Practice Essentials
Meniscal injuries may be the most common knee injury. Meniscal tears are sometimes related to trauma, but significant trauma is not necessary. A sudden twist or repeated squatting can tear the meniscus.
Understanding of the importance of the menisci in the biomechanics of the knee has progressed steadily since 1968, when Jackson wrote, "The exact function of that structure (meniscus) is still a matter of some conjecture." [1] At that time, it was common to remove the entire substance if any doubt existed regarding the integrity of the meniscus. Today, it is known that the menisci are not optional or expendable structures; they have an integral role in normal knee joint mechanics. (See images below.)

The classification of meniscal tears provides a description of pathoanatomy. Such tears include the following:
-
Longitudinal tears that may take the shape of a bucket handle if displaced
-
Radial tears
-
Parrot-beak, or oblique flap, tears
-
Horizontal tears
-
Root tears
-
Complex tears that combine variants of the above
Signs and symptoms of meniscal injury
In meniscal injury, acute joint-line pain may be described. Joint effusion gradually develops over a few hours. Patients with peripheral tears of the meniscus occasionally develop effusion rapidly (in minutes), secondary to a tear that is associated with hemarthrosis and is in the vascular outer one third of the meniscus.
Locking is a common symptom after a meniscal lesion develops, usually occurring at 20-45° of joint extension.
A sensation of giving way may occur. In true meniscal lesions, the fragment becomes lodged momentarily in the knee joint, causing a sense of buckling.
Workup in meniscal injury
Arthroscopy of the knee is the criterion standard for the diagnosis of a meniscal tear.
Magnetic resonance imaging (MRI) is the criterion standard for imaging studies of meniscal pathology and all intra-articular disorders. [2, 3] MRI is not routinely required for the diagnosis of meniscal tears before proceeding with arthroscopic surgery; however, it helps to confirm the diagnosis and provides additional information concerning the status of the ligaments and articular cartilage. [4]
Arthrocentesis can be used as a diagnostic tool and a therapeutic procedure.
Management
Physical therapy
The three main issues considered in the rehabilitation of meniscal repairs are knee motion, weight bearing, and return to sports. [5]
The goals of the physical therapy program are to minimize effusion, normalize gait, normalize pain-free range of motion (ROM), prevent muscular atrophy, maintain proprioception, and maintain cardiovascular fitness.
The protocols for rehabilitation of a meniscal injury take into consideration biomechanical principles and the results of the physical examination. Factors such as the extent and location of the lesion, the amount of articular cartilage degeneration on weight-bearing surfaces, the duration of injury, and joint stability affect the pace and aggressiveness of the rehabilitation program.
The program for rehabilitation following meniscal repair is similar in principle to the program that follows meniscectomy; however, more limitations are put on the patient's weight-bearing status, and the duration of each phase of rehabilitation is longer to allow for healing.
The program for nonoperative rehabilitation is also similar in principle to the program that follows meniscectomy. Cryotherapy and nonsteroidal anti-inflammatory drugs (NSAIDs) play a very important role in the management of nonoperative meniscal injury.
Surgery
If conservative treatment does not lead to resolution, surgical treatment is considered. Surgical options (arthroscopic or open) include the following:
-
Partial meniscectomy - The treatment of choice for tears in the avascular portion of the meniscus or complex tears that are not amenable to repair
-
Meniscal repair - Recommended for tears that occur in the vascular region (red zone or red-white zone, as described below), are longer than 1 cm, are root tears, involve greater than 50% of the meniscal thickness, and are unstable to arthroscopic probing
-
In cases of previous total or subtotal meniscectomy, meniscus transplantation - A relatively new procedure for which specific indications and long-term results have not yet been clearly established
Background
The meniscus has unique anatomic properties. An understanding of its anatomy is essential to comprehending the important functions of the meniscus, which include load bearing, load and force distribution, joint stability, joint lubrication, and proprioception. [6, 7, 8] One of the primary functions is to provide load bearing across the knee joint. Fifty percent of the compressive load in the knee is transferred by the menisci in extension, whereas up to 85% of the load is transferred at 90° of flexion.
Load and forces are distributed across a much larger surface area because of the menisci, which (1) decrease focal contact pressure by increasing the contact area and (2) protect the underlying articular cartilage. Resection of 15-34% of a meniscus may increase contact pressure by more than 350%. Normal knees have 20% better shock-absorbing capacity than meniscectomized knees.
Joint stability is increased because of meniscal structure, which allows increased congruence and conformity between the femoral condyles and tibial plateaus. [6, 7] The wedge-shaped meniscus attached to the tibia serves as a secondary stabilizer. For example, the posterior horn acts as a shim to resist anterior tibial translation relative to the femur. Meniscectomy alone may not increase knee laxity, but it has been shown that in association with anterior cruciate ligament (ACL) deficiency, greater anterior laxity results. Meniscal lubrication occurs from fluid exudation across the surface, much like with articular cartilage.
Pathophysiology
Anatomy
The menisci are C-shaped wedges of fibrocartilage located between the tibial plateau and the femoral condyles. The larger, semilunar medial meniscus is attached more firmly than the loosely fixed, more circular lateral meniscus. [9] The anterior and posterior horns of both menisci are secured to the tibial plateaus. Anteriorly, the transverse ligament connects the two menisci; posteriorly, the meniscofemoral ligament helps to stabilize the posterior horn of the lateral meniscus to the femoral condyle. The coronary ligaments connect the peripheral meniscal rim loosely to the tibia. Although the lateral collateral ligament (LCL) passes in close proximity, the lateral meniscus has no attachment to this structure.
The joint capsule attaches to the entire periphery of each meniscus but adheres more firmly to the medial meniscus. An interruption in the attachment of the joint capsule to the lateral meniscus, forming the popliteal hiatus, allows the popliteus tendon to pass through to its femoral attachment site. Contraction by the popliteus during knee flexion pulls the lateral meniscus posteriorly, avoiding entrapment within the joint space. The medial meniscus does not have a direct muscular connection. The medial meniscus may shift a few millimeters, while the less stable lateral meniscus may move at least 1 cm.
The microanatomy of the meniscus is dense fibrocartilage composed of cells and an extracellular matrix of collagen fibers in network. The cells are termed fibrochondrocytes because they appear to be a mixture of fibroblasts and chondrocytes. These cells are responsible for the synthesis and maintenance of the extracellular fibrocartilaginous matrix.
The most abundant component of the menisci is collagen (75%)—mainly type I collagen (>90%), although they also contain types II, III, V, and VI. Collagen fibers are arranged mostly along a longitudinal or circumferential direction, with some interwoven radial and oblique fibers. The circumferential fibers are related directly to the menisci's functional ability to dissipate compressive loads. The other fibers act primarily as ties to enhance structural rigidity and to help prevent longitudinal splitting. The extracellular matrix also includes proteoglycans, glycoproteins, and elastin.
When a compressive force is applied in the knee joint, a tensile force is transmitted to the menisci. The femur attempts to spread the menisci anteroposteriorly in extension and mediolaterally in flexion. Shrive et al studied the effects of a radial cut in the peripheral rim of the menisci during loading. In joints with intact menisci, the force was applied through the menisci and articular cartilage; however, a lesion in the peripheral rim disrupted the normal mechanics of the menisci and allowed spreading when a load was applied. The load now was distributed directly to the articular cartilage. In light of these findings, it is essential to preserve the peripheral rim during partial meniscectomy to avoid irreversible disruption of the structure's hoop tension capability. [10]
Blood supply
The blood supply to the menisci is limited to their peripheries. The medial and lateral geniculate arteries anastomose into a parameniscal capillary plexus supplying the synovial and capsular tissues of the knee joint. The vascular penetration through this capsular attachment is limited to 10-25% of the peripheral widths of the medial and lateral meniscal rims. In 1990, Renstrom and Johnson reported a 20% decrease in the vascular supply by age 40 years, which may be attributed to weight bearing over time. [11]
The potential for vascular ingrowth is essential for successful meniscal healing and surgical repair. Various zones of the meniscus are described based on the blood supply; the red zone is the well-vascularized periphery, the red-white zone is the middle portion with vascularity peripherally but not centrally, and the white zone is the central avascular portion. Arnoczky, in 1982, proposed a classification system that categorizes lesions in relation to the meniscal vascular supply, as follows [12] :
-
An injury resulting in a lesion within the blood-rich periphery is called a red-red tear; both sides of the tear are in tissue with a functional blood supply, a situation that promotes healing
-
A tear encompassing the peripheral rim and central portion is called a red-white tear; in this situation, one end of the lesion is in tissue with a good blood supply, while the opposite end is in the avascular section
-
A white-white tear is a lesion located exclusively in the avascular central portion; the prognosis for healing in such a tear is unfavorable
Reports describe techniques for manufacturing a vascular access channel from the peripheral vasculature to improve the chance that tissue in the central region will repair itself.
Neuroanatomy
The neuroanatomy of the meniscus is not well described. However, the distribution of neural elements has been demonstrated in essentially the same anatomic distribution as the vascular supply. The anterior and posterior horns are the most richly innervated, and the body innervation follows the pattern along the periphery. Although not entirely clear, these nerve endings are believed to play a role in sensory feedback and proprioception. The greater innervation of the horns of the meniscus reflects the need for feedback at the extremes of flexion and extension, when the meniscal horns are compressed and neural elements are activated. [6, 7, 13]
Biomechanics
The menisci follow the motion of the femoral condyle during knee flexion and extension. Shrive et al presented a model of normal meniscal function. [10] During extension, the femoral condyles exert a compressive force that displaces the menisci anteroposteriorly. As the knee moves into flexion, the condyles roll backward onto the tibial plateau. The menisci deform mediolaterally, maintaining joint congruity and maximal contact area. As the knee flexes, the femur externally rotates on the tibia, and the medial meniscus is pulled forward. Studies by Shrive, Fukubayashi, Walker, and Kurosawa state that the menisci directly influence the transmission of forces, distribution of load, amount of contact force, and pressure distribution patterns.
Mechanism of injury
Meniscal injuries, particularly sports-related injuries, usually involve damage due to rotational force. A common mechanism of injury is a varus or valgus force directed to a flexed knee. When the foot is planted and the femur is internally rotated, a valgus force applied to a flexed knee may cause tearing of the medial meniscus. A varus force on a flexed knee with the femur externally rotated may lead to a lateral meniscus lesion. According to Ricklin, the medial meniscus is attached more firmly than the relatively mobile lateral meniscus, and this may result in a greater incidence of medial meniscus injury. [9]
Epidemiology
Frequency
United States
Although the exact incidence and prevalence of meniscal injury are unknown, it is a fairly common sports-related injury among adults. Knee meniscal injuries also occur in individuals who are skeletally immature, but less commonly than in adults. Meniscal injuries are rare in children younger than 10 years with morphologically normal menisci. [14]
Mortality/Morbidity
Meniscal injuries usually are associated with pain that results in gait deviation and loss of time from work and/or sport.
A study by Yasuda et al suggested that medial meniscus tears cause spontaneous osteonecrosis of the knee (SONK). Specifically, the investigators found medial meniscal extrusion and the femorotibial angle to be significantly associated with SONK stage and volume in the medial femoral condyle. [15]
Race
A correlation between race and meniscal injuries is not known to exist.
Sex
Meniscal injuries are more common in males, which may be a reflection of greater involvement by males in aggressive sporting and manual activities that predispose to rotational injuries of the knee.
Age
Meniscal injuries are common in young males who are involved in sporting or manual activities. A second peak of incidence is observed in persons older than 55 years; this is secondary to a degenerate meniscus being susceptible to injuries with minor trauma. [16] As previously stated, meniscal injuries are rare in children younger than 10 years with morphologically normal menisci. [14]
-
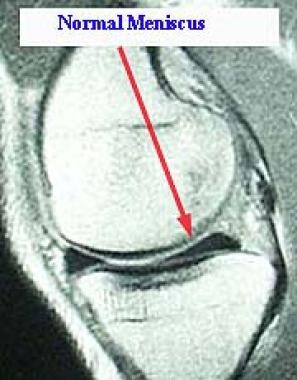
Magnetic resonance imaging scan showing a normal meniscus.
-
Magnetic resonance imaging scan showing a torn medial meniscus.
-
Arthroscopic probing of a posterior horn complex meniscal tear with multiple flaps.
-
Arthroscopic view of medial meniscus after excision of flap tear.






