Practice Essentials
Lateral collateral ligament (LCL) injuries result from a varus force across the knee. A contact injury, such as a direct blow to the medial side of the knee, or a noncontact injury, such as a hyperextension stress, may result in a varus force across the knee injuring the LCL. In terms of functionality, the LCL has often been grouped with the popliteofibular ligament and the popliteus tendon as the posterolateral corner (PLC). See the image below.
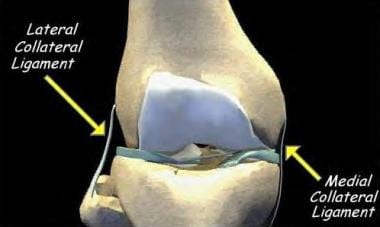 The medial and lateral collateral ligaments of the knee. Courtesy of Randale Sechrest, MD, CEO, Medical Multimedia Group
The medial and lateral collateral ligaments of the knee. Courtesy of Randale Sechrest, MD, CEO, Medical Multimedia Group
Signs and symptoms
Symptoms of LCL injuries include the following:
-
Pain
-
Difficulty on uneven ground
-
Swelling
-
Ecchymosis
Patients may also describe paresthesia as well as a foot drop if injury to the peroneal nerve has occurred.
See Presentation for more detail.
Diagnosis
Radiography of the knee should always be the initial imaging modality. Magnetic resonance imaging (MRI) is an important diagnostic tool for evaluating the LCL as well as the structures of the PLC.
If a multiligamentous knee injury or a knee dislocation is suspected, an arteriogram may be necessary to rule out an arterial injury.
See Workup for more detail.
Management
Grade I and II injuries can usually be treated nonoperatively. Grade III tears of the LCL involve disruption of the PLC and are best treated with surgical intervention to prevent instability.
See Treatment for more detail.
Functional Anatomy
The LCL is a round ligament that originates close to the lateral epicondyle and inserts onto the fibular head.
Sport-Specific Biomechanics
Varus stress
The LCL is the primary restraint to varus stress across the knee.
External tibial rotation
The PLC, which includes the LCL, popliteofibular ligament, and popliteus tendon, is the primary restraint to external rotation stress across the knee.
Etiology
An LCL injury may be caused by a direct blow to the anteromedial aspect of the knee or a noncontact varus or hyperextension injury.
An LCL injury may occur concomitantly with other ligamentous injuries in the setting of a multiple ligamentous knee injury as a result of a significant trauma, such as a motor vehicle accident or a fall from height.
Prognosis
With proper treatment and rehabilitation, the prognosis for LCL injuries is good to excellent.
Complications
Potential complications of LCL injuries are listed below:
-
Chronic pain
-
Weakness
-
Instability
-
Peroneal nerve injury
Patient Education
For patient education resources, see What Are Knee Ligament Injuries? and Workout Injuries: Prevention and Treatment, as well as Knee Injury.
-
The medial and lateral collateral ligaments of the knee. Courtesy of Randale Sechrest, MD, CEO, Medical Multimedia Group






