Practice Essentials
The brain is an organ of immense complexity. In the cranium, dural reflections and bony landmarks divide the brain into anatomic regions. Brain herniation represents mechanical displacement of normal brain relative to another anatomic region secondary to mass effect from traumatic, neoplastic, ischemic, or infectious etiologies. Brain herniation is classified as intracranial or extracranial. An intracranial hernia can be subfalcine, transtentorial (ascending or descending), or tonsillar. Brain herniation can result in brain damage, compression of cranial nerves and vessels (causing hemorrhage or ischemia), or obstruction of the normal CSF circulation, producing hydrocephalus. [1, 2, 3] CT is the preferred imaging modality for brain herniation because of the short acquisition time, the cost, and the wide availability. Prompt diagnsosis is essential because patients with brain herniation are generally in critical condition. [4, 5, 2, 6]
(See the images below.)
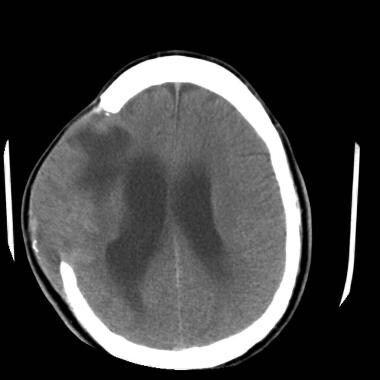
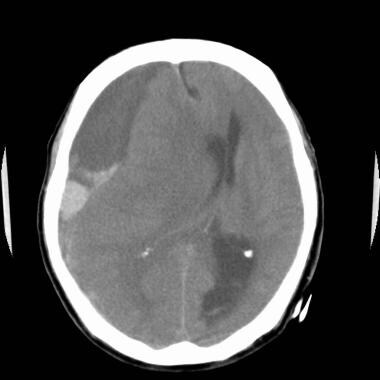 Nonenhanced head computed tomography (CT) scan at the level of the lateral ventricles was obtained in a 78-year-old man who presented with respiratory failure. The image demonstrates a large right frontal and temporal subdural fluid collection with hyperattenuating and hypoattenuating components consistent with an acute on chronic subdural hematoma. Subfalcine herniation, midline shift, effacement of the ipsilateral lateral ventricle, and enlargement of the contralateral occipital horn are present.
Nonenhanced head computed tomography (CT) scan at the level of the lateral ventricles was obtained in a 78-year-old man who presented with respiratory failure. The image demonstrates a large right frontal and temporal subdural fluid collection with hyperattenuating and hypoattenuating components consistent with an acute on chronic subdural hematoma. Subfalcine herniation, midline shift, effacement of the ipsilateral lateral ventricle, and enlargement of the contralateral occipital horn are present.
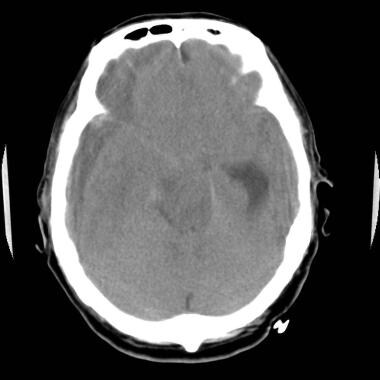 Nonenhanced head computed tomography scan at the level of the suprasellar cistern in the same patient as in the previous image. A large right frontotemporal subdural hematoma is exerting mass effect on the right frontal and temporal lobes, with resultant effacement of the suprasellar cistern and with right-sided uncal herniation. Mass effect from the subdural hematoma effaces the ipsilateral temporal horn, causing dilatation of the contralateral temporal horn. Subfalcine herniation and narrowing of the contralateral ambient and quadrigeminal plate cisterns are present.
Nonenhanced head computed tomography scan at the level of the suprasellar cistern in the same patient as in the previous image. A large right frontotemporal subdural hematoma is exerting mass effect on the right frontal and temporal lobes, with resultant effacement of the suprasellar cistern and with right-sided uncal herniation. Mass effect from the subdural hematoma effaces the ipsilateral temporal horn, causing dilatation of the contralateral temporal horn. Subfalcine herniation and narrowing of the contralateral ambient and quadrigeminal plate cisterns are present.
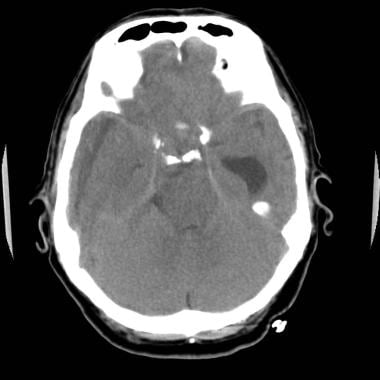 Nonenhanced head computed tomography (CT) scan obtained at the level of the inferior pons in the same patient as in the previous 2 images. Acute-on-chronic right temporal subdural hematoma exerts mass effect on the right temporal lobe, causing ipsilateral temporal horn, with effacement and dilatation of the contralateral temporal horn. Narrowing of the contralateral ambient and quadrigeminal plate cisterns is present, with ipsilateral widening of the ambient and quadrigeminal cisterns.
Nonenhanced head computed tomography (CT) scan obtained at the level of the inferior pons in the same patient as in the previous 2 images. Acute-on-chronic right temporal subdural hematoma exerts mass effect on the right temporal lobe, causing ipsilateral temporal horn, with effacement and dilatation of the contralateral temporal horn. Narrowing of the contralateral ambient and quadrigeminal plate cisterns is present, with ipsilateral widening of the ambient and quadrigeminal cisterns.
Herniations of the brain are divided into 5 major categories, as follows:
-
Transtentorial herniation [7]
-
Subfalcine/cingulate herniation
-
Foramen magnum/tonsillar herniation (seen in patients with Arnold-Chiari malformation, as demonstrated in the images below) [8, 9, 10, 11]
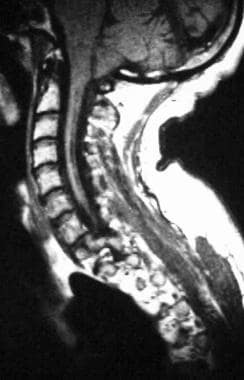 T1-weighted sagittal magnetic resonance image through the cervical spine in a child with a history of an Arnold-Chiari I malformation. Image shows tonsillar herniation with compression of the central canal at the craniocervical junction and resultant syringohydromyelia in the visualized portion of the cervical spinal cord.
T1-weighted sagittal magnetic resonance image through the cervical spine in a child with a history of an Arnold-Chiari I malformation. Image shows tonsillar herniation with compression of the central canal at the craniocervical junction and resultant syringohydromyelia in the visualized portion of the cervical spinal cord.
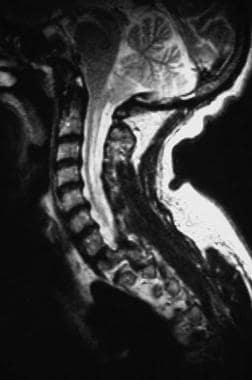 T2-weighted sagittal magnetic resonance image through the cervical spine was obtained in the same patient as in the previous image. The cerebellar tonsils are projecting inferiorly below the level of the opisthion, with compression of the central canal at the craniocervical junction. Hyperintense syringohydromyelia in the visualized portion of the cervical spinal cord is demonstrated.
T2-weighted sagittal magnetic resonance image through the cervical spine was obtained in the same patient as in the previous image. The cerebellar tonsils are projecting inferiorly below the level of the opisthion, with compression of the central canal at the craniocervical junction. Hyperintense syringohydromyelia in the visualized portion of the cervical spinal cord is demonstrated.
-
Sphenoid/alar herniation
-
Extracranial herniation
Each category of herniation is associated with a specific neurologic syndrome.
Preferred examination
Sustained intracranial hypertension and acute brain herniation are “brain codes,” signifying catastrophic neurologic events that require immediate recognition and treatment to prevent irreversible injury and death. In the emergent setting of a brain code, a cranial computed tomography (CT) scan should be obtained to identify a process that may require surgical intervention. Cranial CT is preferred over magnetic resonance imaging (MRI) because of the availability and speed of CT. In the majority of cases, CT will identify the underlying process, although MRI may subsequently be needed for characterization. MRI should only be sought if the imminent risk of an additional brain code has been addressed by medical and/or surgical intervention. [1, 4, 12, 13, 5, 2, 6]
For transtentorial herniation, CT scanning or MRI is useful for evaluation. MRI can provide axial, as well as sagittal and coronal, views.
For subfalcine/cingulate herniation, CT scanning or MRI is again useful for evaluation, with MRI able to provide axial, sagittal, and coronal views.
For foramen magnum/tonsillar herniation, MRI provides the best visualization on sagittal and coronal views. However, because patients with this type of herniation often present acutely, axial CT scanning enables visualization of this condition.
For sphenoid/alar herniation, MRI provides the best visualization on parasagittal images. However, axial CT scanning or MRI can demonstrate anterior displacement of the ipsilateral middle cerebral artery, which is an indirect sign of sphenoid herniation. [14, 15]
For extracranial herniation, CT scanning or MRI is useful for evaluation.
A study by Probst et al found that among 161 patients with frank brain herniation diagnosed by CT scan, 3 (1.9%) had no neurologic deficit. The investigators also found that of 91 patients with significant brain shift but no herniation, 4 (4.4%) had no neurologic deficit. ICT scans were classified into 3 categories: frank herniation, significant shift without frank herniation, and minimal or no shift. [16]
Vascular displacement from mass effect associated with herniation can be seen on cerebral angiograms. Specifically, deep venous anatomic distortion aids in identifying these entities, although CT scanning and MRI are the currently favored diagnostic modalities. The degree of confidence is high when classic displacement of the deep venous structures is seen.
Guidelines
The American College of Radiology (ACR) Appropriateness Criteria for acute mental status change, delirium, and new onset psychosis includes the following recommendations for initial imaging [4] :
-
For the initial imaging of acute mental status changes associated with clinical suspicion for intracranial infection, mass, or elevated intracranial pressure, a noncontrast head CT is usually the initial test of choice. MRI is complementary to CT, but may also be used as a first-line test based on clinical judgement.
-
For the initial imaging of an acute or progressively worsening mental status change in a patient with a known intracranial process (mass, recent hemorrhage, recent infarct, central nervous system infection, etc), CT head without IV contrast, MRI head without and with IV contrast, or MRI head without IV contrast are equivalent alternatives, and the choice of imaging will be based on clinical judgement.
Computed Tomography
CT is the preferred imaging modality for brain herniation because of the short acquisition time, the cost, and the wide availability. Prompt diagnosis is essential because patients with brain herniation are generally in critical condition. [4, 5, 2, 6] Cross-sectional imaging provides a high degree of confidence.
With a descending transtentorial herniation, mass effect in the cerebrum pushes the supratentorial brain through the incisura. [17] With ascending transtentorial herniation, mass effect from the posterior fossa pushes the infratentorial brain through the incisura. This results in the distortion of the midbrain, flattening of the posterior quadrigeminal plate, and narrowing of the bilateral ambient cisterns. Hydrocephalus is frequently noted. [1, 4, 12, 13, 5, 2, 6]
With subfalcine/cingulate herniation (seen below), the supratentorial brain is displaced underneath the anterior falx.
Nonenhanced head computed tomography (CT) scan at the level of the lateral ventricles was obtained in a 78-year-old man who presented with respiratory failure. The image demonstrates a large right frontal and temporal subdural fluid collection with hyperattenuating and hypoattenuating components consistent with an acute on chronic subdural hematoma. Subfalcine herniation, midline shift, effacement of the ipsilateral lateral ventricle, and enlargement of the contralateral occipital horn are present.
Nonenhanced head computed tomography scan at the level of the suprasellar cistern in the same patient as in the previous image. A large right frontotemporal subdural hematoma is exerting mass effect on the right frontal and temporal lobes, with resultant effacement of the suprasellar cistern and with right-sided uncal herniation. Mass effect from the subdural hematoma effaces the ipsilateral temporal horn, causing dilatation of the contralateral temporal horn. Subfalcine herniation and narrowing of the contralateral ambient and quadrigeminal plate cisterns are present.
Nonenhanced head computed tomography (CT) scan obtained at the level of the inferior pons in the same patient as in the previous 2 images. Acute-on-chronic right temporal subdural hematoma exerts mass effect on the right temporal lobe, causing ipsilateral temporal horn, with effacement and dilatation of the contralateral temporal horn. Narrowing of the contralateral ambient and quadrigeminal plate cisterns is present, with ipsilateral widening of the ambient and quadrigeminal cisterns.
With foramen magnum/tonsillar herniation, the infratentorial brain is displaced through the foramen magnum.
With sphenoid/alar herniations, the supratentorial brain is sliding anteriorly or posteriorly over the wing of the sphenoid bone. An anterior herniation occurs when the temporal lobe herniates anteriorly and superiorly over the sphenoid bone. Conversely, a posterior herniation occurs when the frontal lobe herniates posteriorly and inferiorly over the sphenoid bone.
With extracranial herniation, the brain is displaced through a cranial defect, as in the image below.
 Nonenhanced computed tomography (CT) scan of the brain at the level of the body of the lateral ventricles was obtained in a 37-year-old man who underwent a right frontotemporal decompression craniectomy for a large right frontal hematoma after a skiing accident. A focal hypoattenuating infarct is seen in the right frontal lobe, with an adjacent edematous brain parenchyma herniating through the right frontotemporal craniectomy defect. The patient had communicating hydrocephalus with dilatation of the lateral ventricles.
Nonenhanced computed tomography (CT) scan of the brain at the level of the body of the lateral ventricles was obtained in a 37-year-old man who underwent a right frontotemporal decompression craniectomy for a large right frontal hematoma after a skiing accident. A focal hypoattenuating infarct is seen in the right frontal lobe, with an adjacent edematous brain parenchyma herniating through the right frontotemporal craniectomy defect. The patient had communicating hydrocephalus with dilatation of the lateral ventricles.
Magnetic Resonance Imaging
Although CT is the mainstay of imaging for acute traumatic brain injury, MRI is more sensitive for the detection of certain intracranial injuries (eg, axonal injuries) and blood products 24-48 hours after injury. However, MRI does have limitations in terms of speed, accessibility, sensitivity to motion, and cost. Evidence primarily supports the use of MRI when CT findings are normal or when there are persistent and unexplained neurologic findings. [10, 4, 13, 5]
With descending transtentorial herniation, mass effect in the cerebrum pushes the supratentorial brain through the incisura. In ascending transtentorial herniation (seen in the images below), mass effect from the posterior fossa pushes the infratentorial brain through the incisura. This results in the distortion of the midbrain, flattening of the posterior quadrigeminal plate, and narrowing of the bilateral ambient cisterns. Hydrocephalus is frequently noted. [1, 4, 18, 12, 13, 5, 2, 6]
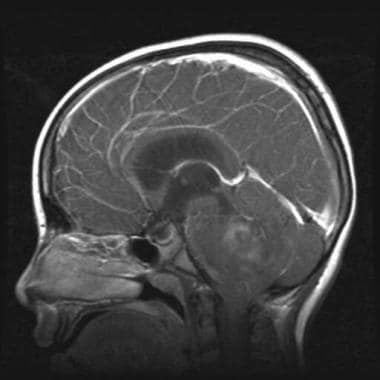 Right parasagittal gadolinium-enhanced T1-weighted magnetic resonance image in a 9-year-old girl with a history of right cerebellar astrocytoma who presented with headaches and vomiting. Heterogeneously enhancing mass is demonstrated in the right cerebellum, with compression of the adjacent brainstem and fourth ventricle. Ascending transtentorial herniation of the cerebellum is demonstrated through the incisura. Descending tonsillar herniation also is present.
Right parasagittal gadolinium-enhanced T1-weighted magnetic resonance image in a 9-year-old girl with a history of right cerebellar astrocytoma who presented with headaches and vomiting. Heterogeneously enhancing mass is demonstrated in the right cerebellum, with compression of the adjacent brainstem and fourth ventricle. Ascending transtentorial herniation of the cerebellum is demonstrated through the incisura. Descending tonsillar herniation also is present.
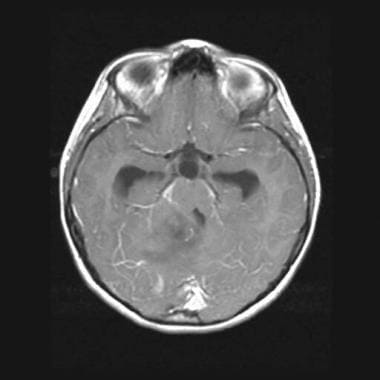 Axial gadolinium-enhanced T1-weighted magnetic resonance image obtained at the level of the midbrain in the same patient as in the previous image. A heterogeneously enhancing mass is seen in the right medial anterior cerebellum, with mass effect on the right posterior lateral midbrain and fourth ventricle. The image shows enlargement of the temporal horns of both lateral ventricles as a result of obstruction by the cerebellar mass at the level of the fourth ventricle.
Axial gadolinium-enhanced T1-weighted magnetic resonance image obtained at the level of the midbrain in the same patient as in the previous image. A heterogeneously enhancing mass is seen in the right medial anterior cerebellum, with mass effect on the right posterior lateral midbrain and fourth ventricle. The image shows enlargement of the temporal horns of both lateral ventricles as a result of obstruction by the cerebellar mass at the level of the fourth ventricle.
Subfalcine/cingulate herniation causes the supratentorial brain to be displaced underneath the anterior falx.
In foramen magnum/tonsillar herniation, the infratentorial brain is displaced through the foramen magnum (see the images below).
 T1-weighted sagittal magnetic resonance image through the cervical spine in a child with a history of an Arnold-Chiari I malformation. Image shows tonsillar herniation with compression of the central canal at the craniocervical junction and resultant syringohydromyelia in the visualized portion of the cervical spinal cord.
T1-weighted sagittal magnetic resonance image through the cervical spine in a child with a history of an Arnold-Chiari I malformation. Image shows tonsillar herniation with compression of the central canal at the craniocervical junction and resultant syringohydromyelia in the visualized portion of the cervical spinal cord.
 T2-weighted sagittal magnetic resonance image through the cervical spine was obtained in the same patient as in the previous image. The cerebellar tonsils are projecting inferiorly below the level of the opisthion, with compression of the central canal at the craniocervical junction. Hyperintense syringohydromyelia in the visualized portion of the cervical spinal cord is demonstrated.
T2-weighted sagittal magnetic resonance image through the cervical spine was obtained in the same patient as in the previous image. The cerebellar tonsils are projecting inferiorly below the level of the opisthion, with compression of the central canal at the craniocervical junction. Hyperintense syringohydromyelia in the visualized portion of the cervical spinal cord is demonstrated.
With sphenoid/alar herniations, the supratentorial brain slides either anteriorly or posteriorly over the wing of the sphenoid bone. An anterior herniation occurs when the temporal lobe herniates anteriorly and superiorly over the sphenoid bone. Conversely, a posterior herniation occurs when the frontal lobe herniates posteriorly and inferiorly over the sphenoid bone.
Extracranial herniation causes the brain to be displaced through a cranial defect.
Gadolinium-based contrast agents have been linked to the development of nephrogenic systemic fibrosis (NSF) or nephrogenic fibrosing dermopathy (NFD). The disease has occurred in patients with moderate to end-stage renal disease after being given a gadolinium-based contrast agent to enhance MRI or magnetic resonance angiography (MRA) scans.
Cross-sectional imaging provides a high degree of confidence.
-
Nonenhanced head computed tomography (CT) scan at the level of the lateral ventricles was obtained in a 78-year-old man who presented with respiratory failure. The image demonstrates a large right frontal and temporal subdural fluid collection with hyperattenuating and hypoattenuating components consistent with an acute on chronic subdural hematoma. Subfalcine herniation, midline shift, effacement of the ipsilateral lateral ventricle, and enlargement of the contralateral occipital horn are present.
-
Nonenhanced head computed tomography scan at the level of the suprasellar cistern in the same patient as in the previous image. A large right frontotemporal subdural hematoma is exerting mass effect on the right frontal and temporal lobes, with resultant effacement of the suprasellar cistern and with right-sided uncal herniation. Mass effect from the subdural hematoma effaces the ipsilateral temporal horn, causing dilatation of the contralateral temporal horn. Subfalcine herniation and narrowing of the contralateral ambient and quadrigeminal plate cisterns are present.
-
Nonenhanced head computed tomography (CT) scan obtained at the level of the inferior pons in the same patient as in the previous 2 images. Acute-on-chronic right temporal subdural hematoma exerts mass effect on the right temporal lobe, causing ipsilateral temporal horn, with effacement and dilatation of the contralateral temporal horn. Narrowing of the contralateral ambient and quadrigeminal plate cisterns is present, with ipsilateral widening of the ambient and quadrigeminal cisterns.
-
Right parasagittal gadolinium-enhanced T1-weighted magnetic resonance image in a 9-year-old girl with a history of right cerebellar astrocytoma who presented with headaches and vomiting. Heterogeneously enhancing mass is demonstrated in the right cerebellum, with compression of the adjacent brainstem and fourth ventricle. Ascending transtentorial herniation of the cerebellum is demonstrated through the incisura. Descending tonsillar herniation also is present.
-
Axial gadolinium-enhanced T1-weighted magnetic resonance image obtained at the level of the midbrain in the same patient as in the previous image. A heterogeneously enhancing mass is seen in the right medial anterior cerebellum, with mass effect on the right posterior lateral midbrain and fourth ventricle. The image shows enlargement of the temporal horns of both lateral ventricles as a result of obstruction by the cerebellar mass at the level of the fourth ventricle.
-
Nonenhanced computed tomography (CT) scan of the brain at the level of the body of the lateral ventricles was obtained in a 37-year-old man who underwent a right frontotemporal decompression craniectomy for a large right frontal hematoma after a skiing accident. A focal hypoattenuating infarct is seen in the right frontal lobe, with an adjacent edematous brain parenchyma herniating through the right frontotemporal craniectomy defect. The patient had communicating hydrocephalus with dilatation of the lateral ventricles.
-
T1-weighted sagittal magnetic resonance image through the cervical spine in a child with a history of an Arnold-Chiari I malformation. Image shows tonsillar herniation with compression of the central canal at the craniocervical junction and resultant syringohydromyelia in the visualized portion of the cervical spinal cord.
-
T2-weighted sagittal magnetic resonance image through the cervical spine was obtained in the same patient as in the previous image. The cerebellar tonsils are projecting inferiorly below the level of the opisthion, with compression of the central canal at the craniocervical junction. Hyperintense syringohydromyelia in the visualized portion of the cervical spinal cord is demonstrated.




