Blazina ME, Kerlan RK, Jobe FW, Carter VS, Carlson GJ. Jumper's knee. Orthop Clin North Am. 1973 Jul. 4(3):665-78. [QxMD MEDLINE Link].
Almekinders LC, Vellema JH, Weinhold PS. Strain patterns in the patellar tendon and the implications for patellar tendinopathy. Knee Surg Sports Traumatol Arthrosc. 2002 Jan. 10(1):2-5. [QxMD MEDLINE Link].
Basso O, Amis AA, Race A, Johnson DP. Patellar tendon fiber strains: their differential responses to quadriceps tension. Clin Orthop Relat Res. 2002 Jul. 400:246-53. [QxMD MEDLINE Link].
Cook JL, Kiss ZS, Khan KM, Purdam CR, Webster KE. Anthropometry, physical performance, and ultrasound patellar tendon abnormality in elite junior basketball players: a cross-sectional study. Br J Sports Med. 2004 Apr. 38(2):206-9. [QxMD MEDLINE Link]. [Full Text].
Cook JL, Khan KM, Kiss ZS, Purdam CR, Griffiths L. Reproducibility and clinical utility of tendon palpation to detect patellar tendinopathy in young basketball players. Victorian Institute of Sport tendon study group. Br J Sports Med. 2001 Feb. 35(1):65-9. [QxMD MEDLINE Link]. [Full Text].
Cook JL, Khan KM, Kiss ZS, Purdam CR, Griffiths L. Prospective imaging study of asymptomatic patellar tendinopathy in elite junior basketball players. J Ultrasound Med. 2000 Jul. 19(7):473-9. [QxMD MEDLINE Link].
Busch MT. Sports medicine in children and adolescents. Morrissy RT, ed. Lovell and Winter’s Pediatric Orthopaedics. Philadelphia, Pa: Lippincott-Raven; 1990. 1091-1128.
Ferretti A, Ippolito E, Mariani P, Puddu G. Jumper's knee. Am J Sports Med. 1983 Mar-Apr. 11(2):58-62. [QxMD MEDLINE Link].
Lian Ø, Refsnes PE, Engebretsen L, Bahr R. Performance characteristics of volleyball players with patellar tendinopathy. Am J Sports Med. 2003 May-Jun. 31(3):408-13. [QxMD MEDLINE Link].
Ferretti A. Epidemiology of jumper's knee. Sports Med. 1986 Jul-Aug. 3(4):289-95. [QxMD MEDLINE Link].
Kujala UM, Osterman K, Kvist M, Aalto T, Friberg O. Factors predisposing to patellar chondropathy and patellar apicitis in athletes. Int Orthop. 1986. 10(3):195-200. [QxMD MEDLINE Link].
Witvrouw E, Bellemans J, Lysens R, Danneels L, Cambier D. Intrinsic risk factors for the development of patellar tendinitis in an athletic population. A two-year prospective study. Am J Sports Med. 2001 Mar-Apr. 29(2):190-5. [QxMD MEDLINE Link].
Visnes H, Aandahl HA, Bahr R. Jumper's knee paradox--jumping ability is a risk factor for developing jumper's knee: a 5-year prospective study. Br J Sports Med. 2012 Oct 11. [QxMD MEDLINE Link].
Visnes H, Bahr R. Training volume and body composition as risk factors for developing jumper's knee among young elite volleyball players. Scand J Med Sci Sports. 2012 Jan 20. [QxMD MEDLINE Link].
Zwerver J, Bredeweg SW, van den Akker-Scheek I. Prevalence of Jumper's knee among nonelite athletes from different sports: a cross-sectional survey. Am J Sports Med. 2011 Sep. 39(9):1984-8. [QxMD MEDLINE Link].
Jonsson P, Alfredson H. Superior results with eccentric compared to concentric quadriceps training in patients with jumper's knee: a prospective randomised study. Br J Sports Med. 2005 Nov. 39(11):847-50. [QxMD MEDLINE Link].
Van der Worp H, de Poel HJ, Diercks RL, van den Akker-Scheek I, Zwerver J. Jumper's knee or lander's knee? A systematic review of the relation between jump biomechanics and patellar tendinopathy. Int J Sports Med. 2014 Jul. 35 (8):714-22. [QxMD MEDLINE Link].
Scott A, Lian O, Bahr R, et al. Elevated mast cell numbers in human patellar tendinosis: correlation with symptom duration and vascular hyperplasia. Br J Sports Med. 2008 Mar 4. epub ahead of print. [QxMD MEDLINE Link]. [Full Text].
Hamilton B, Purdam C. Patellar tendinosis as an adaptive process: a new hypothesis. Br J Sports Med. 2004 Dec. 38(6):758-61. [QxMD MEDLINE Link]. [Full Text].
Warden SJ, Kiss ZS, Malara FA, et al. Comparative accuracy of magnetic resonance imaging and ultrasonography in confirming clinically diagnosed patellar tendinopathy. Am J Sports Med. 2007 Mar. 35(3):427-36. [QxMD MEDLINE Link].
Alfredson H, Ohberg L. Neovascularisation in chronic painful patellar tendinosis--promising results after sclerosing neovessels outside the tendon challenge the need for surgery. Knee Surg Sports Traumatol Arthrosc. 2005 Mar. 13(2):74-80. [QxMD MEDLINE Link].
Gisslén K, Alfredson H. Neovascularisation and pain in jumper's knee: a prospective clinical and sonographic study in elite junior volleyball players. Br J Sports Med. 2005 Jul. 39(7):423-8; discussion 423-8. [QxMD MEDLINE Link]. [Full Text].
Johnson DP, Wakeley CJ, Watt I. Magnetic resonance imaging of patellar tendonitis. J Bone Joint Surg Br. 1996 May. 78(3):452-7. [QxMD MEDLINE Link]. [Full Text].
Khan KM, Bonar F, Desmond PM, et al. Patellar tendinosis (jumper's knee): findings at histopathologic examination, US, and MR imaging. Victorian Institute of Sport Tendon Study Group. Radiology. 1996 Sep. 200(3):821-7. [QxMD MEDLINE Link]. [Full Text].
Hoksrud A, Ohberg L, Alfredson H, Bahr R. Ultrasound-guided sclerosis of neovessels in painful chronic patellar tendinopathy: a randomized controlled trial. Am J Sports Med. 2006 Nov. 34(11):1738-46. [QxMD MEDLINE Link].
Kongsgaard M, Aagaard P, Roikjaer S, et al. Decline eccentric squats increases patellar tendon loading compared to standard eccentric squats. Clin Biomech (Bristol, Avon). 2006 Aug. 21(7):748-54. [QxMD MEDLINE Link].
Purdam CR, Jonsson P, Alfredson H, Lorentzon R, Cook JL, Khan KM. A pilot study of the eccentric decline squat in the management of painful chronic patellar tendinopathy. Br J Sports Med. 2004 Aug. 38(4):395-7. [QxMD MEDLINE Link]. [Full Text].
Bahr R, Fossan B, Løken S, Engebretsen L. Surgical treatment compared with eccentric training for patellar tendinopathy (jumper's knee). A randomized, controlled trial. J Bone Joint Surg Am. 2006 Aug. 88(8):1689-98. [QxMD MEDLINE Link].
Pestka JM, Lang G, Maier D, Südkamp NP, Ogon P, Izadpanah K. Arthroscopic patellar release allows timely return to performance in professional and amateur athletes with chronic patellar tendinopathy. Knee Surg Sports Traumatol Arthrosc. 2018 May 27. [QxMD MEDLINE Link].
Lang G, Pestka JM, Maier D, Izadpanah K, Südkamp N, Ogon P. Arthroscopic patellar release for treatment of chronic symptomatic patellar tendinopathy: long-term outcome and influential factors in an athletic population. BMC Musculoskelet Disord. 2017 Nov 22. 18 (1):486. [QxMD MEDLINE Link].
Abate M, Di Carlo L, Verna S, Di Gregorio P, Schiavone C, Salini V. Synergistic activity of platelet rich plasma and high volume image guided injection for patellar tendinopathy. Knee Surg Sports Traumatol Arthrosc. 2018 Mar 31. [QxMD MEDLINE Link].
Zayni R, Thaunat M, Fayard JM, Hager JP, Carrillon Y, Clechet J, et al. Platelet-rich plasma as a treatment for chronic patellar tendinopathy: comparison of a single versus two consecutive injections. Muscles Ligaments Tendons J. 2015 Apr-Jun. 5 (2):92-8. [QxMD MEDLINE Link].
Fredberg U, Bolvig L, Pfeiffer-Jensen M, et al. Ultrasonography as a tool for diagnosis, guidance of local steroid injection and, together with pressure algometry, monitoring of the treatment of athletes with chronic jumper's knee and Achilles tendinitis: a randomized, double-blind, placebo-controll... Scand J Rheumatol. 2004. 33(2):94-101.
Coombes BK, Bisset L, Vicenzino B. Efficacy and safety of corticosteroid injections and other injections for management of tendinopathy: a systematic review of randomised controlled trials. Lancet. 2010 Nov 20. 376(9754):1751-67. [QxMD MEDLINE Link].
James SL, Ali K, Pocock C, et al. Ultrasound guided dry needling and autologous blood injection for patellar tendinosis. Br J Sports Med. 2007 Aug. 41(8):518-21; discussion 522. [QxMD MEDLINE Link].
Hoksrud A, Torgalsen T, Harstad H, Haugen S, Andersen TE, Risberg MA. Ultrasound-guided sclerosis of neovessels in patellar tendinopathy: a prospective study of 101 patients. Am J Sports Med. 2012 Mar. 40(3):542-7. [QxMD MEDLINE Link].
Hoksrud A, Bahr R. Ultrasound-guided sclerosing treatment in patients with patellar tendinopathy (jumper's knee). 44-month follow-up. Am J Sports Med. 2011 Nov. 39(11):2377-80. [QxMD MEDLINE Link].
Peers KH, Lysens RJ, Brys P, Bellemans J. Cross-sectional outcome analysis of athletes with chronic patellar tendinopathy treated surgically and by extracorporeal shock wave therapy. Clin J Sport Med. 2003 Mar. 13(2):79-83. [QxMD MEDLINE Link].
Zwerver J, Hartgens F, Verhagen E, van der Worp H, van den Akker-Scheek I, Diercks RL. No effect of extracorporeal shockwave therapy on patellar tendinopathy in jumping athletes during the competitive season: a randomized clinical trial. Am J Sports Med. 2011 Jun. 39(6):1191-9. [QxMD MEDLINE Link].
Furia JP, Rompe JD, Cacchio A, Del Buono A, Maffulli N. A single application of low-energy radial extracorporeal shock wave therapy is effective for the management of chronic patellar tendinopathy. Knee Surg Sports Traumatol Arthrosc. 2013 Feb. 21 (2):346-50. [QxMD MEDLINE Link].
Vetrano M, Castorina A, Vulpiani MC, Baldini R, Pavan A, Ferretti A. Platelet-Rich Plasma Versus Focused Shock Waves in the Treatment of Jumper's Knee in Athletes. Am J Sports Med. 2013 Feb 13. [QxMD MEDLINE Link].
Grambart ST. Sports medicine and platelet-rich plasma: nonsurgical therapy. Clin Podiatr Med Surg. 2015 Jan. 32 (1):99-107. [QxMD MEDLINE Link].
Dragoo JL, Wasterlain AS, Braun HJ, Nead KT. Platelet-rich plasma as a treatment for patellar tendinopathy: a double-blind, randomized controlled trial. Am J Sports Med. 2014 Mar. 42 (3):610-8. [QxMD MEDLINE Link].
Smith J, Sellon JL. Comparing PRP injections with ESWT for athletes with chronic patellar tendinopathy. Clin J Sport Med. 2014 Jan. 24 (1):88-9. [QxMD MEDLINE Link].
Andriolo L, Altamura SA, Reale D, Candrian C, Zaffagnini S, Filardo G. Nonsurgical Treatments of Patellar Tendinopathy: Multiple Injections of Platelet-Rich Plasma Are a Suitable Option: A Systematic Review and Meta-analysis. Am J Sports Med. 2018 Mar 1. 58 (1-2):363546518759674. [QxMD MEDLINE Link].
Abat F, Sánchez-Sánchez JL, Martín-Nogueras AM, Calvo-Arenillas JI, Yajeya J, Méndez-Sánchez R, et al. Randomized controlled trial comparing the effectiveness of the ultrasound-guided galvanic electrolysis technique (USGET) versus conventional electro-physiotherapeutic treatment on patellar tendinopathy. J Exp Orthop. 2016 Dec. 3 (1):34. [QxMD MEDLINE Link].
Nanos KN, Malanga GA. Treatment of Patellar Tendinopathy Refractory to Surgical Management Using Percutaneous Ultrasonic Tenotomy and Platelet-Rich Plasma Injection: A Case Presentation. PM R. 2015 Dec. 7 (12):1300-5. [QxMD MEDLINE Link].
Al-Duri ZA, Aichroth PM. Surgical aspects of patellar tendonitis: technique and results. Am J Knee Surg. 2001 Winter. 14(1):43-50. [QxMD MEDLINE Link].
Cook JL, Khan KM, Harcourt PR, Grant M, Young DA, Bonar SF. A cross sectional study of 100 athletes with jumper's knee managed conservatively and surgically. The Victorian Institute of Sport Tendon Study Group. Br J Sports Med. 1997 Dec. 31(4):332-6. [QxMD MEDLINE Link]. [Full Text].
Lian Ø, Scott A, Engebretsen L, et al. Excessive apoptosis in patellar tendinopathy in athletes. Am J Sports Med. 2007 Apr. 35(4):605-11. [QxMD MEDLINE Link].
Matheson GO. Long-term prognosis for jumper's knee. Clin J Sport Med. 2003 May. 13(3):196. [QxMD MEDLINE Link].
Medlar RC, Lyne ED. Sinding-Larsen-Johansson disease. Its etiology and natural history. J Bone Joint Surg Am. 1978 Dec. 60(8):1113-6. [QxMD MEDLINE Link]. [Full Text].
Ogden JA, Southwick WO. Osgood-Schlatter's disease and tibial tuberosity development. Clin Orthop Relat Res. 1976 May. 116:180-9. [QxMD MEDLINE Link].
Roels J, Martens M, Mulier JC, Burssens A. Patellar tendinitis (jumper's knee). Am J Sports Med. 1978 Nov-Dec. 6(6):362-8. [QxMD MEDLINE Link].
Magnani G, Calzetti C, Campari M, Lehndorff H, Pizzaferri P, Rossi E. [Immune response to hepatitis B vaccine and duration of protection in a dialysis unit]. Acta Biomed Ateneo Parmense. 1987. 58 (1-2):41-7. [QxMD MEDLINE Link].
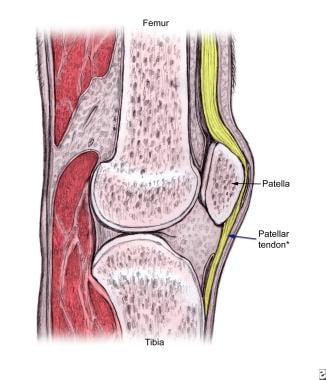 The proximal patellar tendon is most commonly affected in jumper's knee.
The proximal patellar tendon is most commonly affected in jumper's knee.



