Practice Essentials
The layman's term "jammed finger" often refers to injuries that are incurred around the proximal interphalangeal (PIP) joint of the fingers (see image below). Although imprecise in its diagnostic accuracy, jammed finger aptly describes a constellation of injuries that are related to varying degrees of axial loading across the PIP joint.
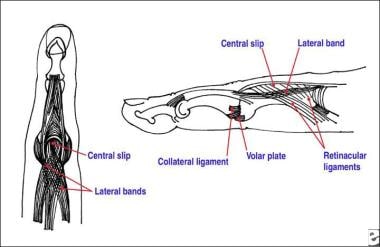 Anatomy of the proximal interphalangeal joint. The central slip passes directly over the joint and inserts on the base of the middle phalanx. The lateral bands pass around the joint, combine with the retinacular ligaments, and unite to form the extensor tendon that attaches on the distal phalanx. Lateral motion is minimized by the collateral ligaments, and extension is limited to 0º by the thick volar plate.
Anatomy of the proximal interphalangeal joint. The central slip passes directly over the joint and inserts on the base of the middle phalanx. The lateral bands pass around the joint, combine with the retinacular ligaments, and unite to form the extensor tendon that attaches on the distal phalanx. Lateral motion is minimized by the collateral ligaments, and extension is limited to 0º by the thick volar plate.
(See also the Medscape Reference articles Finger Nail and Tip Injuries, Interphalangeal Dislocations, Mallet Finger, Boutonniere Deformity, and Mallet Fracture.)
Injury to the PIP joint is common in athletic activities, especially ball-handling sports, but this condition is often minimized by players and coaches. [1] The anatomy of the PIP joint is complex, and several types of injuries can result in permanent disability if they are left undiagnosed or mistreated. The sports medicine practitioner must develop a working knowledge of these common injury patterns so that timely and appropriate treatment can be provided.
Epidemiology
United States statistics
Finger and hand injuries account for 12% of all injuries in American football players. [2]
International statistics
Finger injuries are common (38%) in individuals younger than 5 years. Most of these occur at home (59%), commonly (48%) because of jamming between 2 closeable opposing surfaces and mostly (79%) in doors at home and at school. [3]
A study by Gill et al of Australian football players who presented to the emergency department with a finger, hand, or wrist injury found that ball contact was the most common mechanism of injury (38% of injuries). [4]
Functional Anatomy
The PIP joint is a hinge joint that permits a range of motion (ROM) from 0-120° [5, 6, 7] (see image below). Relatively thick collateral ligaments provide lateral stability. Unlike the metacarpophalangeal (MCP) joint, the tension of these ligaments does not vary during ROM.
Anatomy of the proximal interphalangeal joint. The central slip passes directly over the joint and inserts on the base of the middle phalanx. The lateral bands pass around the joint, combine with the retinacular ligaments, and unite to form the extensor tendon that attaches on the distal phalanx. Lateral motion is minimized by the collateral ligaments, and extension is limited to 0º by the thick volar plate.
The volar plate forms the floor of the joint and separates the joint space from the flexor tendons. The volar plate is ligamentous at its origin on the proximal phalanx and cartilaginous in its insertion onto the middle phalanx.
Dorsally, the central slip of the extensor tendon acts to stabilize the joint and to extend the middle phalanx. The lateral bands, joined by the retinacular ligaments of the intrinsic hand muscles, go around the joint to form the distal extensor tendon and also contribute to joint stability.
The common mechanism of injury at the PIP joint involves the simultaneous application of hyperextension forces with some degree of longitudinal compression.
Volar plate disruption (see image below)
Mild forces may rupture the volar plate at its distal insertion on the middle phalanx; the articular surfaces remain intact. This is a stable injury. Local pain and edema generally produce only short-term disability.
Occasionally, fractures of the middle phalanx at the attachment of the volar plate occur. These fractures usually involve less than 30-40% of the joint surface and are thought to be stable due to maintenance of collateral ligament integrity. (See also the Medscape Reference article Phalangeal Fracture Surgery.)
 Volar plate disruption with a stable, nondisplaced avulsion fracture of the middle phalanx.
Volar plate disruption with a stable, nondisplaced avulsion fracture of the middle phalanx.
Dorsal dislocation (see image below)
If the force of injury is great enough, rupture of the volar plate may occur along with longitudinal splitting in the collateral ligament structures, allowing complete dorsal displacement of the middle phalanx. Simple dislocations are readily reduced, often by the player, coach, or trainer on the field. Following reduction, most dorsal dislocations are stable.
Fractures at the base of the middle phalanx also occur in association with dorsal dislocations. If a fracture involves more than 40-50% of the articular surface, collateral ligament support is lost. Combined with the coexistent volar plate disruption, this reduction of collateral ligament support represents a major loss of joint stability. These injuries are often unstable, exhibiting persistent subluxation of the middle phalanx.

Collateral ligament injury
Angular forces may cause partial or complete rupture of a collateral ligament. When combined with volar plate rupture, lateral dislocation can occur. Most lateral dislocations are easily reduced and do not demonstrate gross instability.
Because of scar-tissue formation in the healing ligament, these injuries often result in enlargement of the PIP joint ("fat knuckle"). This may be of cosmetic concern to some patients, but good functional recovery can usually be expected.
Boutonniere deformity (see image below)
The term "boutonniere" comes from the French word for "buttonhole." This injury involves a disruption of the central slip of the extensor tendon at its insertion on the middle phalanx. The mechanism of injury is a blow to the dorsum of the PIP joint, such as when an athlete's hand is stepped on. Occasionally, a small fleck fracture of the middle phalanx is seen at the central slip insertion. Volar dislocation of the PIP joint is thought to be a component in many cases.
Little deformity may be noted immediately after an injury that results in a boutonniere deformity. The lateral bands may still act weakly to aid joint extension. Left untreated, the central slip retracts and the lateral bands displace volarly below the axis of rotation, becoming flexors of the PIP joint. Thus, the classic deformity of PIP joint flexion and distal interphalangeal (DIP) joint hyperextension is produced. Once a deformity becomes chronic or fixed, it presents a difficult surgical challenge, with potentially permanent functional deficits.
Because volar dislocations may be reduced spontaneously or before the office visit and because the symptoms and signs of such injuries may be subtle, practitioners must maintain a high index of suspicion for central slip disruption when evaluating any PIP joint injury. Patients may have more pain dorsally, and there is usually weakness or the inability to fully extend the PIP joint.

Prognosis
The prognosis for a jammed finger is excellent with the proper treatment and protection.
A study by Cheesman et al found that 63% of patients with a PIP joint sprain had complete resolution of swelling within 1 year. [8]
Complications
Possible complications that follow a PIP joint injury include the following [9] :
-
Persistent pain and swelling
-
Stiffness
-
Weakness
-
Instability
-
Boutonniere deformity
-
Anatomy of the proximal interphalangeal joint. The central slip passes directly over the joint and inserts on the base of the middle phalanx. The lateral bands pass around the joint, combine with the retinacular ligaments, and unite to form the extensor tendon that attaches on the distal phalanx. Lateral motion is minimized by the collateral ligaments, and extension is limited to 0º by the thick volar plate.
-
Volar plate disruption with a stable, nondisplaced avulsion fracture of the middle phalanx.
-
Dorsal dislocation of the proximal interphalangeal joint.
-
Typical boutonniere deformity.
-
Extension block splint with the proximal interphalangeal joint at 30°.
-
Proximal interphalangeal joint that has been splinted in extension for the treatment of a central slip injury.
-
Dynamic spring extension splint for the treatment of a boutonniere finger deformity.






