Practice Essentials
Thoracic outlet syndrome is not the name of a single entity but rather a collective title for a variety of conditions attributed to the compression of neurovascular structures as they traverse the thoracic outlet. [1, 2, 3, 4, 5, 6] The thoracic outlet is bordered by the scalene muscles, first rib, and clavicle. Neurovascular structures pass from the neck and thorax into the axilla through this space. Thoracic outlet syndrome remains one of the most controversial clinical entities in medicine. [7, 8, 9] See the image below.
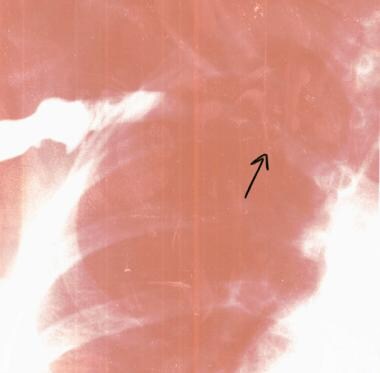 Thoracic outlet syndrome in a 16-year-old volleyball player with a stenotic right subclavian vein (arrow) secondary to fibrosis.
Thoracic outlet syndrome in a 16-year-old volleyball player with a stenotic right subclavian vein (arrow) secondary to fibrosis.
Diagnosis and management
To exclude systemic disease and inflammation, a few simple blood tests may refine the differential diagnosis for thoracic outlet syndrome, including a blood glucose level, complete blood cell (CBC) count, erythrocyte sedimentation rate (ESR), basic metabolic panel, thyrotropin level, and rheumatologic workup, if indicated.
Imaging studies that can be used in the diagnosis of thoracic outlet syndrome include the following:
-
Radiography
-
Computed tomography (CT) scanning and magnetic resonance imaging (MRI) - Useful for identifying other conditions that might cause similar symptoms
-
Magnetic resonance angiography (MRA)
-
Venography and duplex scanning
Electrodiagnostic studies can be helpful in classic cases of neurogenic thoracic outlet syndrome. However, many symptoms are intermittent in this disorder; therefore, negative test results do not rule out the diagnosis.
Surgery in cases of thoracic outlet syndrome is indicated for acute vascular insufficiency and progressive neurologic dysfunction. Other patients should receive nonoperative treatment that, in the acute phase, includes relative rest, nonsteroidal anti-inflammatory medications (NSAIDs), cervicoscapular strengthening exercises, and modalities such as ultrasound, transcutaneous nerve stimulation, and biofeedback. Physiotherapy in the acute phase focuses on pain control and range of motion with specific stretching exercises.
Etiology
Causes of thoracic outlet syndrome can be divided into bony and soft-tissue factors. Bony factors include abnormalities such as anomalous cervical ribs, hypoplastic first thoracic ribs, and exostoses of the first rib or clavicle. [10, 11] The rate of anomalous cervical ribs is considered to be 0.17-0.74% in the general population, and the rate of rudimentary first ribs is 0.29-0.76%. [12]
Soft-tissue factors include congenital anomalies such as anomalous fibrous muscular bands near the brachial plexus and hypertrophic muscles in athletes and weight lifters. [11, 13] Space-occupying lesions (eg, tumors, cysts) and inflammatory processes also occur in the soft tissues and can cause thoracic outlet syndrome.
Trauma or mechanical stress to the neck, shoulders, or upper extremities can lead to thoracic outlet syndrome. In fact, a combination of neck trauma and anatomic predisposition (ie, cervical rib) is considered the main etiology of thoracic outlet syndrome. [14] Posttraumatic conditions such as hematoma, myositis ossificans, and scar formation can be important variables, as can a droopy shoulder secondary to trapezius muscle weakness. [15] Thoracic outlet syndrome can be secondary to malunion of a clavicle fracture. [16]
Interestingly, multiple points of compression may be present as the peripheral nerves descend from the thoracic outlet to the hand (simultaneous thoracic outlet syndrome and ulnar nerve compression at the elbow or carpal tunnel syndrome in the wrist). This has been referred to as double- [17] or multiple-crush syndrome. [18]
Epidemiology
United States statistics
The wide variability of symptoms and signs in patients with thoracic outlet syndrome and the lack of an objective confirmatory test for the diagnosis makes correctly identifying patients with thoracic outlet syndrome difficult. [19] Therefore, determining its exact incidence remains elusive; estimates range from 3-80 cases per 1000 population. [20]
Sex- and age-related demographics
Thoracic outlet syndrome is more common in women, particularly those with poor muscular development, poor posture, or both. [21]
The onset of symptoms typically occurs in persons aged 20-50 years. Although thoracic outlet syndrome is uncommon in children, cases have been reported in adolescents. [22]
Functional Anatomy
The neurovascular bundle courses through 3 spaces, or triangles, as it exits the neck to reach the axilla and proximal arm. All 3 spaces can be the source of compression of the various components of the neurovascular bundle, including the brachial plexus and the subclavian vessels. [23] These spaces are small at rest and become even smaller with certain arm maneuvers, such as abduction and external rotation. [24, 25] This can aid in the diagnosis of thoracic outlet syndrome and forms the basis for provocative testing, which is discussed later (see Clinical, Physical).
The first space is the interscalene triangle. It is bordered by the anterior scalene muscle, the middle scalene muscle, and the upper border of the first rib. This space contains the trunks of the brachial plexus and subclavian artery. The interscalene triangle is the most common site for neural compression, vascular compression, or both. [20]
The second space is the costoclavicular triangle, which is bordered by the clavicle, first rib, and scapula and contains the subclavian artery and vein and the brachial nerves.
The third and final space is beneath the coracoid process just deep to the pectoralis minor tendon; it is referred to as the subcoracoid space.
Sport-Specific Biomechanics
Thoracic outlet syndrome is most often seen in patients who engage in repetitive motions that place the shoulder at the extreme of abduction and external rotation. An example of such activity is swimming, especially with the freestyle stroke, butterfly stroke, and backstroke. When a swimmer reports tightness and pain around the shoulder, neck, and clavicle as his or her hand enters the water, thoracic outlet syndrome should be suspected.
In addition to swimmers, other athletes affected by thoracic outlet syndrome include water polo, baseball, and tennis players and athletes in any other activity that places repetitive stress on the shoulder at the extremes of abduction and external rotation. These individuals may present with neurologic and arterial or venous symptoms. Venous thoracic outlet syndrome most commonly develops in young male athletes in whom the upper extremity musculature is overdeveloped as a result of work or physical conditioning. Baseball players, whose sport requires repetitive throwing motions, are at increased risk for arterial thoracic outlet syndrome in their dominant arm.
Prognosis
Symptoms resolve with conservative therapy in approximately 90% of individuals. Postsurgical success rates over 1 year vary from 43-78%. A good surgical result means improvement, not total cure. Most patients are able to return to their previous lifestyle without difficulty. Job modification is required in individuals who perform repetitive activities, work on assembly lines, perform heavy laboring, or work with their arms elevated.
A systematic review by Garraud et al found that the prognosis for thoracic outlet syndrome in athletes appeared to be generally better than the prognosis in the general population, possibly because of better physical condition and younger age. [26]
Complications
Ischemic changes, including gangrene, are potential complications of arterial thoracic outlet syndrome. Pulmonary embolism is reported in 0-28.5% of patients with subclavian-axillary venous thrombosis. Venous gangrene and upper extremity phlegmasia cerulea dolens account for 2-5% of all cases of phlegmasia. Nerve injury (eg, brachial plexus neurapraxia) is the most serious postoperative complication after thoracic outlet decompression. Bleeding problems from the subclavian vessels and lymph leakage from the thoracic duct occur infrequently.
Patient Education
Inform patients that symptoms recur in 15-20% of patients. [27] The initial treatment is conservative in nature and includes a search for other diagnoses (see Differentials and Other Problems to Be Considered). Chronic pain may improve with the continued use of analgesics and a routine exercise and strengthening program.
-
Thoracic outlet syndrome in a 16-year-old volleyball player with a stenotic right subclavian vein (arrow) secondary to fibrosis.







