Practice Essentials
Morton neuroma, or interdigital neuroma, is a common condition that involves enlargement of the interdigital nerve of the foot. Morton neuroma most commonly affects the third intermetatarsal space, but it can also affect the second intermetatarsal space, although it does so less often. Lesions in the fourth and first interspaces are unusual. The name is derived from Thomas Morton, who first described interdigital nerve compression in 1876 and concluded that the nerve was being compressed between the metatarsal heads. Morton neuroma is not a true neuroma, but it does cause neuropathic pain in the interdigital nerve caused by chronic irritation. [1, 2, 3]
Preferred examination
Although a Morton neuroma can often be confidently diagnosed on the basis of the clinical findings alone, imaging is useful in the preoperative setting or in cases with atypical symptoms. [4] Morton neuromas have been imaged successfully using MRI, CT scanning, and ultrasonography. [5, 6] MRI has been the preferred imaging modality for demonstrating Morton neuroma largely because of MRI's superior contrast resolution and reproducibility. [7, 8, 9, 10, 11, 12, 13, 14, 15]
Neuromas are a common ailment seen by foot and ankle specialists. The diagnosis is often straightforward because of the description of a sharp, shooting pain or numbness in the affected digits. However, because the patients' descriptions of the pain can vary or because the pain can be related to another ailment in the differential diagnosis, MRI has become a useful imaging tool in obtaining a precise diagnosis. Ultrasonography also is commonly used. It is more widely available and less costly than MRI. Despite these advantages, the operator-intensive aspects of sonography, as well as its steep learning curve, are limiting factors. In a study of 37 patients with confirmed Morton neuroma, MRI sensitivity was 82.9% [95% confidence interval (CI): 0.679-0.929] and US sensitivity was 56.5% (95% CI: 0.345-0.768). [16]
(See the images of Morton Neuroma below.)
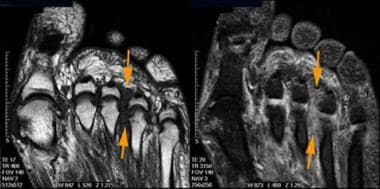 Morton neuroma. Longitudinal T1-weighted (left) and short-tau inversion recovery (right) magnetic resonance images reveal a low–signal-intensity mass between the third and fourth metatarsal heads. Note how the mass is inconspicuous on the latter image.
Morton neuroma. Longitudinal T1-weighted (left) and short-tau inversion recovery (right) magnetic resonance images reveal a low–signal-intensity mass between the third and fourth metatarsal heads. Note how the mass is inconspicuous on the latter image.
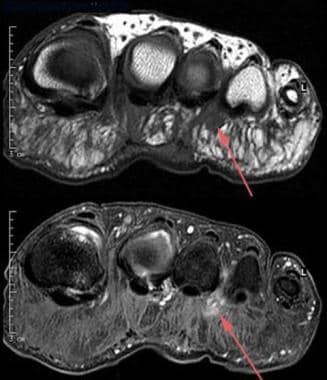 Morton neuroma. Transverse T1-weighted (top) and contrast-enhanced fat-suppressed T1-weighted (bottom) MRIs show the bulbous morphology of the perineural mass with plantar extension. The administration of contrast material reveals enhancement of the lesion.
Morton neuroma. Transverse T1-weighted (top) and contrast-enhanced fat-suppressed T1-weighted (bottom) MRIs show the bulbous morphology of the perineural mass with plantar extension. The administration of contrast material reveals enhancement of the lesion.
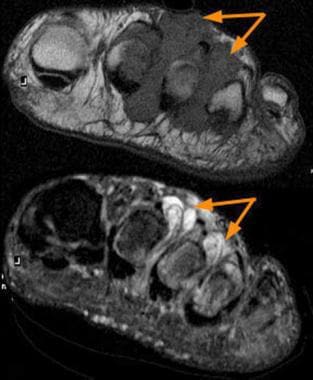 Rheumatoid nodules. T1-weighted (top) and short-tau inversion recovery (bottom) MRIs reveal large masses at the second and third interspaces. The latter image shows high signal intensity, which is not a feature of Morton neuromas. The patient had known rheumatoid arthritis, and the signal-intensity characteristics of these lesions are consistent with the proliferative synovium seen in this condition.
Rheumatoid nodules. T1-weighted (top) and short-tau inversion recovery (bottom) MRIs reveal large masses at the second and third interspaces. The latter image shows high signal intensity, which is not a feature of Morton neuromas. The patient had known rheumatoid arthritis, and the signal-intensity characteristics of these lesions are consistent with the proliferative synovium seen in this condition.
Differential diagnosis
The differential diagnosis of Morton neuroma includes stress fracture, tendon sheath ganglion, foreign-body reaction, nerve-sheath tumor, strain of the plantar capsule, and capsulitis or bursitis at the level of the plantar metatarsal-phalangeal joint (MPJ). [4, 5] Occasionally, the diagnosis can be challenging because, in addition to inflammation of the capsule or bursa, inflammation of the adjacent nerve also may be present, causing the neuritic sensation of a Morton neuroma.
Peripheral neuropathy also can cause symptoms such as a burning or neuritic sensation, but these tend to occur throughout the toes and on both feet. Additional differential diagnoses with similar symptoms involve neoplasms and fibromas. Imaging studies, particularly MRIs, are a valuable tool in differentiating these conditions.
MRI
Not uncommonly, Morton neuromas are incidental findings on MRIs; they are detected best on short-axis (transverse) T1-weighted MRIs through the metatarsal heads. Morton neuroma is typically seen as a bulbous mass arising between the metatarsal heads. Because neuromas have a highly cellular and/or fibrous nature, lesions demonstrate low signal intensity on both T1- and T2-weighted images (see the images below). The lesions are highly vascular and are typically enhancing after the intravenous administration of a gadolinium-based contrast agent. [17] Contrast enhancement is best visualized on T1-weighted fat-saturated images. [4, 7]
Morton neuroma. Longitudinal T1-weighted (left) and short-tau inversion recovery (right) magnetic resonance images reveal a low–signal-intensity mass between the third and fourth metatarsal heads. Note how the mass is inconspicuous on the latter image.
Morton neuroma. Transverse T1-weighted (top) and contrast-enhanced fat-suppressed T1-weighted (bottom) MRIs show the bulbous morphology of the perineural mass with plantar extension. The administration of contrast material reveals enhancement of the lesion.
Rheumatoid nodules. T1-weighted (top) and short-tau inversion recovery (bottom) MRIs reveal large masses at the second and third interspaces. The latter image shows high signal intensity, which is not a feature of Morton neuromas. The patient had known rheumatoid arthritis, and the signal-intensity characteristics of these lesions are consistent with the proliferative synovium seen in this condition.
Reliably differentiating Morton neuroma from a normal plantar nerve is difficult unless the lesion is 5 mm or larger. [18] An intermetatarsal space lesion that is bright on T2-weighted images is unlikely to represent a Morton neuroma. Lesions with hyperintense signal on T2-weighted images are more likely to represent a true neuroma, a synovial or rheumatoid nodule, or bursal fluid. The administration of contrast material assists in differentiating these entities because true neuromas are intensely enhancing, and bursal fluid is not enhancing. [17]
MRI findings in a suggested Morton neuroma effectively influence therapy. In one study, imaging findings changed the treatment plan in 57% of patients, with the withdrawal of the diagnosis in 28% and with changes in the location or number of detected neuromas in more than 33% of the feet of the remaining patients. [18] Interspace lesions with low intensity appear on imaging studies in asymptomatic patients. [4] Therefore, careful correlation with the clinical findings is essential prior to initiating therapy.
Gadolinium-based contrast agents have been linked to the development of nephrogenic systemic fibrosis or nephrogenic fibrosing dermopathy (NSF/NFD). For more information, see the eMedicine topic Nephrogenic Fibrosing Dermopathy. NSF/NFD has occurred in patients with moderate to end-stage renal disease after being given a gadolinium-based contrast agent to enhance MRI or magnetic resonance angiography scans. NSF/NFD is a debilitating and sometimes fatal disease. Characteristics include red or dark patches on the skin; burning, itching, swelling, hardening, and tightening of the skin; yellow spots on the whites of the eyes; joint stiffness with trouble moving or straightening the arms, hands, legs, or feet; pain deep in the hip bones or ribs; and muscle weakness. For more information, see the FDA Public Health Advisory or Medscape.
Ultrasonography
Ultrasonography has the advantage of being less expensive and more portable than MRI, but it has a high learning curve and dependence on the operator's skill. Relatively few radiologists and technologists in the United States are experienced in using ultrasonography to diagnose Morton neuroma. [19, 20, 21, 22, 23] In one study, Morton neuroma was confirmed on ultrasonography at the site of clinical diagnosis in 98% of patients (53 out of 54 feet). [24]
Ultrasound-guided procedures for Morton neuroma have been extensively studied and shown to be effective, such as ultrasound-guided administration of corticosteroids, pulsed radio frequency, and alcohol injection. US has also been shown in some studies to be equivalent to MRI in making the diagnosis of Morton neuroma. [24, 25, 26, 27, 28, 29, 30, 31, 32] Ultrasound-guided steroid injections in Morton neuroma have been found to provide short-term pain relief to over 60% of the patients in one study. [26]
A systematic review of 12 studies with 217 patients who underwent MRI and 241 who underwent ultrasound examinations found equivalent or better diagnostic accuracy for ultrasound than MRI for the diagnosis of Morton's neuroma (ultrasound sensitivity 90%, specificity 88%, positive likelihood ratio 2.77, negative likelihood ratio 0.16; versus MRI sensitivity 93%, specificity 68%, positive likelihood ratio 1.89, negative likelihood ratio 0.19). [12]
In a study by Bignotti et al, ultrasonography and MRI were identified as being equally accurate in diagnosing Morton neuroma, with sensitivities of 0.91 and 0.90, respectively. [3]
-
Morton neuroma. Longitudinal T1-weighted (left) and short-tau inversion recovery (right) magnetic resonance images reveal a low–signal-intensity mass between the third and fourth metatarsal heads. Note how the mass is inconspicuous on the latter image.
-
Morton neuroma. Transverse T1-weighted (top) and contrast-enhanced fat-suppressed T1-weighted (bottom) MRIs show the bulbous morphology of the perineural mass with plantar extension. The administration of contrast material reveals enhancement of the lesion.
-
Rheumatoid nodules. T1-weighted (top) and short-tau inversion recovery (bottom) MRIs reveal large masses at the second and third interspaces. The latter image shows high signal intensity, which is not a feature of Morton neuromas. The patient had known rheumatoid arthritis, and the signal-intensity characteristics of these lesions are consistent with the proliferative synovium seen in this condition.


