Practice Essentials
Bicipital tendinitis, or biceps tendinitis, is an inflammatory process of the long head of the biceps tendon and is a common cause of shoulder pain due to its position and function. [1, 2, 3, 4] The tendon is exposed on the anterior shoulder as it passes through the humeral bicipital groove and inserts onto the superior aspect of the labrum of the glenohumeral joint. (See the image below.) Disorders of the biceps tendon can result from impingement or as an isolated inflammatory injury. Other causes are secondary to compensation for rotator cuff disorders, labral tears, and intra-articular pathology.
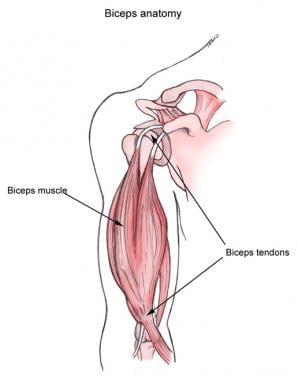 Biceps muscle and tendons.
Biceps muscle and tendons.
Signs and symptoms
Patients typically report achy anterior shoulder pain, which is exacerbated by lifting or elevated pushing or pulling. A frequent complaint is pain with overhead activity or with lifting heavy objects.
See Presentation for more detail.
Diagnosis
Standard shoulder radiographs are generally not helpful or necessary in cases of isolated bicipital tendinitis.
Magnetic resonance imaging (MRI) can demonstrate the entire course of the long head of the biceps tendon. However, this imaging study is expensive and not cost-effective as a routine test.
Arthroscopy may be useful in evaluating chronic shoulder pain. This procedure is sensitive for detecting and differentiating subtle defects in the shoulder, including lesions in the superior labral complex and the articular surface of the humeral head.
See Workup for more detail.
Management
The initial goals of the acute phase of treatment for bicipital tendinitis are to reduce inflammation and swelling.
Physical therapy and rehabilitation are directed toward restoring the integrity and strength of the dynamic and static stabilizers of the shoulder joint while restoring the affected shoulder's range of motion, which is critical for most athletes.
Surgical treatment is indicated only after a 6-month trial of conservative care is unsuccessful.
See Treatment and Medication for more detail.
Patient education
Inform the patient that an increased risk of biceps tendon rupture or chronic inflammatory changes exists if the directed restrictions are not followed.
Etiology
The long head of the biceps tendon passes down the bicipital groove in a fibrous sheath between the subscapularis and supraspinatus tendons. This relationship causes the biceps tendon to undergo degenerative and attritional changes that are associated with rotator cuff disease because the biceps tendon shares the associated inflammatory process within the suprahumeral joint. [5]
Full humeral head abduction places the attachment area of the rotator cuff and biceps tendon under the acromion. External rotation of the humerus at or above the horizontal level compresses these suprahumeral structures into the anterior acromion. Repeated irritation leads to inflammation, edema, microscopic tearing, and degenerative changes.
In younger athletes, relative instability due to hyperlaxity may cause similar inflammatory changes on the biceps tendon due to excessive motion of the humeral head.
Labral tears may disrupt the biceps anchor, resulting in dysfunction and causing pain.
The transverse humeral ligament holds the biceps tendon long head within the bicipital groove. Injuries and disruption of the ligament can lead to subluxation and medial dislocation of the biceps tendon. Local edema and calcifications can physically displace the biceps tendon from the bicipital groove, resulting in subluxation. An osteochondroma in the bicipital groove has been reported as a cause of bicipital tendinitis in a baseball player by physical displacement and subluxation. [6]
A study evaluated the histologic findings of the extra-articular portion of the long head of the biceps (LHB) tendon and synovial sheath in order to compare those findings to known histologic changes seen in other tendinopathies. The study concluded that anterior shoulder pain attributed to the biceps tendon does not appear to be due to an inflammatory process in most cases. The histologic findings of the extra-articular portion of the LHB tendon and synovial sheath are similar to the pathologic findings in de Quervain tenosynovitis at the wrist, and may be due to a chronic degenerative process similar to this and other tendinopathies of the body. [7]
Epidemiology
United States statistics
Bicipital tendinitis is frequently diagnosed in association with rotator cuff disease as a component of the impingement syndrome or secondary to intra-articular pathology, such as labral tears. [8]
Functional Anatomy
As its name implies, the biceps has 2 proximal heads with a common distal insertion onto the radius. The long head of the biceps merges with the short head of the biceps to form the body of the biceps brachii muscle. This muscle is a powerful supinator and flexor of the forearm.
The long head biceps tendon lies in the bicipital groove of the humerus between the greater and lesser tuberosities and angles 90° inward at the upper end of the groove, crossing the humeral head to insert at the upper edge of the glenoid labrum and supraglenoid tubercle. The long head of the biceps tendon helps to stabilize the humeral head, especially during abduction and external rotation.
See the image below.
Biceps muscle and tendons.
Sport-Specific Biomechanics
Bicipital tendinitis frequently occurs from overuse syndromes of the shoulder, [9] which are fairly common in overhead athletes such as baseball pitchers, swimmers, gymnasts, racquet sport enthusiasts (eg, tennis players), and rowing/kayak athletes. [10, 11, 12, 13] A systematic review by Stamm et al found that overuse injuries are common among softball players and that the windmill pitch puts significant stress on the biceps tendon. [14]
In overhead athletes, trauma may occur because of direct injury to the biceps tendon when the arm is passed into excessive abduction and external rotation. This pattern of shoulder injury can also occur in the left shoulder of right-handed golfers. Many overuse injuries coexist with some degree of bicipital tendinitis and rotator cuff tendinitis.
The athletic shoulder differs qualitatively from the biomechanics of the shoulder in daily life because of the higher energies and repetitive motions that are involved in athletic activities. Sports activities that require repetitive overhead motion with inadequate reparative time may cause the biceps tendon to break down.
Prognosis
Although the prognosis of bicipital tendinitis is dependent upon the degree of injury, most patients do well with treatment (see Treatment: Acute Phase, Recovery Phase, Maintenance Phase, and Surgical Intervention). However, a significant number of patients develop degenerative changes, and spontaneous rupture of the biceps tendon occurs in 10% of patients.
Complications
Individuals who return to a high level of athletic activity too soon may find themselves with symptom flare-ups. Continued straining of an injury that has not healed completely can put the individual at risk for chronic degenerative tissue damage and biceps tendon rupture.
-
Biceps muscle and tendons.



