Practice Essentials
Muscle contusion indicates a direct, blunt, compressive force to a muscle. Contusions are one of the most common sports-related injuries. [1, 2, 3, 4] The severity of contusions ranges from simple skin contusions to muscle and bone contusions to internal organ contusions.
Any blunt trauma with sufficient force to propel its energy into the muscle can cause a contusion. Contusions are often the result of sports-related injuries. Education about the proper use of protective equipment and aggressive early treatment of contusions is essential. (See the image below.)
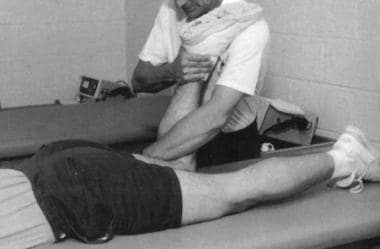 Modified treatment of quadriceps contusion. Used with permission courtesy of John Aronen, MD.
Modified treatment of quadriceps contusion. Used with permission courtesy of John Aronen, MD.
Although all tissue and organ contusions can result from traumatic sports injury, this article focuses on muscle contusions. Contusions of internal organs and bone contusions are not discussed in this article (see the Medscape Reference articles Concussion, Sacroiliac Joint Injury, Femur Injuries and Fractures, and Hip Pointer).
Signs and symptoms
Contusion symptoms include the following:
-
Soreness
-
Pain with active range of motion and passive range of motion
-
Limited range of motion
See Presentation for more detail.
Diagnosis
In most cases of contusions, extensive workup is unnecessary and unwarranted.
If the initial history and physical examination merit further evaluation, radiographs of the traumatized region may help rule out a fracture.
Magnetic resonance imaging (MRI) is rapidly becoming the imaging modality of choice for soft-tissue injuries. However, use of this imaging tool tends to be limited to the professional athlete, to those patients in whom the diagnosis is in doubt, and in those whose symptoms are not responding to therapy
See Workup for more detail.
Management
In the acute phase following a muscle contusion, hematoma maturation, inflammation, necrosis of damaged myofibrils, and phagocytosis of the necrotic debris are main features. The goal of therapy is to minimize hemorrhage and inflammation and control pain.
See Treatment and Medication for more detail.
Epidemiology
United States statistics
Contusions and strain injuries comprise approximately 60-70% of all sports-related injuries. In addition, most contusion injuries go unreported and untreated. Documented muscle contusions account for one third of all sports injuries. The quadriceps and gastrocnemius muscle groups are most often involved (see the images below). [5, 6, 7, 8]
A study that compared incidence, duration of absence and characteristics of indirect (strain) and direct (contusion) quadriceps and hamstring muscle injuries reported that these thigh injuries are more frequent than have been previously described. Direct injuries (contusion) are less frequent than indirect ones (strain), and players can usually return to full activity in under half the average time for an indirect injury. [9]
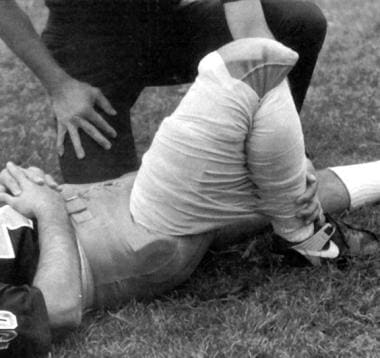 Athlete with a quadriceps strain. Place knee passively in 120º of flexion and immobilize with a double elastic wrap in a figure-8 fashion. This should occur within minutes of the injury. Used with permission courtesy of John Aronen, MD.
Modified treatment of quadriceps contusion. Used with permission courtesy of John Aronen, MD.
Athlete with a quadriceps strain. Place knee passively in 120º of flexion and immobilize with a double elastic wrap in a figure-8 fashion. This should occur within minutes of the injury. Used with permission courtesy of John Aronen, MD.
Modified treatment of quadriceps contusion. Used with permission courtesy of John Aronen, MD.
Rotator cuff contusions of the shoulder have also been seen in professional football players. Cohen et al evaluated the incidence, treatment, and magnetic resonance imaging (MRI) appearance of players sustaining such injuries in a North American professional football team. [10] . The team's injury records from 1999 to 2005 were retrospectively reviewed for athletes who had sustained a rotator cuff contusion of the shoulder during in-season participation.
The investigators reported 26 players had a rotator cuff contusion, with an average of 5.5 rotator cuff contusions per season (47% of all shoulder injuries), 70.3% of which the predominant mechanism of injury was a direct blow. MRI findings included peritendon edema at the myotendinous junction, critical zone tendon edema, and subentheseal bone bruises. [10]
All patients were treated with a protocol involving modalities and cuff rehabilitation; 6 patients had persistent pain and weakness for at least 3 days and were given a subacromial corticosteroid injection. Overall, 3 patients (11.4%) required later surgical treatment on the shoulder. [10]
Cohen et al determined that rotator cuff contusions composed nearly half of all shoulder injuries in the football players in their study, [10] but the majority of affected athletes are able to return to sports with conservative treatment. A minority of shoulders might progress to more severe injuries such as rotator cuff tears. See the images below.

 In this patient's shoulder radiography, the humeral head no longer matches up with the glenoid because the rotator cuff is torn and the strong deltoid muscle is pulling the head superiorly toward the acromion. Courtesy of Dr Thomas Murray, Orthopaedic Associates of Portland.
In this patient's shoulder radiography, the humeral head no longer matches up with the glenoid because the rotator cuff is torn and the strong deltoid muscle is pulling the head superiorly toward the acromion. Courtesy of Dr Thomas Murray, Orthopaedic Associates of Portland.
International statistics
The international frequency of contusions is similar to that in the United States.
A European study of soccer players found that many muscle injuries of the anterior thigh are direct contusions, which may occur during collisions. In players who sustain direct contusions, the most frequently involved muscles are the vastus intermedius, vastus lateralis, and vastus medialis. [11]
A meta-analysis by Horan et al showed that the time-loss injury incidence rate among European women’s elite club football players who had sustained contusions was 0.76/1000 hours. [12]
Functional Anatomy
Skeletal muscle constitutes the largest tissue mass in the body, comprising up to 45% of the total body weight. Muscles that cross a single joint are located close to bone, are frequently responsible for postural maintenance, and are most susceptible to contusions. On the other hand, 2-joint muscles, such as the rectus femoris muscle, lie more superficial and are more susceptible to stretch-induced strain injury.
Contusions are caused by blunt trauma to the outer aspect of the muscle, resulting in tissue and cellular damage and bleeding deep within the muscle and between the muscle planes. [1] The resultant tissue necrosis and hematoma lead to inflammation. [13] Little is known about the role of the inflammatory process and its importance in the healing process. Clearly, too much inflammation is unfavorable, but too little may be just as devastating.
A bruise is caused by blood that has escaped from damaged capillaries into the interstitial tissues. Within a few hours after the injury, the presence of necrotic tissue and hematoma initiates an inflammatory reaction. Because inflammation initiates macrophage action with subsequent phagocytosis of necrotic debris and stimulation of capillary production, it is vital to the process of muscle regeneration. However, inflammation invariably causes edema that leads to anoxia and further cell death.
Findings from an experimental model of contusion injury in humans support the role of edema in contusion-related pain. Barnes et al demonstrated that as the volume of edema increases, the site of the injury becomes more painful. [4]
The extent of the inflammatory response is often considered excessive and detrimental to muscle regeneration. However, controversy exists regarding this theory, because some literature indicates a worsened long-term outcome in patients placed on anti-inflammatory medications. Controversy also surrounds cryotherapy, with some literature touting its benefits, whereas others question its utility. [14, 15, 16]
Prognosis
For most muscle contusions, the prognosis is excellent. Jackson and Feagin's research on thigh contusions found the average disability time was 13 days for mild contusions, 19 days for moderate contusions, and 21 days for severe contusions. [5]
Risk factors for a more unfavorable prognosis include injuries that occur during football, previous contusion in the same muscle, delay in treatment for more than 3 days, and large muscle involvement. Reinjury is a significant factor in prolonging disability.
Complications
Myositis ossificans occurs in 9% of all contusions, 4% of mild contusions, 13% of moderate contusions, and 18% of severe contusions. Development of myositis ossificans is a multifactorial problem. Reinjury is a significant factor in prolonging disability.
The incidence of myositis ossificans among athletes, especially those who participate in contact sports, is estimated to range from 9% to 20% after upper leg contusions. Nieuwenhuizen et al reported the case of a football player who developed myositis ossificans of the lower leg following a traumatic injury to the site. [17]
Rhabdomyolysis must be considered if the contusions are extensive or multiple.
The most serious complication is compartment syndrome. Pain out of proportion to the injury or increasing pain over time are red flags that should alert and prompt the physician to measure the compartment pressures. See the images below.
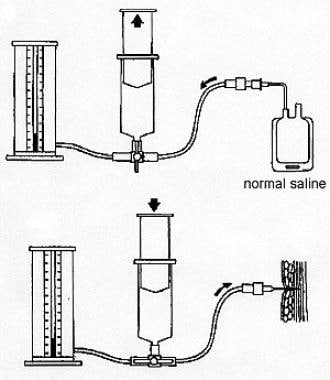 Picture of compartment pressure measuring device for use when commercial devices are unavailable.
Picture of compartment pressure measuring device for use when commercial devices are unavailable.
 Stryker STIC Monitor. Image courtesy of Stryker Corporation, used with permission.
Stryker STIC Monitor. Image courtesy of Stryker Corporation, used with permission.
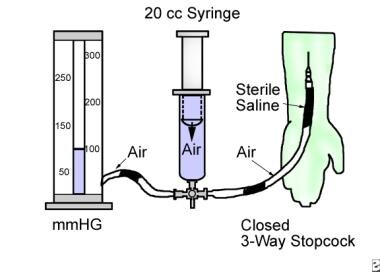 An illustration that depicts measurement of compartment pressures in the forearm.
An illustration that depicts measurement of compartment pressures in the forearm.
-
Athlete with a quadriceps strain. Place knee passively in 120º of flexion and immobilize with a double elastic wrap in a figure-8 fashion. This should occur within minutes of the injury. Used with permission courtesy of John Aronen, MD.
-
Modified treatment of quadriceps contusion. Used with permission courtesy of John Aronen, MD.
-
Rotator cuff injury.
-
In this patient's shoulder radiography, the humeral head no longer matches up with the glenoid because the rotator cuff is torn and the strong deltoid muscle is pulling the head superiorly toward the acromion. Courtesy of Dr Thomas Murray, Orthopaedic Associates of Portland.
-
Lateral view of the neck showing calcification in the paraspinal muscles. Image contributed by Ajay K. Singh, MD, William Beaumont Hospital, Royal Oak, Mich.
-
A 6-year-old girl who presents a few days after being disciplined on the buttocks with a wooden spoon by her mother. This pattern of bruises is of suspicious shape, number, and location.
-
Picture of compartment pressure measuring device for use when commercial devices are unavailable.
-
Stryker STIC Monitor. Image courtesy of Stryker Corporation, used with permission.
-
An illustration that depicts measurement of compartment pressures in the forearm.
-
Anteroposterior radiograph of the right hip in a 16-year-old boy who had suffered trauma to the hip 2 years previously (same patient in Images 10-11). The patient is currently experiencing hip pain. Mature heterotopic ossification (arrowheads) projects over and lateral to the femoral head.
-
Corresponding lateral view of the right hip (same patient in Images 10-11). Distal to the mature heterotopic ossification (HO) seen on the anteroposterior view (arrowheads) is a subtle area of early mineralization (arrows) consistent with early HO.






