Practice Essentials
The ankle joint is the most commonly injured joint in sports. [1, 2, 3] In the United States, approximately 70% of basketball players have sprained an ankle, and the likelihood of reinjury is as high as 80%. [4] Lateral ankle sprains account for 90% of all ankle injuries, whereas an ankle fracture occurs only approximately 15% of the time. [5, 6, 7]
Ankle injuries are caused by acute trauma.
Functional Anatomy
The distal tibia, distal fibula, and talus bones make up the ankle joint. These 3 bones are bound together by the joint capsule and surrounding ligaments. The anatomic relationship of the tibial plafond (joint surface of the distal tibia) to the talus is important for ankle stability. Because the anterior portion of the talus is more broadly shaped, dorsiflexion increases bone surface contact, thus improving stability. This relationship causes decreased stability during plantarflexion, accounting for the vulnerability to ligamentous injuries when the foot is plantarflexed. [8] See the image below.
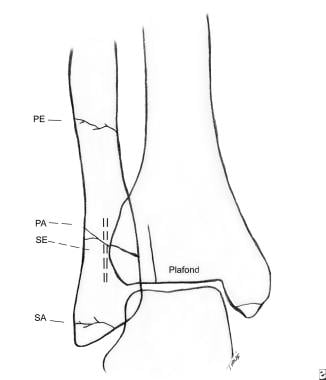 Diagram showing the typical locations for ankle fractures occurring from the 4 major injury mechanisms (SA= supination adduction, SE= supination external rotation, PA= pronation abduction, PE= pronation external rotation). Note that the SE fracture is shown as a dashed line, since it is best seen in the lateral projection.
Diagram showing the typical locations for ankle fractures occurring from the 4 major injury mechanisms (SA= supination adduction, SE= supination external rotation, PA= pronation abduction, PE= pronation external rotation). Note that the SE fracture is shown as a dashed line, since it is best seen in the lateral projection.
Sport-Specific Biomechanics
Forces acting on the ankle lead to typical fracture or ligamentous patterns. Determining the position of the ankle during the injury can assist in assessing for ligament stability. Although simple unidirectional forces can be involved in an ankle injury, multidirectional forces are usually involved, making diagnosis a challenge.
Medial complex injuries typically occur from eversion and abduction forces. The medial complex consists of the medial malleolus, the medial facet of the talus, and the superficial and deep components of the deltoid ligament. Eversion of the ankle causes injury to the superficial deltoid ligaments and, if sufficient, the deep deltoid ligament. Avulsion of the distal medial malleolus tends to occur in young and old patients, because the ligamentous strength may be greater than the strength of the bone in these individuals. With continuation of these forces, impaction of the distal lateral malleolus occurs, resulting either in rupture of the syndesmosis or in transverse fracture of the distal fibula. [8]
Most unstable ankle fractures are the result of excessive external rotation of the talus with respect to the tibia. If the foot is supinated at the time of external rotation, an oblique fracture of the fibula ensues. If the foot is pronated at the time of external rotation, a mid- or high-fibular fracture results.
The lateral complex consists of the distal fibula, the lateral facet of the talus, and the lateral collateral ligaments of the ankle and subtalar joints. Lateral malleolus injury (most common type of fracture involving the ankle) typically occurs with supination external rotation forces. The inversion force first strains the lateral ligament complex or avulses (transverse fracture) the lateral malleolus. With continuation of this force, the talus impacts the medial malleolus, causing an oblique fracture of the distal tibia. Inversion ligamentous injuries of the ankle are the most commonly observed soft-tissue trauma in sports.
Posterior malleolus injury typically occurs with a supination-external rotation or a pronation-external rotation injury and represents avulsion of the posterior tibiofibular ligament from the posterior distal tibia.
-
Diagram showing the typical locations for ankle fractures occurring from the 4 major injury mechanisms (SA= supination adduction, SE= supination external rotation, PA= pronation abduction, PE= pronation external rotation). Note that the SE fracture is shown as a dashed line, since it is best seen in the lateral projection.









