Practice Essentials
Neck pain is common in the general population and even more common in a chronic pain management practice. Very few reliable epidemiologic studies regarding the prevalence of neck pain exist; however, a Finnish study [1] and a Norwegian study [2] estimated the prevalence of neck pain in the general population to be approximately 34%. In a Swedish study, 29% of elderly men reported neck pain. [3] Furthermore, the prevalence of chronic neck pain, defined as lasting 6 months or longer, is estimated at approximately 14%. [1, 2]
In 1933, Ghormley coined the term facet syndrome to describe a constellation of symptoms associated with degenerative changes of the lumbar spine. [4] Relatively recently, the term cervical facet syndrome has appeared in the literature and implies axial pain presumably secondary to involvement of the posterior elements of the cervical spine. See the image below.
Many pain generators are located in the cervical spine, including the intervertebral discs, facet joints, ligaments, muscles, and nerve roots. The facet joints have been found to be a possible source of neck pain, and the diagnosis of cervical facet syndrome is often one of exclusion or not considered at all.
Clinical features that are often, but not always, associated with cervical facet pain include tenderness to palpation over the facet joints or paraspinal muscles, pain with cervical extension or rotation, and absent neurologic abnormalities. [5] Imaging studies usually are not helpful, with the exception of ruling out other sources of pain, such as fractures or tumors. Signs of cervical spondylosis, narrowing of the intervertebral foramina, osteophytes, and other degenerative changes are equally prevalent in people with and without neck pain. [6]
Etiology
Bogduk and Marsland studied patients with neck pain without objective neurologic signs to determine if the facet joints were the primary source of their pain. [7] Twenty-four consecutive patients presenting at a pain clinic with neck pain of unknown origin were entered into the study. Those with lower cervical spine pain underwent C5 and C6 medial branch blocks first. If these medial branch blocks did not provide relief, then adjacent levels were blocked until the pain was relieved. Those with upper cervical spine pain underwent third occipital nerve blocks, and then C3 and C4 medial branch blocks if necessary. Bupivacaine was used as the blocking agent and a positive response was considered total pain relief for at least 2 hours. [7]
Fifteen patients experienced complete relief of their neck pain, and repeat blocks had the same effect. Seven of these patients underwent intra-articular facet joint blocks, corresponding to the levels determined by the medial branch blocks, which also completely relieved their pain. [7] No clinical or radiologic features corresponded with the positive responses. This finding suggests that facet joints in the cervical spine can be a significant source of neck pain and that medial branch blocks can be used as both diagnostic and therapeutic tools in the management of this type of pain. [7]
Each facet joint seems to have a particular radiation pattern upon painful stimulation. Even in subjects without neck pain, stimulation of the facet joints by injecting contrast material into the joints and distending the capsule produces neck pain in a specific pattern corresponding to the specific joint.
In a study of 5 such subjects, joint pain referral patterns were mapped out. [8] The C2-C3 facet joint refers pain to the posterior upper cervical region and head, whereas the C3-C4 facet joint refers pain to the posterolateral cervical region without extension into the head or shoulder. The C4-C5 joint refers pain to the posterolateral middle and lower cervical region, and to the top of the shoulder. The C5-C6 joint refers pain to the posterolateral middle and primarily lower cervical spine and the top and lateral parts of the shoulder and caudally to the spine of the scapula. The C6-C7 joint refers pain to the top and lateral parts of the shoulder and extends caudally to the inferior border of the scapula.
These pain referral maps were subsequently used to predict the segmental origin of neck pain in 10 symptomatic patients, who were referred for radiologic evaluation of possible facet joint pain. [9] Each of these patients was interviewed before the procedure and recorded the distribution of their pain on a diagram. These diagrams were compared with the maps previously generated from the asymptomatic subjects, and the facet joint or joints thought to be responsible for the pain patterns were predicted. Afterward, the patients underwent diagnostic facet joint nerve blocks at the predicted levels, and the pain was completely relieved in all but one patient. [9] This result suggests that these pain referral maps may be a powerful diagnostic tool when evaluating patients with cervical pain.
Facet joint pain referral patterns have also been documented in the OA joint and the lateral AA joint. Dreyfuss et al studied 5 asymptomatic subjects and injected the right AA joint and the left OA joint in each participant with contrast medium to distend the capsule. [10] The resultant pain referral patterns for the AA joints were similar and located posterior and lateral to the C1-C2 segments. The patterns for the OA joints were variable and extended from the vertex of the skull to the C5 segment. Perceived pain was also greater with the OA injections compared with the AA injections. Pain referral patterns have also been documented in symptomatic patients and correspond well to those obtained from asymptomatic subjects. [11]
Fukui et al created pain referral patterns from the OA facet joint to the C7-T1 joint. [5] The investigators studied 61 patients with neck pain and stimulated the painful joints by the following 2 methods: injection of contrast medium into the joints and electrical stimulation of the medial branches. Two separate pain referral maps were constructed, and the facet joints and their corresponding medial branches correlated relatively well. [5]
Windsor et al electrically stimulated the medial branches of the C3-C8 posterior primary rami with or without the third occipital nerve in 9 subjects. [12] This study demonstrated that the medial branch and third occipital nerve, when stimulated individually, have a separate and distinct referral pattern from the facet joint referral patterns previously mentioned. These medial branch referral maps may provide additional insight in the evaluation of patients with suboccipital, cervical, or shoulder girdle pain.
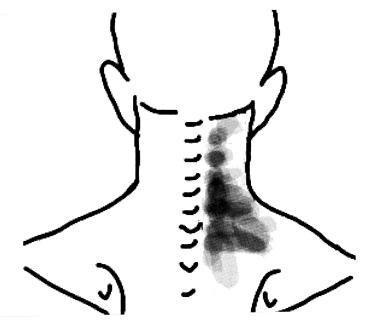 A composite drawing of the referral patterns of 9 subjects derived from the minimal threshold stimulation of their right occipital nerve and C3-C8 medial branches
A composite drawing of the referral patterns of 9 subjects derived from the minimal threshold stimulation of their right occipital nerve and C3-C8 medial branches
Epidemiology
United States statistics
Aprill and Bogduk estimated the prevalence of cervical facet joint pain by reviewing the records of patients who had presented with neck pain for at least 6 months secondary to some type of injury. [13] These patients underwent discography, facet joint nerve blocks, or both at the request of the referring physicians.
A total of 318 patients were investigated, and 26% of the patients had at least one symptomatic facet joint. However, only 126 patients of the original study group had their facet joints investigated, and 65% of these patients had painful facet joints. [13] Furthermore, 62% of the patients who underwent both discography and facet joint nerve blocks had painful facet joints. This study indicated that the prevalence of cervical facet joint pain may be as low as 26% or as high as 65%, depending on how aggressively it is sought. [13]
A large study by Manchikanti et al involved 500 patients with chronic, nonspecific spine pain. The prevalence of facet joint pain was determined using controlled comparative local anesthetic blocks with 1% lidocaine followed by 0.25% bupivacaine. [14] This study indicated that the prevalence of cervical facet joint pain was 55%. A more recent study by Manchikanti et al showed that the prevalence of cervical facet joint pain was 49.3% among patients who presented with chronic neck pain. [15]
It seems apparent that the cervical facet joints may be a common source of neck pain; however, there are other pain generators in the cervical spine, such as the intervertebral discs, that may be involved as well. To evaluate the contribution of the disc to neck pain, a sample of 56 patients were selected from participants in the earlier study by Manchikanti et al. This group consisted of patients who had undergone both discography and facet joint nerve blocks at the same segment of the cervical spine as part of the diagnostic process. [16]
The results demonstrated that 41% of this group had a painful disc and facet joint at the same segment, and an additional 23% had a painful facet joint but not a painful disc at the same segment. [16] Therefore, most of the sample had a painful facet joint, but there was often a painful disc at the same level. This finding is not surprising when one considers how the facet joints and discs are intimately involved in motion of the cervical spine.
Cervical facet joint pain is a common sequela of whiplash injury. Barnsley and Lord et al studied the prevalence of chronic cervical facet joint pain after whiplash injury using double-blind, controlled, diagnostic blocks of the facet joints. [17] The joints were blocked randomly with either a short-acting or long-acting anesthetic, and, if complete pain relief was obtained, the joint was blocked with the other agent 2 weeks later. Of the 38 patients who completed the trial, 27 obtained complete relief from both anesthetics and longer relief from the longer acting agent. [17] Therefore, the prevalence of this sample is 54%, making cervical facet joint pain the most common cause of chronic neck pain after whiplash injury in this population.
Lord and Barnsley et al subsequently studied the prevalence of chronic cervical facet joint pain after whiplash injury using a double-blind, placebo-controlled protocol. [18] The sample consisted of 68 consecutive patients referred for neck pain secondary to a motor vehicle accident and longer than 3 months in duration. Those individuals with a predominant headache underwent a third occipital nerve block and were removed from the study if they received pain relief. [18] The third occipital nerve has a cutaneous branch and a branch to the C2-C3 facet joint; therefore, patients with pain from this segment could not participate in the placebo study because they would feel the effects of the local anesthetic. The remaining 41 patients underwent diagnostic blocks with either a short-acting or a long-acting local anesthetic, followed by a second block with either normal saline or the other anesthetic, followed by a third block with the remaining agent.
The investigators reported the positive responders experienced complete relief with each anesthetic and no relief with the normal saline. The prevalence of cervical facet joint pain after whiplash injury was found to be 60%, and the most common levels were C2-C3 and C5-C6.
Neck pain is increased in patients with primary headache, according to one study. The authors assessed the prevalence of neck pain in patients with migraine (M), tension-type headache (TTH), or both migraine and TTH (M+TTH) and found that prevalence is highest in coexistent M+TTH, followed by pure TTH and migraine. In comparison with those without headaches, the prevalence of neck pain was significantly higher in those with M+TTH (89.3%), pure TTH (88.4%), and pure migraine (76.2%). In patients without primary headache, the prevalence of neck pain was 56.7%. [19]
International statistics
To estimate the global burden of neck pain, a systematic review was performed on the prevalence, incidence, remission, duration, and mortality risk of neck pain. The global point prevalence of neck pain was 4.9%. Disability-adjusted life years increased from 23.9 million in 1990 to 33.6 million in 2010. Out of all 291 conditions studied in the Global Burden of Disease 2010 Study, neck pain ranked 4th highest in terms of disability as measured by years lived with disability (YLDs) and 21st in terms of overall burden. [20]
Functional Anatomy
The cervical spine is made up of the first 7 vertebrae and functions to provide mobility and stability to the head, while connecting it to the relative immobile thoracic spine (see the image below). The first 2 vertebral bodies are quite different from the rest of the cervical spine. The atlas, or C1, articulates superiorly with the occiput and inferiorly with the axis, or C2.
The atlas is ring-shaped and does not have a body, unlike the rest of the vertebrae. The body has become part of C2, and it is called the odontoid process, or dens. The atlas is made up of an anterior arch, a posterior arch, 2 lateral masses, and 2 transverse processes. The transverse foramen, through which the vertebral artery passes, is enclosed by the transverse process. On each lateral mass is a superior and inferior facet (zygapophyseal) joint. The superior articular facets are kidney-shaped, concave, and face upward and inward. These superior facets articulate with the occipital condyles, which face downward and outward. The relatively flat inferior articular facets face downward and inward to articulate with the superior facets of the axis.
The axis has a large vertebral body, which contains the fused remnant of the C1 body, the dens. The dens articulates with the anterior arch of the atlas via its anterior articular facet and is held in place by the transverse ligament. The axis is composed of a vertebral body, heavy pedicles, laminae, and transverse processes, which serve as attachment points for muscles. The axis articulates with the atlas by its superior articular facets, which are convex and face upward and outward.
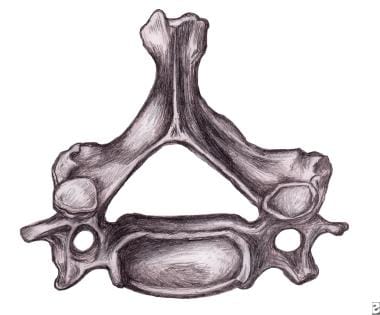
The remaining cervical vertebrae, C3-C7, are similar to each other, but they are very different from C1 and C2. They each have a vertebral body, which is concave on its superior surface and convex on its inferior surface. On the superior surfaces of the bodies are raised processes or hooks called uncinate processes, which articulate with depressed areas on the inferior aspect of the superior vertebral bodies called the echancrure or anvil. These uncovertebral joints are most noticeable near the pedicles and are usually referred to as the joints of Luschka. [21] These joints are believed to be the result of degenerative changes in the annulus, which leads to fissuring in the annulus and the creation of the joint. [22] The spinous processes of C3-C5 are usually bifid, in comparison to the spinous processes of C6 and C7, which are usually tapered.
The facet joints in the cervical spine are diarthrodial synovial joints with fibrous capsules. The joint capsules in the lower cervical spine are more lax compared with other areas of the spine to allow for gliding movements of the facets. The joints are inclined at 45° from the horizontal plane and angled 85° from the sagittal plane. This alignment helps to prevent excessive anterior translation and is important in weight bearing. [23]
The fibrous capsules are innervated by mechanoreceptors (types I, II, and III), and free nerve endings have been found in the subsynovial loose areolar and dense capsular tissues. [24] In fact, there are more mechanoreceptors in the cervical spine than in the lumbar spine. [25] This neural input from the facets may be important for proprioception and pain sensation and may modulate protective muscular reflexes that are important in preventing joint instability and degeneration.
The facet joints in the cervical spine are innervated by both the anterior and dorsal rami. The occipitoatlantal (OA) joint and atlantoaxial (AA) joint are innervated by the ventral rami of the first and second cervical spinal nerves. Two branches of the dorsal ramus of the third cervical spinal nerve innervate the C2-C3 facet joint, a communicating branch and a medial branch known as the third occipital nerve.
The remaining cervical facets, C3-C4 to C7-T1, are supplied by the dorsal rami medial branches that arise one level cephalad and caudad to the joint. [26, 27, 28] Therefore, each joint from C3-C4 to C7-T1 is innervated by the medial branches above and below. These medial branches send off articular branches to the facet joints as they wrap around the waists of the articular pillars.
Intervertebral discs are located between each vertebral body caudad to the axis. The discs are composed of 4 parts, including the nucleus pulposus in the middle, the annulus fibrosis surrounding the nucleus, and 2 end plates that are attached to the adjacent vertebral bodies. The discs are involved in cervical spine motion, stability, and weight bearing. The annular fibers are composed of collagenous sheets called lamellae, which are oriented 65-70° from the vertical and alternate in direction with each successive sheet. Therefore, the annular fibers are prone to injury with rotation forces because only one half of the lamellae are oriented to withstand the force in this direction. [25] The middle and outer one third of the annulus is innervated by nociceptors, and phospholipase A2 has been found in the disc and may be an inflammatory mediator. [29, 30, 31]
Several ligaments of the cervical spine, which provide stability and proprioceptive feedback, are worth mentioning. [32, 33] The transverse ligament, the major portion of the cruciate ligament, arises from tubercles on the atlas and stretches across its anterior ring while holding the dens against the anterior arch. A synovial cavity is located between the dens and the transverse process. This ligament allows for rotation of the atlas on the dens and is responsible for stabilizing the cervical spine during flexion, extension, and lateral bending. The transverse ligament is the most important ligament in preventing abnormal anterior translation. [34]
The alar ligaments run from the lateral aspects of the dens to the ipsilateral medial occipital condyles and to the ipsilateral atlas. The alar ligaments limit axial rotation and side bending. If the alar ligaments are damaged, as in a whiplash injury, the joint complex becomes hypermobile, which can lead to kinking of the vertebral arteries and stimulation of the nociceptors and mechanoreceptors. This may be associated with the typical complaints of patients with whiplash injuries such as headache, neck pain, and dizziness. The alar ligaments prevent excessive lateral and rotational motions, while allowing flexion and extension.
The anterior longitudinal ligament (ALL) and the posterior longitudinal ligament (PLL) are the major stabilizers of the intervertebral joints. Both ligaments are found throughout the entire length of the spine; however, the anterior longitudinal ligament is closely adhered to the discs in comparison to the posterior longitudinal ligament, and it is not well developed in the cervical spine. The anterior longitudinal ligament becomes the anterior atlantooccipital membrane at the level of the atlas, whereas the posterior longitudinal ligament merges with the tectorial membrane. Both ligaments continue onto the occiput. The posterior longitudinal ligament prevents excessive flexion and distraction. [35]
The supraspinous ligament, interspinous ligament, and ligamentum flavum maintain stability between the vertebral arches. The supraspinous ligament runs along the tips of the spinous processes, the interspinous ligament runs between the spinous processes, and the ligamentum flavum runs from the anterior surface of the cephalad vertebra to the posterior surface of the caudad vertebra. The interspinous ligament and especially the ligamentum flavum control for excessive flexion and anterior translation. [35, 36, 37] The ligamentum flavum also connects to and reinforces the facet joint capsules on the ventral aspect. The ligamentum nuchae is the cephalad continuation of the supraspinous ligament and has a prominent role in stabilizing the cervical spine.
Sport Specific Biomechanics
The patterns of motion of C2–C7 are determined by the orientation of the facet joints, the intervertebral discs, and the uncovertebral joints. The orientation of the facet joints lead to coupling of rotation and lateral flexion. For example, as the vertebral bodies laterally flex to the left, they also rotate to the left (the spinous processes move to the right). The degree of rotation that is coupled with lateral flexion decreases in the more caudal motion segments, possibly due to the difference in facet orientation in the caudal segments, which may contribute to unilateral facet joint dislocations in the lower cervical spine. [38]
The height of the articular process increases with caudal progression, which determines the quality of flexion and extension and allows more gliding motion in the cephalad segments. [39] Horizontal translation of a vertebral body more than 3.5 mm as measured on a lateral radiograph during flexion and extension is considered to be the upper limit of normal motion. [40]
The orientation of the facet joints alone does not determine the pattern of motion. In the lumbar spine, the pattern of motion does not change after the facets are removed, which implies that the discs and ligaments determine the pattern of motion. [41] Also, because of the orientation of the annular fibers in the disc, there is very little rotation in the lumbar spine. [42] However, it is known that there is a great deal of rotation in the cervical spine. Therefore, the discs do not seem to be the primary determinant of motion in the cervical spine.
The joints of Luschka are suggested to be involved primarily in rotation and may aid in the coupling of rotation and lateral flexion. [43] Another purpose of the joints of Luschka may be to protect the disc from injury as it ages and loses its water content. This may explain why these joints are not present at birth but develop later in childhood. [44]
The orientation of the OA joints allow for substantial flexion and extension (13°), less lateral flexion (8°) and rotation (10°), and minimal translation (1 mm). [45, 46] The AA joints allow for axial rotation of 65°, which is 40-50% of the total cervical spine rotation, negligible lateral flexion, 10° of flexion and extension, and lateral translation of 4 mm. [45, 47] This degree of axial rotation can cause kinking of the vertebral arteries that run in the transverse foramina of C6 to the atlas. The contralateral artery begins to kink at 30° and the ipsilateral artery at 45°. [48] Consequences include nausea, vomiting, visual problems, vertigo, and stroke. [49]
With axial rotation of the atlas on the axis, there is a coupled movement of vertical translation of the atlas, so that it is at its lowest position at the extremes of right and left rotation and at its highest position at neutral. This coupling of translation with rotation is secondary to the orientation of the facets. [5] The instantaneous axis of rotation (IAR) is a term used to describe the motion of one vertebral body in relation to the vertebral body below.
The IAR has been estimated at the OA joint, [47] the AA joint, [45] and in the cervical spine from C2-C3 to C6-C7. [50] In the middle and lower cervical spine, the IAR has been measured for each segment from C2-C3 to C6-C7 in asymptomatic people. [51] In a subsequent study, the IARs were measured in persons with neck pain, who had not received a diagnosis after examination and imaging of the cervical spine. [50] Abnormal IARs were found in 46% of the patients, and an additional 26% had marginal findings. However, the location of the abnormal motion segments did not correlate with the findings on discography or facet joint blocks.
-
Cervical vertebra.
-
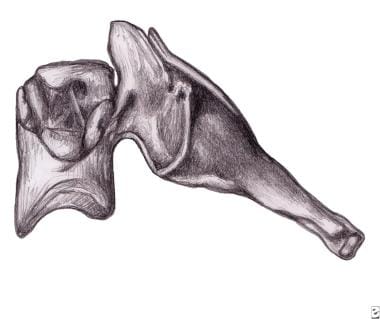
Unilateral facet dislocation.
-
Bilateral facet dislocation.
-
Cervical facet syndrome.
-
A composite drawing of the referral patterns of 9 subjects derived from the minimal threshold stimulation of their right occipital nerve and C3-C8 medial branches


