Practice Essentials
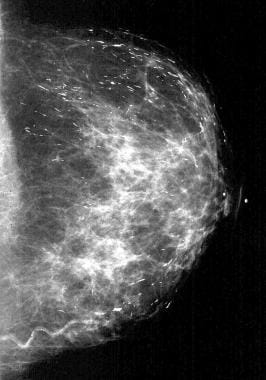
Breast calcifications are a common mammographic finding, present on over 80% of images, and they are usually benign. Characteristics such as size, shape, number, distribution pattern, location, density, and other findings help determine pathology. [1, 2] Radiologists who interpret mammograms encounter calcifications on a daily basis (see the images below) and must be able to identify typically benign breast calcifications that do not require biopsy to prevent unnecessary procedures and to reduce patient anxiety. [3, 4, 5, 6, 7, 8] Typically, benign calcifications that do not require biopsy are skin or dermal, vascular, lucent-centered, eggshell or rim, coarse or popcornlike, large rodlike, round and punctuate, milk of calcium, suture, and dystrophic. [9, 10]
Preferred examination
High-quality mammography is the best diagnostic tool for the identification of breast calcifications. Accredited, dedicated mammographic equipment should be used to obtain high-quality images. Mammography technologists must be well trained and skilled in the proper positioning and compression of the breast. [11, 12, 13, 14, 15, 16]
Mammograms should always be interpreted on dedicated high-luminance mammographic view boxes or viewers, and a magnifying glass should be used routinely. Extraneous light and glare should be eliminated for optimal viewing conditions. Mammograms should be arranged in the same manner at each interpretation session to minimize left-right confusion.
Routine mammograms should include craniocaudal (CC) and mediolateral oblique (MLO) views. That is, the 2 mammographic views usually obtained first for screening or diagnostic evaluations are the MLO view and the CC view. Magnification images of calcifications should be obtained in the CC and mediolateral (ML) or lateromedial (LM) views, also known as true lateral views. Tangential views are useful for verification of the intradermal location of calcifications. [17]
Comparing current mammograms with prior mammograms is essential to determine the stability of any calcifications detected. Finally, on the basis of the interpretation, the radiologist can make an informed decision about whether the calcifications identified are benign and do not require biopsy or whether the appearance of the calcifications warrants biopsy.
In a retrospective study of 2359 calcifications for which a stereotactic biopsy was performed, calcifications associated with ductal carcinoma in situ (DCIS) were larger than those associated with benign breast disease at biopsy (median, 10 mm vs 6 mm, respectively; P< .001). The researchers concluded that the rate of calcification change may help discriminate benign from malignant calcifications. The relative annual increase in the long-axis length of DCIS calcifications was greater than that of benign breast calcifications (96% [95% confidence interval: 72%, 224%] vs 68% [95% confidence interval: 56%, 80%] per year, respectively; P< .001). [18]
Limitations of techniques
Mammography is limited in evaluating benign calcifications when benign calcifications morphologically overlap with indeterminate or malignant calcifications. These calcifications may be observed for a short period (ACR BI-RADS category 3; see below), or biopsy may be performed (ACR BI-RADS categories 4 and 5; see below).
Although screening mammography remains the only modality demonstrated to reduce death from breast cancer, 70–80% of biopsies performed for suspicious mammographic findings (masses and calcifications) are benign. These shortcomings have led to studies of other imaging modalities with the goal of improving the current benchmarks of mammography.
In a study comparing conspicuity of DCIS to benign calcifications on unenhanced breast CT (bCT), contrast-enhanced breast CT (CEbCT), and mammography, DCIS was found to be more conspicuous than benign microcalcifications on CEbCT. DCIS visualization on CEbCT is equal to that on mammography but better than that on bCT. Radiologists’ discrimination performance using CEbCT is significantly higher than enhancement values alone. CEbCT may have an advantage over mammography by reducing false positive examinations when calcifications are analyzed. [19, 20]
Distribution of breast calcifications
Breast calcifications are described in terms of type and distribution and categorized according to the Breast Imaging Reporting and Data System (BI-RADS) of the American College of Radiology (ACR). [21, 22, 23, 24, 25, 26]
Distribution modifiers (grouped or clustered, linear, segmental, regional, diffuse) are used to describe the arrangement of the calcifications. Historically, the terms grouped or clustered were used to describe suspicious calcification. Now, these terms are neutral and may be used to describe benign or malignant processes. Grouped or clustered should be used to describe calcifications that occupy a small volume (< 2 µL) of tissue. [27]
Calcifications that are linearly distributed are arranged in a line and may have branch points.
Segmentally distributed calcifications suggest deposition of calcification in a duct and its branches. This type of calcification may be secondary to benign or malignant processes.
Regionally distributed calcifications are most likely due to benign processes. These calcifications are scattered in a large volume of the breast and do not necessarily conform to a ductal distribution.
Diffusely distributed calcifications are scattered randomly throughout the breast.
ACR BI-RADS lexicon for mammographic findings
The ACR BI-RADS lexicon enables radiologists to use similar terminology to describe mammography findings. This lexicon facilitates data tracking and provides clear management and follow-up recommendations to referring physicians, allied healthcare providers, and patients.
There are 7 ACR BI-RADS standardized categories [22, 23, 28, 29] :
-
Category 0, or "need additional imaging evaluation," is used if additional imaging is needed (this category is almost always used in a screening situation and should be used only rarely after a full imaging workup; additional imaging evaluation includes the use of spot compression and magnification views, along with other tailored mammographic views and ultrasonography)
-
Category 1, or "negative," is used if there are no findings to comment on; for example, the breasts are symmetrical, and no masses, architectural disturbances, or suspicious calcifications are present
-
Category 2, or "benign finding(s)," is used if the radiologist wishes to describe a benign finding while still concluding that there is no mammographic evidence of malignancy
-
Category 3, or "probably benign finding–initial short-interval follow-up suggested," is used when a noted finding has a very high probability of being benign; the finding is not expected to change over the follow-up interval, but the radiologist prefers to establish its stability over time
-
Category 4, or "suspicious abnormality–biopsy should be considered," is used when a finding has a definite probability of being malignant
-
Category 5, or "highly suggestive of malignancy–appropriate action should be taken," is used when a finding has a high probability of being cancerous
-
Category 6, or "known biopsy-proven malignancy-appropriate action should be taken," is "reserved for lesions identified on imaging study with biopsy proof of malignancy prior to definitive therapy"
Typically, benign calcifications will be placed in ACR BI-RADS categories 1 and 2. Sometimes, these calcifications are initially placed in ACR BI-RADS category 0 and, after additional imaging evaluation, are found to have benign features. Early in their development, calcifications (eg, vascular, dystrophic, or lucent centered calcifications) may be indeterminate; these are often followed at short intervals to establish or confirm their etiology (ie, BI-RADS category 3).
Mammogram
Skin or dermal calcifications
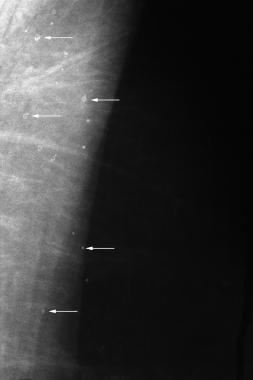
Skin or dermal calcifications (see the image below) are usually identified as spherical, lucent-centered calcifications at the periphery of the breast, especially in the inferior, posterior, and medial aspects. [30, 31] Skin calcifications may develop from a degenerative metaplastic process. Usually, skin calcifications are readily distinguished as benign findings. However, in some cases, additional imaging is needed to differentiate skin calcifications from more worrisome calcifications.
When mammograms are compared, calcifications that maintain a fixed relationship to one another are suggestive of a dermal location. Magnification views may be used to demonstrate the lucent centers characteristic of skin calcifications. In some cases, a skin localization procedure may be needed to prove that the calcifications are in the skin.
When performing a skin localization procedure, the radiologist should determine if the calcifications are more likely to be in the upper or the lower portion of the breast. Thereafter, the patient's breast is placed in the mammographic unit by using a fenestrated compression device. For calcifications presumed to be in the upper part of the breast, a CC approach is used with the fenestration device in the region of the calcifications. For calcifications thought to be in the inferior part of the breast, a caudocranial approach is used. A metal marker is then placed over the calcifications, and a tangential view is obtained to show the dermal calcifications in the skin.
Vascular calcifications
Vascular calcifications (shown below) are commonly identified on mammography, especially in older women. Vascular calcifications, which are usually secondary to medial atherosclerosis, often demonstrate a characteristic train tracklike configuration. In some cases, it may be difficult to distinguish vascular calcifications from ductal calcifications (including calcifications representing ductal carcinoma in situ). Arterial calcification in the breasts may be associated with diabetes and hyperparathyroidism.
The presence of mammary vascular calcifications may allow for the detection of women with elevated cardiovascular disease risk profiles. [32, 33, 34, 35] Researchers in the Netherlands examined 12,239 women in a population-based breast cancer screening program. The study showed a significant correlation between vascular calcifications identified on mammography and myocardial infarction, transient ischemic attacks, and hypertension. Additional studies are needed to validate the potential role for screening mammography in the early detection of women at risk for cardiovascular disease.
In a systematic review and meta-analysis, breast arterial calcifications (BAC) were found in 12.7% of women in breast cancer screening programs. Increasing age, diabetes, and parity (as opposed to nulliparity) were associated with a higher prevalence of BAC. The authors concluded that medial arterial calcification might contribute to cardiovascular disease through a pathway distinct from the intimal atherosclerotic process. [36]
Screening mammograpms in women with a history of warfarin use found that the prevalence of breast arterial calcification is increased in women with current or past warfarin use independent of other risk factors and conditions predating warfarin use. According to the study, this effect appears to be cumulative and may be irreversible. The increased prevalence varied depending on duration of treatment, from 25% for use less than one year to 74.4% for use more than 5 years. [37]
Lucent-centered calcifications
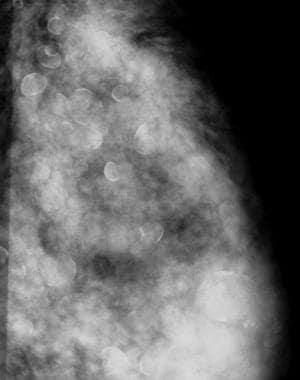
Lucent-centered calcifications, as depicted below, which are round or oval, are almost always benign, and they have thicker walls than those of rim or eggshell calcifications. Skin calcifications are often lucent-centered, and lucent-centered calcifications may form around benign debris in the ducts. Other entities that may appear as lucent-centered calcifications on mammography include silicone granulomas and fat necrosis.
 This patient was in a car accident and sustained a seatbelt injury. The lucent-centered calcifications seen are typical of fat necrosis.
This patient was in a car accident and sustained a seatbelt injury. The lucent-centered calcifications seen are typical of fat necrosis.
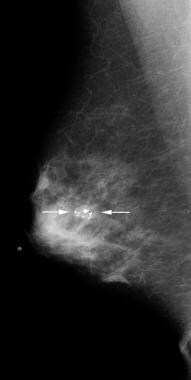
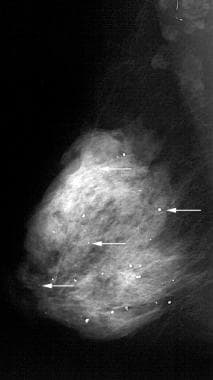
 This patient underwent breast-conserving surgery. The lucent-centered calcifications (arrow) are typical of fat necrosis.
This patient underwent breast-conserving surgery. The lucent-centered calcifications (arrow) are typical of fat necrosis.
Fat necrosis results from several causes including trauma, surgery, and radiation therapy. Fat necrosis occurs most often in fatty pendulous breasts of middle-aged women. Lucent-centered calcifications may result from fat necrosis, and the thickness of the calcified wall around the lucent area is variable and probably related to the amount of desmoplastic reaction.
Eggshell or rim calcifications
Eggshell or rim calcifications, shown below, are thin and appear as calcium deposited on the surface of a sphere. The walls of eggshell or rim calcifications are thinner than the walls of lucent-centered calcifications.
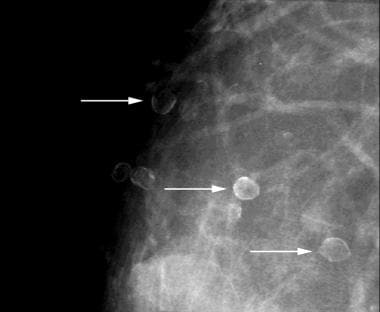 Eggshell or rim calcifications (arrows) have walls thinner than those of lucent-centered calcifications.
Eggshell or rim calcifications (arrows) have walls thinner than those of lucent-centered calcifications.
The entire circumference of an eggshell calcification does not need to be completely calcified to represent a benign finding. Although fat necrosis can result in eggshell calcifications, calcification in the walls of cysts is the most common cause of eggshell or rim calcifications.
Coarse or popcornlike calcifications
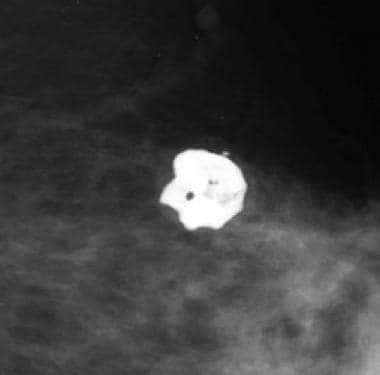
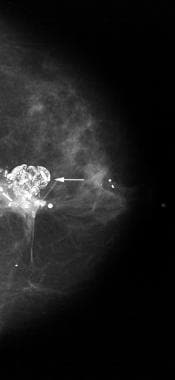
Coarse or popcornlike calcifications, as shown below, are associated with the involution and hyaline degeneration of fibroadenomas. Fibroadenomas are the most common breast masses seen in women younger than 35 years.
 This mass with associated large, coarse calcifications (arrows) is a degenerating fibroadenoma.
This mass with associated large, coarse calcifications (arrows) is a degenerating fibroadenoma.
 Calcifications associated with fibroadenomas have been termed popcorn calcifications because of their large size and dense, coarse appearance.
Calcifications associated with fibroadenomas have been termed popcorn calcifications because of their large size and dense, coarse appearance.
Calcifications in fibroadenomas usually begin at the periphery and then involve the central portion of the fibroadenoma. Fibroadenomas may be completely replaced by calcification without a mass discernible by mammography.
Large rodlike or secretory calcifications
Large rodlike or secretory calcifications (see below) are oriented along the axes of the ductal system. [38] These calcifications result from calcification of ductal secretions.
 Large rodlike or secretory calcifications are oriented along the axis of the breast ductal system.
Large rodlike or secretory calcifications are oriented along the axis of the breast ductal system.
Large rodlike calcifications may have lucent centers if the ductal secretions undergo peripheral calcification. In general, these calcifications are coarser and larger (usually >1 mm in diameter) than malignant calcifications. Large rodlike calcifications are commonly bilateral and diffuse. These calcifications are associated with secretory disease, plasma cell mastitis, and duct ectasia. [38]
In a study of 7935 women who underwent screeining or diagnostic mammography, 239 (3%) were found to have large rodlike calcifications. The mean length of the longest calcification was 4.2 mm (median, 3.5 mm; range, 1-14 mm), and the mean width of the widest calcification was 0.6 mm (median, 0.5 mm; range 0.2-3 mm). [38]
Round and punctate calcifications
Punctate calcifications, as shown in the image below, are spherical calcifications that have well-defined margins.
Punctate calcifications usually measure less than 0.5 mm in diameter. Round calcifications are benign spherical calcifications that may vary in size. When less than 1 mm, round calcifications are frequently formed in the acini of the lobules.
Milk of calcium
Milk of calcium (see below) is a benign process that can be diagnosed readily during mammography, especially with magnification views in the CC and the true lateral (ML or LM) projections. [39]
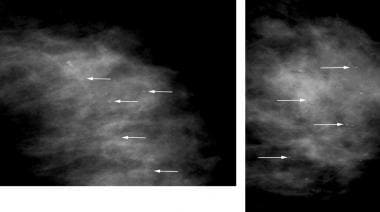 Left, On the craniocaudal (CC) magnification view, milk of calcium appears poorly defined and smudgy (arrows). Right, On the mediolateral (ML) or the lateromedial (LM) magnification view, milk of calcium is seen as sharply defined, crescent-shaped, semilunar, curvilinear (concave up), or linear arrangements (arrows).
Left, On the craniocaudal (CC) magnification view, milk of calcium appears poorly defined and smudgy (arrows). Right, On the mediolateral (ML) or the lateromedial (LM) magnification view, milk of calcium is seen as sharply defined, crescent-shaped, semilunar, curvilinear (concave up), or linear arrangements (arrows).
When milk of calcium is imaged with a vertical x-ray beam on the CC view, the calcifications appear poorly defined and smudgy. When imaged with a horizontal x-ray beam on the ML or the LM view, the calcifications are seen as sharply defined, crescent-shaped, semilunar, curvilinear (concave up), or linear arrangements. The characteristic appearance of the calcifications on the magnification views helps to establish the correct diagnosis of milk of calcium.
Suture calcifications
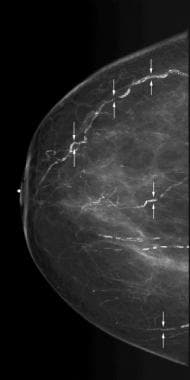
Suture material (see the image below) may become calcified, resulting in suture calcifications. [40, 41] Suture calcifications are usually seen at a known surgical site, and the calcifications may be linear or tubular. Knots may be demonstrated. Suture calcifications are likely due to delayed resorption of catgut sutures, which can provide a matrix on which calcium can precipitate.
Suture calcifications are more common in women who have undergone radiation therapy compared with those who have had benign breast biopsy. Radiation therapy results in delayed tissue healing, and it is likely that suture resorption is also delayed in the radiated breast, allowing for the precipitation of calcium in the catgut sutures. The earliest time at which calcified suture material may become evident on mammography is within 2 years of surgery.
Dystrophic calcifications
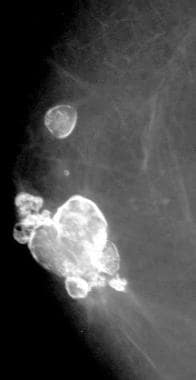
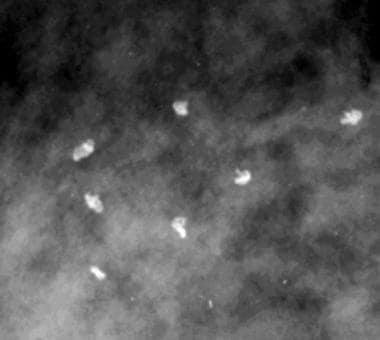
Dystrophic calcifications, as shown in the image below, may form secondary to trauma, surgery, or irradiation.
 This patient's breast was burned. The irregular, large calcifications are dystrophic.
This patient's breast was burned. The irregular, large calcifications are dystrophic.
Most often irregular, dystrophic calcifications are usually larger than 0.5 mm, and they may have lucent centers.
Several studies have shown that women with chronic kidney disease (CKD) or end-stage renal disease (ESRD) have a higher prevalence of breast calcifications. These studies have shown that the majority of calcifications were typically benign, such as vascular calcifications, ductal calcifications located behind the areola or typically oriented toward the nipple, and small, oval, or scattered parenchymal calcifications. [42, 43, 44] [45, 46]
-
Multiple skin calcifications (arrows).
-
Scattered vascular calcifications with train track—like appearance (arrows).
-
This patient was in a car accident and sustained a seatbelt injury. The lucent-centered calcifications seen are typical of fat necrosis.
-
This patient underwent breast-conserving surgery. The lucent-centered calcifications (arrow) are typical of fat necrosis.
-
Multiple silicone granulomas are lucent-centered calcifications.
-
Eggshell or rim calcifications (arrows) have walls thinner than those of lucent-centered calcifications.
-
This mass with associated large, coarse calcifications (arrows) is a degenerating fibroadenoma.
-
Calcifications associated with fibroadenomas have been termed popcorn calcifications because of their large size and dense, coarse appearance.
-
Large rodlike or secretory calcifications are oriented along the axis of the breast ductal system.
-
Scattered round and punctate calcifications (arrows).
-
Left, On the craniocaudal (CC) magnification view, milk of calcium appears poorly defined and smudgy (arrows). Right, On the mediolateral (ML) or the lateromedial (LM) magnification view, milk of calcium is seen as sharply defined, crescent-shaped, semilunar, curvilinear (concave up), or linear arrangements (arrows).
-
Knotted suture calcifications.
-
This patient's breast was burned. The irregular, large calcifications are dystrophic.
-
Benign breast calcification.









