Practice Essentials
Radiologic detection of calcifications within the heart is quite common. The amount of coronary artery calcification correlates with the severity of coronary artery disease (CAD). Calcification of the aortic or mitral valve may indicate hemodynamically significant valvular stenosis. Myocardial calcification is a sign of prior infarction, while pericardial calcification is strongly associated with constrictive pericarditis. Therefore, detecting and recognizing calcification related to the heart on chest radiography and other imaging modalities such as fluoroscopy, CT, and echocardiography may have important clinical implications. [1, 2, 3, 4]
Coronary artery calcium (CAC) progression is associated with coronary and cardiovascular event rates, but it adds only weakly to risk prediction. What counts is the most recent CAC value and risk factor assessment. Therefore, a repeat scan more than 5 years after the first scan may be of additional value, except when a double-zero CT scan is present or when the patients are already at high risk. [5]
See the images of cardiac calcifications below.
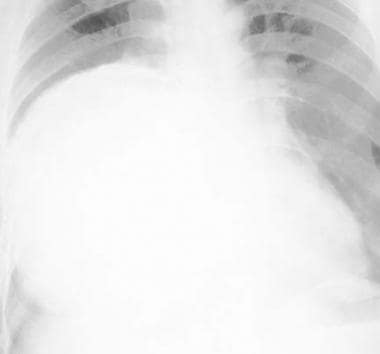 Frontal chest radiograph demonstrates a large calcified pericardial cyst. Courtesy of Mysore Seetharaman, MD.
Frontal chest radiograph demonstrates a large calcified pericardial cyst. Courtesy of Mysore Seetharaman, MD.
 Calcification in a left ventricular aneurysm in a patient with significant coronary artery disease
Calcification in a left ventricular aneurysm in a patient with significant coronary artery disease
 Frontal chest radiograph reveals calcification involving the ascending aorta in a patient with syphilitic aortitis. Courtesy of Mysore Seetharaman, MD.
Frontal chest radiograph reveals calcification involving the ascending aorta in a patient with syphilitic aortitis. Courtesy of Mysore Seetharaman, MD.
In patients with diabetes mellitus, by determining the presence of coronary calcifications, patients at risk for future myocardial infarction and coronary artery disease could be identified, and future events could be excluded if no coronary calcifications were present. [6]
A study of participants from the Multi-Ethnic Study of Atherosclerosis (MESA), a prospective cohort study of 6814 males and females aged 45 to 84 years without known cardiovascular disease from 4 race/ethnicity groups (white [38.5%], African American [27.5%], Hispanic [22.1%], and Chinese [11.9%]) reported CAC scores had significant long-term (>10 years) value in prognosticating cardiovascular disease in patients with metabolic syndrome and diabetes. A CAC score of 0 was associated with low cardiovascular disease risk independent of diabetes duration, insulin use, or glycemic control. [7]
A separate study of MESA participants found patients with CAC and extra-coronary calcium (ECC) are at markedly higher risk of incident hypertension and may benefit from more intensified prevention efforts. [8]
In an asymptomatic population, determination of the presence of coronary calcifications identified patients at risk for future myocardial infarction and coronary artery disease independent of concomitant risk factors. In patients without coronary calcifications, future cardiovascular events could be excluded. [9]
Coronary Artery Calcium Scoring (CACS)
Coronary artery calcium scoring (CACS) is a measure of coronary artery calcification detected on electron beam CT (EBCT) or helical CT. It is a marker of the atherosclerotic plaque burden and is an independent predictor of future myocardial infarction and mortality. CACS provides incremental risk information beyond traditional risk calculators. To calculate a CAC score, the original Agatston method involved defining a calcified lesion as a density of 130 Hounsfield units or more and an area of 3 or more pixels. A score was assigned to each lesion (the product of density and area), and the total score was reached by adding up each of the calcified lesion scores. A semiautomated Agatston method is now commonly utilized based on coronary artery calcification detected by unenhanced low-dose CT. Patients with a high Agatston score (>160) have an increased risk for a major adverse cardiac event. [10, 11, 12]
Cardiovascular risk stratification using calcium scoring has been widely studied, and standard categories according to cardiovascular prognosis and total mortality are as follows:
-
CAC=0: very low risk of death (< 1% at 10 years)
-
CAC=1-100: low risk of death (< 10% at 10 years)
-
CAC=101-400: intermediate risk of death (10-20% at 10 years)
-
CAC=101-400 and >75th percentile for age, sex, and ethnicity: moderately high risk of death (15-20% at 10 years)
-
CAC >400: high risk of death (>20% at 10 years)
Pericardial Calcifications
Calcification of the pericardium is usually preceded by a prior episode of pericarditis or trauma. Occasionally, pericardial tumors, such as intrapericardial teratomas and pericardial cysts, can calcify. [13] CT is the best technique to detect pericardial calcification; however, overpenetrated films, conventional tomography, fluoroscopy, and MRI may be helpful. The normal pericardium is 1-2 mm thick and composed of an outer fibrous layer and an inner serous layer, which subdivides into a visceral layer, or epicardium, and a parietal layer. The pericardium normally lacks any calcium deposits. Calcification may be a sign of underlying inflammation or another cause. Signs and symptoms of pericardial calcification can develop because of an underlying disease process such as constrictive pericarditis. Pericardial calcification alone, however, is generally asymptomatic. Chest radiography may identify pericardial calcification but has low sensitivity. CT can provide excellent detail of both the heart and the pericardium. [14, 15]
(See the images below.)
Frontal chest radiograph demonstrates a large calcified pericardial cyst. Courtesy of Mysore Seetharaman, MD.
 Lateral chest radiograph of the same patient shown in the previous image reveals calcified pericardial cyst.
Lateral chest radiograph of the same patient shown in the previous image reveals calcified pericardial cyst.
On chest radiographs, pericardial calcification appears as curvilinear calcification usually affecting the right side of the heart (see the images below). This is often visualized better on lateral chest radiographs than on frontal views. Calcifications associated with tuberculous pericarditis present as thick, amorphous calcifications along the atrioventricular groove. This pattern may be observed less commonly with other forms of pericarditis as well.
 Note the calcification along the left heart border over the right ventricle in this patient with calcific pericarditis.
Note the calcification along the left heart border over the right ventricle in this patient with calcific pericarditis.
 On the lateral view, thick nodular calcification is observed over the right ventricle, representing pericardial calcification.
On the lateral view, thick nodular calcification is observed over the right ventricle, representing pericardial calcification.
Myocardial Calcifications
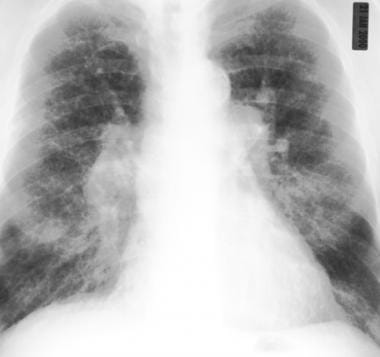
Myocardial calcification usually occurs in patients who have sustained sizable infarcts. Calcification is identified as thin and curvilinear shaped and usually appears toward the apex of the left ventricle. The associated contour abnormality from the aneurysm is frequently noted. Rarely, calcification can appear spherical or platelike. The walls of the left ventricle rarely calcify, and calcification of the mural thrombus in the aneurysm is more common. Rarely, calcification is noted in cardiac tumors, such as rhabdomyomas and endotheliomas. The CTs and radiograph below show a patient with calcification in a left ventricular aneurysm. [16]
Calcification in a left ventricular aneurysm in a patient with significant coronary artery disease
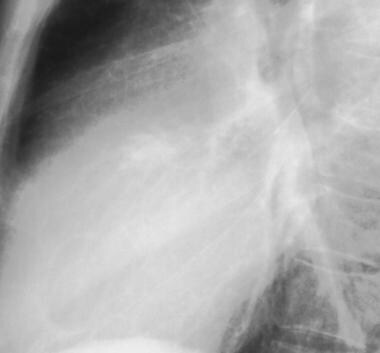
 Lateral chest radiograph from the patient shown in the previous image demonstrates calcification within the left ventricular aneurysm.
Lateral chest radiograph from the patient shown in the previous image demonstrates calcification within the left ventricular aneurysm.
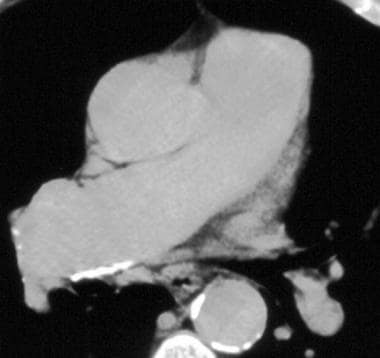
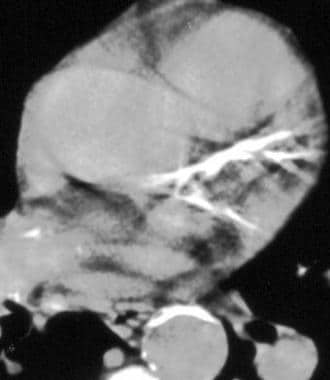
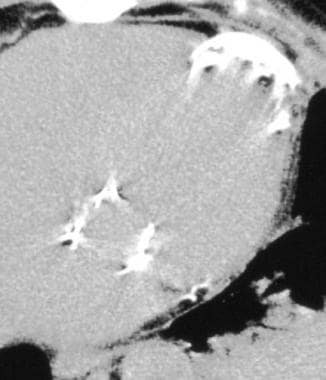 Non–contrast-enhanced CT of the patient seen in the previous 2 images reveals calcification within the left ventricular aneurysm.
Non–contrast-enhanced CT of the patient seen in the previous 2 images reveals calcification within the left ventricular aneurysm.
Left Atrial Calcifications
Detection of left atrial wall calcification has significant clinical implications. Most of these patients have congestive heart failure and atrial fibrillation from long-standing mitral valve disease. LA calcification usually is secondary to endocarditis resulting from rheumatic heart disease, and the amount of calcification is often related to the duration of untreated disease. [17] LA calcification may be in the endocardial or subendocardial layer or within a thrombus. Complete calcification of the left atrium has been termed coconut atrium or porcelain atrium. Interatrial septal puncture during balloon mitral valvotomy can be difficult because of thickened and calcified interatrial septum. [18] Calcification is usually thin and curvilinear, as can be seen in the radiographs below.
 Calcification within the left atrium in a patient with a history of rheumatic heart disease and mitral valve replacement
Calcification within the left atrium in a patient with a history of rheumatic heart disease and mitral valve replacement

Valvular Calcifications
Valvular calcification identified radiographically suggests the presence of a hemodynamically significant stenosis. Dominant valvular insufficiency is not associated with radiographic depiction of calcification, except in patients with calcified stenotic valves secondarily destroyed by endocarditis. The aortic valve calcification is detected most frequently. [19]
In bicuspid aortic valves, calcification may be nodular, semilunar, or mushroom shaped. A dilated ascending aorta often is seen. A thick, irregular, semilunar ring pattern with a central bar or knob is typical of stenotic bicuspid valves and results from calcification of the valve ring and the dividing ridge of the 2 cusps or the conjoined leaflet, as seen in the radiograph below.
 Lateral chest radiograph demonstrating thick calcification of a bicuspid aortic valve in a patient with previously repaired coarctation
Lateral chest radiograph demonstrating thick calcification of a bicuspid aortic valve in a patient with previously repaired coarctation
In mitral valve calcification, a nodular or amorphous pattern of calcification is observed, and signs of rheumatic mitral stenosis frequently are present. These include enlargement of the LA, especially the LA appendage, and pulmonary venous hypertension with cephalization and interstitial edema seen as Kerley B lines. Detection of mitral valve calcification from chest radiographs is uncommon; echocardiographic detection is far more common. Detection of the calcification has surgical implications, since in such instances valve replacement is preferred to commissurotomy.
Calcification of the pulmonary valve occurs rarely in patients with pulmonary valvular stenosis. If valve calcification is identified radiologically, the gradient across the valve often exceeds 80 mm Hg; valvar calcification also may be observed in patients with long-standing, severe pulmonary hypertension.
Tricuspid valve calcification is rare and is most frequently caused by rheumatic heart disease; however, it has been associated with septal defects, congenital tricuspid valve defects, and infective endocarditis.
Annular Calcifications
Annular calcification is a degenerative process. [20, 21] A, J, U, or reverse C-shaped bandlike calcification is observed involving the mitral annulus. [22] Calcification can appear O-shaped if the anterior leaflet also is involved. Calcification appears bandlike and of uniform radiopacity compared to the nodular and more irregular opacity of mitral valve calcification, as shown in the radiograph below.

Vascular Calcifications
The aortic arch has been identified as the most vulnerable site for calcifications in the thoracic aorta. Aortic arch calcification (AAC) is detectable on chest radiogaph and can accurately represent the magnitude of calcified change throughout the entire aorta. Calcification involving the aortic arch is observed as a curvilinear density along the ascending aorta and the arch. [23, 24, 25]
Syphilitic aortitis, an inflammatory aortitis involving the ascending aorta, sinuses of Valsalva, and the aortic valve, is associated with aortic insufficiency, ascending aortic aneurysms, and a positive serologic test for syphilis. In these patients, calcification occurs in a linear pattern along the ascending aorta. On gross specimen examination, the aorta has been described as revealing a "tree-bark" appearance, as shown in the frontal chest radiograph below.
Frontal chest radiograph reveals calcification involving the ascending aorta in a patient with syphilitic aortitis. Courtesy of Mysore Seetharaman, MD.
Calcification of the pulmonary artery is rare and almost always represents long-standing pulmonary hypertension. It may involve the main and/or central pulmonary arteries (see the images below).
 Calcification in the right main pulmonary artery in a patient with chronic, interstitial lung disease and pulmonary hypertension
Calcification in the right main pulmonary artery in a patient with chronic, interstitial lung disease and pulmonary hypertension
 Frontal chest radiograph in the same patient as in the previous image reveals changes of diffuse, interstitial lung disease. Pulmonary artery calcification is barely visualized.
Frontal chest radiograph in the same patient as in the previous image reveals changes of diffuse, interstitial lung disease. Pulmonary artery calcification is barely visualized.
Calcification of the ductus arteriosus is observed on a frontal chest radiograph as a curvilinear or nodular density between the aorta and pulmonary trunk.
Coronary (artery) Calcifications
Evaluation of patients with coronary artery disease (CAD) includes patient history (including review of symptoms and significant coronary risk factors), physical examination, and evaluation of a resting ECG. In patients with symptoms suggestive of CAD, additional investigation, including the physiologic response to stress, may be indicated. This may include stress ECG, stress echocardiography or MRI, or radionuclide perfusion imaging. Coronary calcification is a recognized marker for atherosclerotic CAD. Calcification can be identified on plain radiographs, fluoroscopy, and CT. More reproducible CT evaluation, including quantitation of coronary calcium, may be performed using helical and electron beam CT (EBCT).
Physicians are increasingly using CT detection of calcification to detect subclinical CAD, which may result in early initiation of diet and drug therapy.
Dedicated cardiac CT scans have standardized slice thickness, acquisition protocols, ECG gating to minimize cardiac motion, and reconstruction protocols. There is also a standardized quantitation for gated cardiac CT scans using the Agatston score, which has been well validated. [26, 4, 27]
Nongated 256-detector row chest CT has been shown to be reliable for detecting and quantifying calcifications in coronary arteries, when compared to dedicated calcium-scoring CT. In a study by Chen et al, for example, sensitivity and specificity of nongated chest CT for determining CAC was 94.8% (182/192) and 100%, respectively. [28]
In a retrospective study of women 40 years of age or older who underwent a digital screening mammogram within 2 years of having a cardiac catheterization, benign arterial calcifications (BACs) and a history of smoking and hypercholesterolemia were all significant predictors of coronary artery disease (CAD). Routine screening digital mammography could potentially assist in stratification of patients in consideration of CAD. [29, 30]
Imaging of coronary calcification
Numerous modalities exist for identifying coronary calcification, including plain radiography, fluoroscopy, intravascular ultrasound, MRI, echocardiography, and conventional, helical, and electron-beam CT (EBCT). [31, 32, 33, 34, 35, 36]
Plain radiographs have poor sensitivity for detection of coronary calcification and have a reported accuracy as low as 42% (see the image below). [37, 38]
 Frontal chest radiograph demonstrates calcification involving the left anterior descending coronary artery.
Frontal chest radiograph demonstrates calcification involving the left anterior descending coronary artery.
Fluoroscopy was the most frequently used modality in detecting coronary artery calcification before the advent of CT. The ability of fluoroscopy to detect small, calcified plaques is poor. In one study, only 52% of calcific deposits observed on EBCT were identified fluoroscopically. In addition, fluoroscopy is operator dependent, and certain patient characteristics (eg, body habitus, overlying anatomic structures, calcification in overlying anatomic regions) can compromise fluoroscopic examination. [39, 40]
CT is highly sensitive for detecting calcification. In a study using calcification on CT as a marker of significant angiographic stenosis, sensitivities of 16-78% were reported. [41] Reported specificities were 78-100%, and positive predictive values were 83-100%, suggesting that CAD may be likely to occur when coronary calcification is observed on CT. Conventional CT demonstrates calcification in 50% more vessels than fluoroscopy does in patients with angiographically proven stenosis. However, conventional CT has a slower scan time and is more prone to artifacts from cardiac and respiratory motion and volume averaging than helical or EBCT. [42, 43, 44, 45, 46, 47]
Electron-beam CT
EBCT minimizes motion artifacts, since cardiac-gated imaging can be triggered by the R wave of the cardiac cycle. [48] Imaging can be performed in diastole, minimizing cardiac motion. Typically, 20 contiguous, 100-millisecond, 3-mm thick sections are obtained during 1 or 2 breath-holds. Coronary calcification is observed as a bright white area along the course of coronary vessels.
Helical CT
Scans are performed with acquisition times approaching 0.5 second to 250 milliseconds; the faster acquisition is possible with the newer multidetector scanners. Calcific deposits are identified as bright white areas along the course of coronary arteries (see the image below). [49, 50, 51, 52]
 Helical non–contrast-enhanced CT reveals calcification involving the left main coronary artery.
Helical non–contrast-enhanced CT reveals calcification involving the left main coronary artery.
Coronary calcifications detected on EBCT or helical CT can be quantified, and a total calcification score can be calculated. In this schematic, an arbitrary pixel threshold of +130 Hounsfield units (HU) (+90 for some helical scanners) covering an area greater than 1 mm is often used to detect coronary artery lesions. Regions of interest are placed around the area of calcification. Once the region of interest is placed, scanner software displays peak calcification, attenuation in HU, and area of the calcified region in millimeters squared. The volume or Agatson score is displayed. The volume score is the area of the lesion, while the Agatson score is weighted to consider attenuation of pixels, as well as the area.
In the Agatson scoring system, +130-200 HU lesions are multiplied by a factor of 1, +201-300 HU by a factor of 2, +301-400 HU lesions by a factor of 3, and lesions greater than 401 HU by a factor of 4. The sum of the individual lesion scores equals the score for that artery, and the sum of all lesion scores equals the total calcification score.
In one study, a total calcification score of 300 had a sensitivity of 74% and a specificity of 81% in detecting obstructive CAD. The negative predictive value of a zero calcification score was 98%. In another study, sensitivity for detecting calcific deposits in patients with angiographically significant stenosis was 100%, and specificity was 47%. In the same study, 8 patients without calcification showed no angiographic evidence of CAD, while 28 patients with calcification showed mild or moderate CAD.
However, despite the high sensitivity of EBCT, calcification scores do not always predict significant stenosis at the site of calcification. [53, 54] In another study, EBCT was compared with coronary angiography; only 1 patient with stenosis greater than 50% on angiography did not demonstrate coronary calcification on EBCT. Thus, absence of calcification appears to be a good predictor of the absence of significant luminal stenosis. However, absence of calcification does not always indicate the absence of atherosclerotic plaque.
A multicenter study reviewed cardiac event data in 501 mostly symptomatic patients with CAD who underwent both EBCT and coronary angiography. In this group, 1.8% of patients died and 1.2% had nonfatal myocardial infarctions during a mean follow-up period of 31 months. A calcification score of 100 or more was revealed to be highly predictive in separating patients with from those without cardiac events.
Conclusion
The amount of coronary calcification relates to the extent of atherosclerosis, although the relationship between arterial calcification and the probability of plaque rupture is unknown. A zero calcification score is a good predictor of absence of significant CAD. Detecting extensive coronary calcification on CT appears to be a marker of significant atherosclerotic burden and serves as an indication for a more aggressive evaluation of coronary risk factors and an early institution of dietary and/or drug therapy. [55]
Questions & Answers
Overview
How is cardiovascular risk stratification determined with coronary artery calcium scoring (CACS)?
What is cardiac calcification?
What is coronary artery calcium scoring (CACS)?
What is the role of CT scanning in the identification of pericardial calcifications?
Which findings on chest radiography are characteristic of pericardial calcifications?
Which imaging findings are characteristic of myocardial calcifications?
Which imaging findings are characteristic of left atrial calcifications?
Which imaging findings are characteristic of valvular calcifications?
Which imaging findings are characteristic of annular calcifications?
Which imaging findings are characteristic of vascular calcifications?
What is in included in the workup of coronary artery calcifications?
Which imaging modalities are used to evaluate coronary calcification?
What is the accuracy of radiography for the evaluation of cardiac calcification?
What is the role of fluoroscopy in the imaging workup for cardiac calcifications?
What is the accuracy of CT scanning for the evaluation of cardiac calcifications?
What is the role of EBCT in the imaging workup of cardiac calcification?
What is the role of helical CT in the imaging workup of cardiac calcification?
-
Frontal chest radiograph demonstrates a large calcified pericardial cyst. Courtesy of Mysore Seetharaman, MD.
-
Lateral chest radiograph of the same patient shown in the previous image reveals calcified pericardial cyst.
-
Note the calcification along the left heart border over the right ventricle in this patient with calcific pericarditis.
-
On the lateral view, thick nodular calcification is observed over the right ventricle, representing pericardial calcification.
-
Calcification in a left ventricular aneurysm in a patient with significant coronary artery disease
-
Lateral chest radiograph from the patient shown in the previous image demonstrates calcification within the left ventricular aneurysm.
-
Non–contrast-enhanced CT of the patient seen in the previous 2 images reveals calcification within the left ventricular aneurysm.
-
Calcification within the left atrium in a patient with a history of rheumatic heart disease and mitral valve replacement
-
Lateral chest radiograph of a patient with left atrial calcification
-
Lateral chest radiograph demonstrating thick calcification of a bicuspid aortic valve in a patient with previously repaired coarctation
-
Mitral annular calcification in an asymptomatic patient
-
Frontal chest radiograph reveals calcification involving the ascending aorta in a patient with syphilitic aortitis. Courtesy of Mysore Seetharaman, MD.
-
Calcification in the right main pulmonary artery in a patient with chronic, interstitial lung disease and pulmonary hypertension
-
Frontal chest radiograph in the same patient as in the previous image reveals changes of diffuse, interstitial lung disease. Pulmonary artery calcification is barely visualized.
-
Frontal chest radiograph demonstrates calcification involving the left anterior descending coronary artery.
-
Helical non–contrast-enhanced CT reveals calcification involving the left main coronary artery.





