Practice Essentials
Nasal fractures seen in participants of athletic activities occur as a result of direct blows in contact sports and as a result of falls. The nasal bones are the most commonly fractured bony structures of the maxillofacial complex. [1, 2, 3, 4, 5, 6, 7] See the images below.
 Lateral radiographic view of a displaced nasal bone fracture in a patient who sustained this injury because of a punch to the face during a hockey game.
Lateral radiographic view of a displaced nasal bone fracture in a patient who sustained this injury because of a punch to the face during a hockey game.
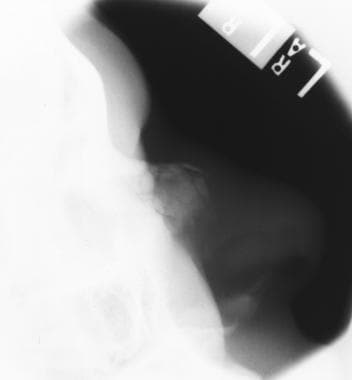 Lateral radiographic view of a nasal bone fracture in an elderly patient who fell forward on her face as a result of syncope. Marked comminution is present.
Lateral radiographic view of a nasal bone fracture in an elderly patient who fell forward on her face as a result of syncope. Marked comminution is present.
The nasal bone's protruding position coupled with its relative lack of support predisposes it to fracture. Prompt appropriate treatment prevents functional and cosmetic changes. Because of the nose's central location and proximity to important structures, the clinician should carefully search for other facial injuries in the presence of facial fractures.
Epidemiology
United States statistics
Nasal fractures occur nearly twice as often in males as in females. Athletic injuries and interpersonal altercations account for the greatest proportion of causes. Less common causes include falls and motor vehicle accidents. [8, 9]
In a retrospective study, Erdmann et al investigated the medical records of 437 patients with 929 facial fractures. [3] These authors noted that the most common etiology of facial trauma was assault (36%), followed by motor vehicle collision (MVC, 32%), falls (18%), sports (11%), occupations (3%), and gunshot wounds (2%). Of the facial fractures sustained, the most common fracture type was nasal bone fracture. [3]
A study by Hanba et al found that risk factors for facial fracture included being white, Asian, female, or ≥ 60 years of age. [10]
A study by Plawecki et al evaluated the incidence of 20,519 patients, 55 years of age or older, who went to the ED for recreational activity-associated facial fractures. The study reported that the annual incidence of facial fractures increased by 45.3% from 2011 through 2015. Nasal fractures were the most common site of fracture (65.4%) and cycling (26.6%) was the most common cause in this cohort of older patients. [11]
In a study of patients who presented to US emergency departments (EDs) with sports- or recreation-related nasal fracture, Xiao et al found that the most common causes of injury were basketball (23.2%), baseball (17.1%), softball (9.8%), soccer (7.4%), and football (7%). Among pediatric patients, the most frequent cause was baseball (25.1%). [12]
International statistics
In a retrospective study of Brazilian children aged 5-17 years, Cavalcanti and Melo found that facial injuries were most frequent in males (78.1%; 3-fold more common than in females) aged 13-17 years (60.9%), and the most common causes of these injuries were falls (37.9%) and traffic accidents (21.1%). [1] Of the facial injuries, nasal fractures were also most common (51.3%), followed by the zygomatic-orbital complex (25.4%).
In another retrospective study, Hwang et al reviewed and analyzed the medical records of 236 patients with facial bone fractures from various sports who were treated at one hospital between 1996 and 2007. [13] The investigators noted the age group with the highest frequency of such injuries was 11-20 years (40.3%), with a significant male predominance across all age groups (13.75:1). There were 128 isolated nasal fractures, with soccer accounting for 39% of these; baseball, 18%; basketball, 12.5%; martial arts, 5%; and skiing or snowboarding, 5%. [13]
In a Finnish study of patients with sports-related nasal fractures, the majority of fractures (56%) were associated with team sports and contact with another player was the most frequent cause of injury (52% of fractures). Among team sports, basketball posed the highest risk of nasal fracture. [14]
A study by Gupta et al found at a British major trauma center that the coronavirus disease 2019 (COVID-19) pandemic may have reduced the number of patients presenting to the ED with nasal fractures. The investigators reported that the number of patients with suspected or confirmed nasal fractures in 2020 was 51.4% less than in 2019. [15]
Functional Anatomy
The lay term nose consists of bone and cartilage. The nasal septum, a commonly injured structure, consists of the vomer, the perpendicular plate of the ethmoid, and the quadrangular cartilage. Paired protrusions from the frontal bones and the ascending processes of the maxilla complete the bony component. The upper lateral and lower lateral cartilages, as well as the cartilaginous septum, compose the nonbony portion.
The blood supply occurs via branches of the ophthalmic artery, the ethmoidal and dorsal arteries, the facial artery, the nasopalatine, the sphenopalatine, and the greater palatine arteries. Sensation results from many small nerve branches; the external surface superiorly receives sensation from the supratrochlear and infratrochlear nerves, and the inferior portion receives sensation from branches of the infraorbital and anterior ethmoidal nerves. Internally, sensation is supplied by branches of the anterior ethmoidal ganglion and the sphenopalatine ganglion.
Sport-Specific Biomechanics
Any force directed to the mid face, either frontally or laterally, can disrupt the nasal anatomy, causing bony or cartilaginous injury. Frontally directed forces must be greater than normal to cause bony injury because the upper and lower lateral cartilages absorb a great deal of impact.
Children are more likely to sustain cartilaginous injury for a variety of reasons. This is mainly because children have a greater proportion of cartilage to bone, and the cartilage provides increased protection from fracture. Children's bones are also more elastic than adults' bones. This explains the increased incidence of greenstick fractures in children (fracture without displacement).
-
Lateral radiographic view of a displaced nasal bone fracture in a patient who sustained this injury because of a punch to the face during a hockey game.
-
Lateral radiographic view of a nasal bone fracture in an elderly patient who fell forward on her face as a result of syncope. Marked comminution is present.
-
Lateral radiographic view of a minimally displaced nasal bone fracture.









