Practice Essentials
Long-term central venous access devices (an example of which is shown below) are increasingly being used for the administration of antibiotics and chemotherapeutic drugs, for total parenteral nutrition, and for providing high-flow access for hemodialysis and plasmapheresis. Indwelling catheters also offer the ability to obtain frequent blood samples, which may be needed in some patients. Increasing numbers of these devices are being placed in the same patients. This practice can prove to be challenging when traditional venous access sites are used repeatedly, because of the resultant stenosis or occlusion of the central vessels. Although routine chest radiographs to verify correct central venous catheter (CVC) position and exclude pneumothorax are commonly performed, bedside ultrasonography avoids radiation while verifying correct placement and lack of pneumothorax without delay. Evidence suggests that routine chest radiographs may be unnecessary and can be replaced by bedside ultrasound. [1, 2, 3]
Traditionally, interventional radiology (IR) did not play a significant role in the placement of venous access devices. In the past, IR was involved in the fluoroscopic evaluation of occluded catheters, the repositioning of misplaced catheters, or the percutaneous retrieval of lost catheter fragments. [4, 5] However, as operating room schedules became tighter, IR procedures became easier to schedule; in many instances, IR procedures are also more cost-effective. [6, 7, 8, 9, 10, 11, 12]
Smit et al performed a meta-analysis of 25 studies reporting diagnostic accuracy of ultrasound in detecting the position of CVCs and the mechanical complications associated with insertion. A total of 2602 CVC placements were included in the analysis, with a pooled specificity of 98.9 (95% confidence interval (CI): 97.8-99.5) and sensitivity of 68.2 (95% CI: 54.4-79.4). The prevalence of CVC malposition and pneumothorax was 6.8% and 1.1%, respectively. The mean time for ultrasound performance was 2.83 minutes (95% CI: 2.77-2.89 min), and chest radiograph performance was 34.7 minutes (95% CI: 32.6-36.7 min). Bedside ultrasound was feasible in 97% of cases. [2] .
In a population-based retrospective cohort study performed to review the records of 6,875 adult patients who had ultrasound-guided CVC placement in the operating room, the overall incidence of pneumothorax and catheter misplacement was 0.33% (95% CI, 0.22-0.5) (23 patients) and 1.91% (95% CI, 1.61-2.26) (131 patients), respectively. The study concluded that because pneumothorax and catheter misplacement after ultrasound-guided CVC insertion were rare, the high costs of routine postprocedural chest radiographs were not justified. [1]
A systematic review and meta-analysis was conducted to examine the accuracy of bedside ultrasound for confirmation of CVC position and exclusion of pneumothorax compared with chest radiography. Fifteen studies with 1,553 central venous catheter placements were identified, with a pooled sensitivity and specificity of catheter malposition by ultrasound of 0.82 (0.77-0.86) and 0.98 (0.97-0.99), respectively. The pooled positive and negative likelihood ratios of catheter malposition by ultrasound were 31.12 (14.72-65.78) and 0.25 (0.13-0.47). The sensitivity and specificity of ultrasound for pneumothorax detection was nearly 100% in the participating studies. Bedside ultrasound reduced mean central venous catheter confirmation time by 58.3 minutes. [3]
Most patients tolerate central venous access with local analgesia. Tunneled catheters, port placement, and other forms of complicated venous access may require intravenous pain medications and/or moderate conscious sedation, which most interventionalists are capable of providing in the IR suite. In extreme cases, consultation with the anesthesia department may be necessary.
Guidelines
The American College of Radiology has offered the following guidance on the radiologic management of central venous access [13] :
-
Tunneled double-lumen small-bore central venous catheter (CVC) and chest port are the best choices for administration of long-term total parenteral nutrition (PN) and intermittent intravenous antibiotics. Chest ports are recommended as the first choice for intravenous access for the treatment of recurrent sickle cell crisis.
-
Tunneled small-bore single-lumen CVC provides the best option for the administration of long-term antibiotics (6 weeks or more) in patients with stage 3 chronic kidney disease. A nontunneled CVC is the most appropriate CVC to use in a patient admitted to the hospital with acute or chronic renal insufficiency requiring short-term antibiotics (approximately 7-10 days) for acute sepsis.
-
The contralateral internal jugular vein is the most appropriate venous access site for hemodialysis in a patient with end-stage renal disease who has undergone creation of an arteriovenous fistula and the fistula has not yet matured.
-
The presence of fever and malaise alone in an immunocompromised patient is not an indication for removal of a tunneled CVC. However, the catheter should be removed if positive blood cultures are confirmed.
-
For a patient requiring head and neck surgery for cancer, arm or chest ports and peripherally inserted central catheters (PICCs) are recommended for intravenous access for chemotherapy.
-
Chest radiograph and contrast study of the catheter are the recommended first steps for assessing a dysfunctional chest port and other CVCs.
-
For suspected thrombotic complications leading to a dysfunctional tunneled dialysis catheter, catheter removal and placement of a new catheter from a different site, catheter exchange, contrast study of the catheter, and fibrin sheath stripping or disruption are excellent next steps. An attempt should be made to perform dialysis with the patient arm in a different position. Arm swelling secondary to extensive thrombus surrounding a functioning, in-use peripherally inserted CVC should be treated by anticoagulation without removal of the catheter.
Imaging Guidance in Venous Access
Achieving traditional central venous access by using the jugular, subclavian, or femoral veins or by using surface landmarks may be sufficient in many patients. The internal jugular veins are probably the most commonly used sites for tunneled catheters. However, coagulopathy and the patient's body habitus may limit the use of surface landmarks in obtaining safe access, even in routinely used vessels, such as the internal jugular and subclavian veins. Interventional radiologists are trained to rely on imaging guidance as a means of obtaining venous access.
Most IR suites are equipped with dedicated ultrasonography machines, or ultrasonography equipment is readily available and can be used to evaluate the site of planned vascular access before catheter placement (see the images below). [14] Small, handheld, portable ultrasound units can be used, even at the bedside.
 Transverse ultrasonogram of the neck demonstrates the jugular vein (Jug) next to the carotid artery (Car).
Transverse ultrasonogram of the neck demonstrates the jugular vein (Jug) next to the carotid artery (Car).
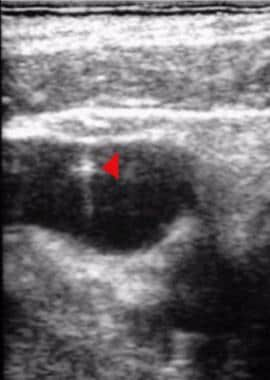 Note the bright echogenic tip of the micropuncture needle as it enters the jugular vein (arrowhead).
Note the bright echogenic tip of the micropuncture needle as it enters the jugular vein (arrowhead).
Most ultrasonography units are equipped with a needle guide; however, the use of a needle guide often requires scanning of the vessel in a longitudinal plane, which does not allow the operator to keep the adjacent artery in view at all times.
At the authors' institution, needle guides are not used because, without them, entering the vein freehand while scanning in the horizontal plane and keeping the adjacent artery in view at all times is easier and prevents inadvertent arterial puncture. The vessel is usually entered in a freehand fashion by using a single-wall 21-g auge needle and suction applied with a syringe while the needle is withdrawn until blood flows freely. Then, the guidewire is advanced under fluoroscopic guidance.
Ultrasonography has the additional advantage of depicting thrombosed veins. Once such a vein is identified, placing a needle into the thrombosed vessel and advancing a guidewire through the occluded vessel into the central circulation may be possible. This can allow a catheter to be placed through a site that could not have been accessed by using traditional techniques.
Ultrasonographic investigation of the neck may demonstrate multiple small collateral vessels instead of a single large jugular vein, which usually indicates a stenosis or occlusion of the main vein. In many instances, one of the collateral veins can be accessed under direct ultrasonographic visualization.
If a guidewire cannot be easily advanced into the central circulation, a small amount of iodinated contrast material can be injected to identify central venous stenosis or occlusion. Medical-grade carbon dioxide gas can be safely used in patients with severe allergy to intravenous contrast agents or in patients with compromised renal function.
The gas is difficult to see under fluoroscopy, and digital subtraction angiography is needed for imaging. Carbon dioxide gas is useful in visualizing venous anatomy, occlusion, and collaterals, and it is inexpensive as well. Care must be taken to prevent contamination with room air.
Gadolinium-based contrast agents should not be used as a vascular contrast agent because of the development of nephrogenic systemic fibrosis (NSF) or nephrogenic fibrosing dermopathy (NFD). The disease has occurred in patients with moderate to end-stage renal disease after being given a gadolinium-based contrast agent to enhance magnetic resonance imaging (MRI) or magnetic resonance angiography (MRA) scans. NSF/NFD is a debilitating and sometimes fatal disease. Characteristics include red or dark patches on the skin; burning, itching, swelling, hardening, and tightening of the skin; yellow spots on the whites of the eyes; joint stiffness with trouble moving or straightening the arms, hands, legs, or feet; pain deep in the hip bones or ribs; and muscle weakness.
If a significant stenosis is identified, the radiologist has access to an armamentarium of catheters and guidewires that can be used to access the central circulation. Most often, a hydrophilic wire, such as a Glidewire with an angled tip, can be negotiated through a severe stenosis into the central circulation.
Predilation with an appropriately sized angioplasty balloon allows placement of a central venous catheter in a vessel that could not have been accessed with traditional access techniques. With similar techniques, guidewires can be manipulated into the central circulation through small collateral veins, again allowing placement of a catheter via vessels that could not be used otherwise.
Ultrasonography allows the safe puncture of veins in patients with coagulopathy, because arterial puncture can be avoided. In these patients, the authors often use a micropuncture needle system, such as the Micropuncture Introducer Kit with a 21-gauge needle. This needle allows safe access into the venous system with a 0.018-inch-diameter guidewire, versus the 0.035-inch guidewire and a 19-gauge needle included with most venous access catheters.
The transitional dilator supplied with the micropuncture kit allows exchange of the 0.018-inch guidewire for a standard 0.035-inch guidewire. If any doubt remains about which vessel has been accessed after placement of the 0.018-inch guidewire or if the guidewire cannot easily be advanced into the central circulation, the smaller inner dilator (3F) of the micropuncture kit can be placed and injected with iodinated contrast material or carbon dioxide. This avoids placement of a 5F catheter or a peel-away sheath into a vessel that may not be suitable for use or may be the arterial system. This is especially important in a patient with coagulopathy.
Use of the micropuncture technique under ultrasonographic guidance can also allow the safe access of vessels without discontinuing anticoagulation therapy.
Once a guidewire has been negotiated into the central circulation, transitional dilators are used to dilate the tract to the appropriate size. This is best accomplished under fluoroscopic guidance to avoid kinking the guidewire. The peel-away sheath can then be introduced into the central circulation for final placement of the catheter. Pinching the peel-away sheath or having the patient hold his or her breath during the introduction of the catheter through this sheath is important in preventing the complication of an air embolism. Many new peel-away sheaths have a valve for prevention of an air embolism. If the table can be tilted, placing the patient in the Trendelenburg position can also minimize the risk of air embolism.
If an air embolism does occur, the patient should be immediately positioned in the left lateral decubitus position so that the air can remain in the right heart chambers until it is slowly resorbed. Life support measures should then be initiated as dictated by the clinical situation.
Nontraditional Access Sites
If traditional venous access sites are not usable because of thrombosis, nonconventional central venous access can be achieved by placing a transhepatic central venous catheter or a translumbar inferior vena cava (IVC) catheter. [15, 16, 17, 18]
Transhepatic and translumbar venous access should be used only as a last resort, because they may induce thrombosis of the hepatic veins or IVC. Small central lines can be placed through collateral vessels, such as the intercostal vessels or chest wall collaterals if needed.
Transhepatic IVC access
A transhepatic approach is relatively easy and can be performed by using a 15-cm-long, 22-gauge Chiba needle via a midaxillary approach through the level of ribs 10-12. The Chiba needle is advanced above the rib into the liver parenchyma, as during percutaneous transhepatic cholangiography, and a small amount of dilute water-soluble contrast material is injected under fluoroscopy as the needle is withdrawn. The only difference is that, in this case, the goal is to opacify a hepatic vein instead of the biliary tree. Alternatively, ultrasonographic guidance may be used to enter a peripheral right hepatic vein branch.
Once a suitable peripheral hepatic vein is opacified, a 0.018-inch-diameter Cope Mandril Wire Guide is advanced into the IVC. An AccuStick or other similar transitional dilator system allows the 0.018-inch guidewire to be exchanged for a standard 0.035-inch guidewire. An appropriately sized peel-away sheath is placed, and the catheter is advanced through it to the cavoatrial junction under fluoroscopy.
The external portion of the catheter then can be tunneled subcutaneously, and either a subcutaneous-port catheter or an external type of catheter (eg, Hickman catheter or a tunneled dialysis catheter) is placed. [19]
Translumbar IVC access
The IVC is accessed with the aid of fluoroscopy by advancing a 22-gauge Chiba needle just lateral to the right edge of the L2-3 lumbar vertebral body with the patient in a prone or prone-oblique position. Once venous blood is aspirated, a 0.018-inch guidewire can be advanced into the IVC. The remainder of the procedure is similar to transhepatic catheter placement.
A long tunnel is often made so that the catheter can exit the skin on the patient's side rather than from his or her back. This allows the patient to take better care of the catheter at the exit site, because reaching a site on his or her back may be a problem. Depending on the application, the distal tip of the catheter can be extended into the cavoatrial junction or positioned below the level of the renal veins.
If the IVC cannot be accessed by using fluoroscopic landmarks, venous access can be achieved under CT scan guidance. Ultrasonographic guidance may be used in children or patients with a smaller body habitus. [20, 21, 22] Alternatively, a pigtail catheter or an angiographic guidewire can be placed in the IVC from the femoral venous approach or through a preexisting femoral venous catheter and used as a marker for fluoroscopy-assisted puncture of the IVC if the femoral veins are patent.
Access Devices
Many types of venous access devices are available. Each has its own advantages and disadvantages, and the radiologist must be familiar with these. To select the appropriate device, the physician must have a complete understanding of the indications for central venous access and of the available access vessels in the individual patient, as well as the length of time for which access is needed. Patient preference combined with an understanding of the patient's lifestyle should be taken into consideration. When given a choice, most patients prefer the use of their nondominant side for the placement of peripheral lines.
The prophylactic administration of antibiotics or presoaking of the catheters in an antibiotic solution may decrease the risk of infection with the more permanent tunneled type of catheters. Catheters impregnated with antibiotics may have lower rates of line-related infections. [23] Such antibiotics need to be given at the start of the procedure or within 30 minutes of the initiation of the procedure.
Peripherally inserted central catheters
Traditionally, peripherally inserted central catheters (PICCs) have been placed at the bedside by trained IV technologists or nurses. However, non–image-guided PICC lines can be placed into visible superficial veins that are large enough to accommodate 3-5F catheters. If superficial access sites have been used or if advancing the catheter into the central circulation is difficult, central lines are traditionally used. Non–image-guided placement of PICC lines can result in catheter tip malpositioning (eg, placement of the tip into the internal jugular vein or contralateral brachiocephalic vein). [24] Subsequent repositioning may be required.
Routine use of ultrasonography or contrast-enhanced venography allows the radiologist to place PICC lines into deeper veins, such as the basilic, cephalic, brachial, and axillary veins. [25] PICC systems specifically designed for radiologic placement, such as the Vaxcel system or RadPICC, must be used. These catheters differ from traditional PICC lines in that they are over-the-wire systems (usually placed over a 0.018-inch guidewire), and they come with peel-away sheaths longer than those of standard PICCs.
Alternatively, standard PICC lines that are routinely placed by IV teams all across the country, such as the Bard Groshong PICC, may be used. Their main disadvantage is that they do not track over a guidewire, but they have the unique advantage of the Groshong valve, which prevents blood from staying within the catheter. Thus, they do not need to be flushed as often as the open-ended PICCs. [26]
The authors prefer ultrasonographic access for the upper arm veins. If a central venous occlusion is identified, the guidewire can often be manipulated through small collateral veins into the central circulation, allowing placement of the PICC.
Ports
Traditionally, single- and double-lumen chest ports have been placed by surgeons. Smaller port designs, such as the R-Port, allow ports to be placed in the arm; these are preferred by many patients. Lower profile chest ports, such as the P.A.S. Port T2 Power P.A.C., is also CT injector compatible.
Strict adherence to surgical scrub techniques and proper surgical attire with caps, gowns, and masks are crucial when the ports are placed, to minimize the risk of infection. IR suites equipped with operating room–quality positive airflow and microfilters are best suited for the placement of such devices.
Some operators routinely provide antibiotic prophylaxis to provide coverage against skin flora. Venous access is obtained by using ultrasonographic guidance, as described previously. [27] Alternatively, water-soluble contrast material can be injected through an IV line in the ipsilateral arm, and the central veins can be directly accessed by using fluoroscopy. The catheter is then tunneled for a short distance, and a small subcutaneous pocket is created for placement of the port.
The ideal location for the reservoir is thought to be along the anteromedial aspect of the second rib. This high medial position keeps the port away from the breast tissue and prevents inadvertent retraction of the catheter once the patient is upright. The port should be sutured to the underlying fascia to prevent it from twisting or rotating.
Hemodialysis catheters
Patients undergoing hemodialysis pose special challenges in terms of placing long-term venous access devices. High-flow-rate catheters are needed in these patients to meet the requirements of modern hemodialysis machines. Desired flow rates are typically at least 250-300 mL/min, with higher rates (400-500 mL/min) being more desirable.
Catheters must be precisely placed away from the vessel wall and side branches, and they require frequent maintenance in most patients. Access can be difficult because of the central venous occlusions and stenoses that develop in these patients as a result of multiple prior catheterizations.
Balloon angioplasty and stent placement may be needed to provide ongoing access. Long-term results of adjunctive procedures in keeping central vessels patent are often poor, but they may allow catheter placement. Older, poorly functioning dialysis catheters can be treated with thrombolytic agents. Fibrin sheaths often develop around these catheters, resulting in poor flow rates. The radiologist can help clear these catheters by using adjunctive treatment such as stripping them off with a snare or exchanging the catheters out over guidewires.
Radiologic Intervention for Catheter-Related Complications
Complications associated with venous access devices may be categorized as early or late. Early complications include procedural complications directly related to catheter placement, such as arterial puncture or injury, pneumothorax, venous rupture, air embolism, catheter malpositioning, and catheter transection that results in the catheter's migration. The rates of most complications can be significantly reduced with the aid of imaging guidance during catheter placement.
Late complications of venous access devices include catheter-related infection [28] , catheter occlusions, and catheter fracture and migration. Catheter-related infections often require removal of the catheter and concurrent antibiotic treatment. Other late complications and the tools available to help the interventional radiologist overcome them are discussed below.
Catheter occlusion or malfunction
Catheter occlusions are commonly related to the formation of a thrombus within the lumen, the formation of a fibrin sheath around the catheter end, the malpositioning of a catheter tip against the vessel wall or within a small branch vessel, or the presence of thrombosis or stenosis in the native vein.
Catheter thrombosis may be treated with thrombolytic agents, such as tissue-type plasminogen activator (t-PA) (eg, alteplase) or reteplase. [29, 30] The entire lumen of the catheter is filled with approximately 2 mg of t-PA diluted in the appropriate volume to fill the catheter. This is left in place for 15-30 minutes. Care must be taken to infuse just enough solution so that it fills only the lumen of the catheter and to prevent systemic administration of the thrombolytic agent. After the appropriate time, the thrombolytic agent is aspirated.
The procedure may result in clearing the thrombus within or around the tip of the catheter. If this fails, short infusions of t-PA through the catheter, as described by Savader et al (2.5 mg over 3 hours), may be used. [31] If such an infusion is used, the patient must be appropriately monitored in the hospital, because this treatment entails exposing the patient to systemic thrombolytic therapy.
If catheter thrombolysis fails, occluded catheters can often be replaced with a new catheter by using a guidewire. When placing tunneled catheters, the authors make a small cutdown over the previous access site, then cut and remove the catheter over a stiff, angled glidewire and finally create a new tunnel to minimize the risk of infection. However, replacement of the catheter over 1 or 2 stiff glidewires has been described and is routinely used in many centers. [32]
The formation of a fibrin sheath around a catheter can be seen as soon as 24 hours after catheter placement. Fluid infusion through the catheter might still be possible, but the fibrin sleeve usually prevents the withdrawal of blood, because it acts as a valve.
The fibrin sheath can be easily identified under fluoroscopy by injecting the catheter with a small amount of water-soluble contrast agent. The presence of a fibrin sheath is indicated by contrast material that does not exit the tip of the catheter but instead flows back along the catheter for a short distance before being carried forward by blood flow. [33, 34]
The traditional treatment option is catheter replacement. However, the radiologist has several methods for removing the fibrin sheath. A guidewire can be advanced through the catheter and used to create a hole in the fibrin sheath. Unfortunately, this usually results in the creation of only a small hole that can easily become reoccluded. In addition, many catheters have side holes that remain covered by the fibrin sheath. An angled guidewire can be placed through the catheter and used to clear each hole under fluoroscopy, but this procedure is cumbersome and may create small holes that are prone to reocclusion.
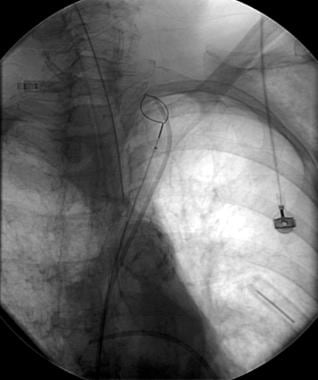
A better approach is to attempt to remove the entire fibrin sheath. [35] Usually, this is performed via a femoral venous approach. An appropriately sized loop snare, such as an Amplatz Goose Neck Snare, is advanced through the IVC and used to capture the catheter. [36] This snare, once placed around the catheter, is moved up around the proximal portion of the catheter. Then, the snare is tightened over the catheter and pulled back across the distal end of the catheter to dislodge the fibrin sheath. (A fibrin sheath and the snare used to remove it are seen in the images below.)
 The injection of contrast material through a Hickman catheter demonstrates the presence of a fibrin sheath at its tip).
The injection of contrast material through a Hickman catheter demonstrates the presence of a fibrin sheath at its tip).
 Magnification view of the tip of the catheter demonstrates the fibrin sheath (same patient as in the previous image).
Magnification view of the tip of the catheter demonstrates the fibrin sheath (same patient as in the previous image).
 An Amplatz snare has been used to strip off the fibrin sheath. Note the free flow of contrast material from the catheter tip (same patient as in the previous 2 images).
An Amplatz snare has been used to strip off the fibrin sheath. Note the free flow of contrast material from the catheter tip (same patient as in the previous 2 images).
If the catheter is wedged against the wall and cannot be freed, a pigtail catheter can often be rotated alongside the catheter in the brachiocephalic vein or in the superior vena cava (SVC) to move the catheter away from the wall. Alternatively, a guidewire can be advanced through the catheter down into the right atrium or IVC. Then, the snare can be advanced from below, over the guidewire, to snare the catheter tip. If a wire is placed through the catheter, the hub of the catheter may be presoaked in Betadine to reduce the risk of infecting the catheter.
An alternative approach to breaking up the fibrin sheath is to remove the catheter over a guidewire and use an angioplasty balloon to disrupt the fibrin sheath before a new catheter is placed.
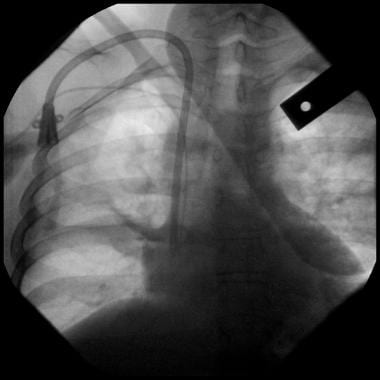
Catheters may not function adequately if the catheter tip migrates into a branch vessel or if it is against the vessel wall (see the images below). The catheter tip can be redirected by replacing the catheter over a guidewire or, in the case of tunneled catheters, by redirecting the tip by using a snare from a femoral venous approach. However, redirecting catheters that have migrated into a branch vessel may be only a temporary measure, because migration may recur.
 Digital chest image demonstrates that the tip of a Hickman catheter has migrated into the right jugular vein.
Digital chest image demonstrates that the tip of a Hickman catheter has migrated into the right jugular vein.

Catheters may malfunction as a result of thrombosis of the native vessel in which the catheter was placed. If the patient is symptomatic because of vessel thrombosis, catheter-directed thrombolytic therapy may be pursued. A catheter with multiple side holes can be placed through the area of thrombus, and catheter-directed thrombolytic therapy can be initiated.
In many patients, an underlying stenosis may be uncovered after the thrombosis has been found. The stenosis can be treated by using balloon angioplasty or stent placement, as needed. Unfortunately, balloon angioplasty of venous lesions is not as successful as in arterial lesions. Stent placement through an area of narrowing can result in an immediate angiographic cure, but long-term results are often poor.
Catheter fracture or malpositioning
Fractures can occur along the intravascular or extravascular portions of the catheter. Most catheter manufacturers sell repair kits to fix external catheter problems; these kits should be readily available. If an appropriate length of the external catheter remains, the damaged portion of the catheter can be cut off, and a new hub can be attached to allow continued use of the same catheter.
If the subcutaneous extravascular course of the catheter is between the clavicle and first rib, pinch-off syndrome may result. [37] The catheter can become occluded, and with repeated trauma, this can result in catheter fracture and embolization of the distal fragment. [38]
Pinch-off syndrome can be avoided by using the jugular venous approach. The catheter fragment can become lodged in the heart, resulting in cardiac arrhythmias or possible cardiac perforation or embolization to the pulmonary artery.
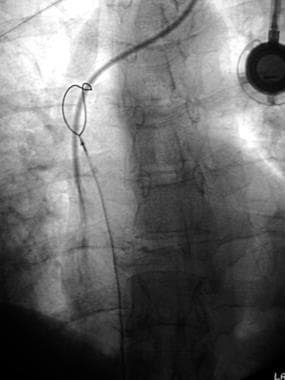
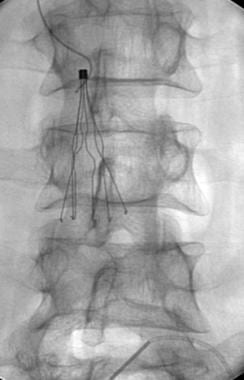
If recognized early, the interventional radiologist can usually capture the catheter fragments and successfully remove them. If the fragments within the central vasculature remain unrecognized, thrombus formation and fibrosis around the catheter can result in catheter attachment to the vessel wall. (The removal of a catheter fragment with a snare, using the right femoral approach, is shown below.)
 Digital image demonstrates a snare being placed over the proximal catheter fragment via the right femoral approach.
Digital image demonstrates a snare being placed over the proximal catheter fragment via the right femoral approach.
 Radiograph demonstrates a snare that is being used to pull back a catheter into the inferior vena cava (same patient as in the previous image).
Radiograph demonstrates a snare that is being used to pull back a catheter into the inferior vena cava (same patient as in the previous image).

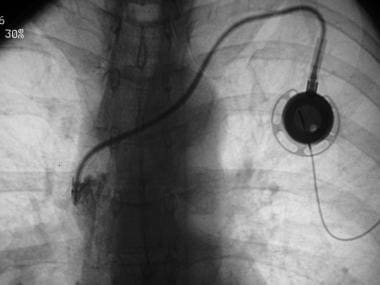
The tip of an intact catheter can migrate into the opposite brachiocephalic vein, jugular vein, or azygous veins. If a catheter was placed without imaging guidance, it may have been placed in an artery or in one of these vessels. IR can play an important role in repositioning misplaced catheters. With tunneled catheters that have migrated, a snare can be passed up from a femoral venous approach to redirect the catheter into the appropriate location. Occasionally, a catheter can be buckled down into the SVC by advancing a guidewire through it, allowing the catheter to flip into the SVC.
Complications associated with guidewires
Guidewires used for venous access can become trapped in indwelling vena cava filters or electrodes from pacemakers and other implantable devices (see the images below). Occasionally, the authors are consulted by clinical colleagues about a stuck guidewire that cannot be removed in a patient with a filter. Fluoroscopy often demonstrates that the J-wire has become trapped around the tip of an IVC filter.
 Abdominal radiograph demonstrates a J-wire trapped in the apex of a Greenfield filter. The wire became trapped during blind placement of a central venous line.
Abdominal radiograph demonstrates a J-wire trapped in the apex of a Greenfield filter. The wire became trapped during blind placement of a central venous line.
 Magnified image demonstrates the J-wire trapped in the apex of a Greenfield filter (same patient as in the previous image).
Magnified image demonstrates the J-wire trapped in the apex of a Greenfield filter (same patient as in the previous image).
 A catheter was advanced over the wire and used to gently remove the trapped wire from the Greenfield filter (same patient as in the previous 2 images).
A catheter was advanced over the wire and used to gently remove the trapped wire from the Greenfield filter (same patient as in the previous 2 images).
The usual tendency of the operator who is placing the line is to keep pulling back on the wire in the hope of dislodging it. Unfortunately, this maneuver can result in the migration of the filter, with catastrophic results, such as a tear in the wall of the IVC caused by the filter hooks. However, the guidewire usually unravels inside the patient. Most guidewires are made of a central mandril with fine wire wound around it. Excessive pulling on the guidewire causes the wire to unwind, and the operator simply keeps pulling back the flimsy wire that is several times longer than the overall length of the original wire. In many instances, the wire tip remains entangled in the filter.
Several techniques are available to the radiologist to remove broken wires or wires trapped in filters. A 5F catheter can gently be passed over the remaining guidewire down to the filter, and the remaining wire can slowly be advanced to try to release the J-tip from the filter. This is the portion of the wire that is usually stuck on the filter. Alternatively, a snare can be used to grasp the end of the wire and to try to twist it and pull it to free it from the filter. High-magnification fluoroscopy is important during these maneuvers, and care must be taken to ensure that the entire wire has been removed and that a fragment has not been left behind or become embolized distally.
Caution should thus be taken in placing lines in such patients with indwelling vena cava filters because of the risk of the wire tip getting trapped on the filter. Central lines should be placed in these patients only under fluoroscopic guidance.
Subcutaneous ports may invert in the subcutaneous space. This phenomenon is sometimes referred to as twiddler's syndrome. Distending the fibrous capsule with 5-10 mL of sodium chloride solution may provide enough space to manually rotate the reservoir within the capsule, as described by de Costa et al. [39]
-
Chest radiograph demonstrates an entire Swan catheter within the venous system with no residual catheter portion outside the patient.
-
Digital image demonstrates a snare being placed over the proximal catheter fragment via the right femoral approach.
-
Radiograph demonstrates a snare that is being used to pull back a catheter into the inferior vena cava (same patient as in the previous image).
-
Retrieved catheter fragment (same patient as in the previous 2 images).
-
Abdominal radiograph demonstrates a J-wire trapped in the apex of a Greenfield filter. The wire became trapped during blind placement of a central venous line.
-
Magnified image demonstrates the J-wire trapped in the apex of a Greenfield filter (same patient as in the previous image).
-
A catheter was advanced over the wire and used to gently remove the trapped wire from the Greenfield filter (same patient as in the previous 2 images).
-
The injection of contrast material through a Hickman catheter demonstrates the presence of a fibrin sheath at its tip).
-
Magnification view of the tip of the catheter demonstrates the fibrin sheath (same patient as in the previous image).
-
An Amplatz snare has been used to strip off the fibrin sheath. Note the free flow of contrast material from the catheter tip (same patient as in the previous 2 images).
-
Digital chest image demonstrates that the tip of a Hickman catheter has migrated into the right jugular vein.
-
The tip of a Hickman catheter has been redirected into the superior vena cava.
-
Transverse ultrasonogram of the neck demonstrates the jugular vein (Jug) next to the carotid artery (Car).
-
Note the bright echogenic tip of the micropuncture needle as it enters the jugular vein (arrowhead).
-
Central venous access.




