibers that surround the oculomotor nerve. Trigeminal nerve involvement (primarily V1) may cause paresthesias of the forehead. Pathological involvement beyond the cavernous sinus, superior orbital fissure, or apex of the orbit occurs rarely, and the disorder is part of a continuum with idiopathic orbital pseudotumor, with which it shares histopathologic features. Spontaneous remissions can occur; relapses may occur in up to 40% of the patients.
Epidemiology
Frequency
Tolosa-Hunt syndrome (THS) is uncommon in both the United States and internationally. The disorder is rare during the first 2 decades of life; in people older than 20 years, it appears to have an even distribution. When THS occurs in children, the course of the disorder appears to be similar to that experienced by adults. [2] THS affects males and females equally. And, as stated, although rare in children it is important to keep this condition in the differential diagnosis. [3]
Mortality/Morbidity
Tolosa-Hunt syndrome is not a fatal disorder; patients experience unilateral onset of acute orbital pain and ophthalmoparesis, and the disorder may threaten sight if untreated inflammation extends beyond the cavernous sinus to affect the optic nerve.
Prognosis
Typically, the prognosis for Tolosa-Hunt syndrome is considered good. Patients usually respond to corticosteroids, and spontaneous remission can occur, although permanent ocular motor deficits may remain.
Relapse can occur in as many as 40% of patients successfully treated for Tolosa-Hunt syndrome. This typically occurs on the same side as the original lesion but can be observed on the opposite side. Spontaneous remission can occur; patients who have experienced spontaneous remission appear to have as much risk of reoccurrence as those treated with medication. Gimenez-Roldan et al have reported that relapses may occur as long as 13 years after initial diagnosis and treatment. [13]
Patient Education
Patients should understand that this is an idiopathic condition that is usually self-limited. Relapses may occur (30-40% of patients may experience relapse), and patients should know that the course of any relapse often follows the original event but may require additional testing. Patients should have an idea of the differential diagnosis of Tolosa-Hunt syndrome and report any new symptoms or side effects from treatment to the physician.
The risks associated with the use of high-dose steroids should be emphasized prior to the onset of treatment.
-
MRI of a 40-year-old man with severe periorbital pain ocular sinister (OS; ie, left eye), complete oculomotor nerve palsy OS, and partial abducens nerve palsy OS. Axial imaging without (left) and with (right) enhancement demonstrates nonspecific fullness involving the left cavernous sinus, consistent with Tolosa-Hunt syndrome within the context of the history. Treatment with steroids produced complete resolution of symptoms. Image courtesy of Eric Eggenberger, DO.
-
Coronal T1-weighted MRI with (below) and without (above) enhancement demonstrates left cavernous sinus fullness consistent with Tolosa-Hunt syndrome (THS). The imaging features are nonspecific and must be placed into the context of the history, examination, and clinical course to avoid misdiagnosis of infiltrating, infectious, or neoplastic cavernous sinus processes. Image courtesy of Eric Eggenberger, DO.



