Practice Essentials
Pulmonary hypoplasia is a developmental abnormality of the lung characterized by a decrease in the number of alveoli, cells, and airways, eventually resulting in decreased size and weight of the lungs. Pneumothorax and respiratory distress are common in affected infants. Although pulmonary hypoplasia is occasionally a primary condition, [1] most cases are secondary to other abnormalities that prevent complete pulmonary development. Pulmonary hypoplasia is frequently associated with malformations of the cardiac, genitourinary, gastrointestinal, and musculoskeletal systems. Bronchopulmonary malformations are also associated with this disease. [2, 3, 4, 5, 6, 7]
Imaging modalities
Antenatal ultrasonography provides early predictors of pulmonary hypoplasia. [8, 9, 10, 11] Magnetic resonance imaging (MRI) is used in some centers to assess fetal volume and predict the presence of pulmonary hypoplasia. [12] After birth, chest radiography shows changes of pulmonary hypoplasia, which is better demonstrated on computed tomography (CT) scans. Any vascular abnormality is also assessed with CT scanning or contrast-enhanced magnetic resonance angiography.
The American College of Radiology (ACR) and Society of Pediatric Radiology (SPR) joint guidance on the safe and optimal performance of MRI during pregnancy endorses the use of MRI at any stage of pregnancy for further evaluation of any anomly found on ultrasound. Specific indications include volumetric assessment of fetal lung parenchyma for secondary hypoplasia in at-risk fetuses. [13]
(See the following images.)

Other problems to consider
Atelectasis, persistent pulmonary hypertension, pulmonary agenesis, pulmonary aplasia, and proximal interruption of pulmonary artery should be considered. Unlike agenesis or aplasia, pulmonary hypoplasia results in bronchi and alveoli that are intact. The pulmonary artery is usually small or, sometimes, absent. [14] In pulmonary agenesis, the lung is absent, as are the bronchi, airways, and pulmonary vasculature. The right and left sides are affected equally, but the prognosis is worse if the right side is involved because of associated severe congenital malformations. The affected side has reduced volume, and patients have homogeneous opacification of the entire lung, with a mediastinal shift to the same side. Compensatory overinflation of the opposite lung and herniation and congenital malformation are associated findings. In pulmonary aplasia, the lung is absent, but a rudimentary blind ending bronchus is present. [15, 16]
Radiography
Pulmonary hypoplasia is usually unilateral but is occasionally seen bilaterally. The volume of the chest is reduced on the affected side; the affected lung is small; and the mediastinum is shifted toward the side of the hypoplastic lung (see the following image). There is also an increased ipsilateral mediastinal shift during inspiration because of increased volume of the contralateral lung. In addition, a bell-shaped thorax and rib deformities are frequently observed, the lung is more lucent than normal (homogeneous opacification can also be seen), and the hilum is small because of a hypoplastic or aplastic pulmonary artery. Other associated lung and vertebral anomalies are also noted. [17]
Computed Tomography
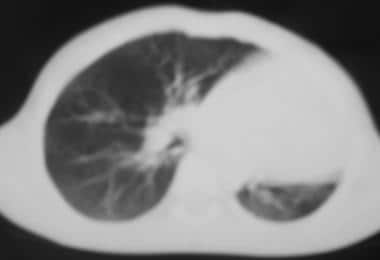
CT scans show an abnormally shaped thorax, volume reduction on the affected side, compensatory overinflation of the opposite side, ipsilateral mediastinal shift, hypoplastic airways, and rib abnormalities (see the images below).
With the advent of multisection CT scanners, CT angiography can be performed in a few minutes with intravenous contrast and images reconstructed in multiple planes. This study is a noninvasive way of assessing pulmonary vasculature, as compared to conventional angiography. The pulmonary arteries are hypoplastic. Aberrant vasculature can be seen, as well as associated cardiac abnormalities, scimitar syndrome, diaphragmatic abnormalities, and gastrointestinal and genitourinary abnormalities.
Magnetic Resonance Imaging
MRI of the fetus is being increasingly used to predict the presence of pulmonary hypoplasia. [12] Factors used for prediction are (1) the fetal lung volume, (2) the relative lung volume, and (3) the ratio of lung volume to body weight (which is the most widely used ratio). [18, 19, 20, 21, 22]
Fetal lung volume is measured by obtaining thin sections of the lung. The cross-sectional area is calculated by drawing an outline of the lung and estimating the area within it. Volume of each section is obtained by multiplying the area by the section thickness.
To determine the relative lung volume, the percentage of lung volume is calculated relative to the expected lung volume for the patient's gestational age. This parameter is not applicable when the fetus is macrosomic or has retardation.
A combination of MRI and ultrasonography can also be used to predict the development of pulmonary hypoplasia. Tanigaki et al used the ratio of fetal lung volume measured by means of MRI and fetal body weight estimated by means of ultrasonography for this purpose. [23]
The use of lung-to-liver signal intensity ratio (LLSIR) on T2-weighted images to predict fetal pulmonary hypoplasia has been proposed. [24]
Postnatally, MR angiography is a reliable method of assessing pulmonary vasculature, which can be hypoplastic and aberrant but not completely absent (unlike agenesis).
Ultrasonography
As discussed in the MRI section, antenatal ultrasonography can be used to predict development of pulmonary hypoplasia. [9, 10, 25, 26, 27, 28] Features that are useful in predicting pulmonary hypoplasia are (1) the lung area; (2) the ratio of lung area to thoracic area; (3) the ratio of thoracic to abdominal circumference; and (4) lung volume, which can be measured by using many techniques, including 3-dimensional ultrasonography.
Ultrasonography can be used to assess factors contributing to pulmonary hypoplasia, such as oligohydramnios, renal agenesis, renal obstruction, renal cysts, renal dysplasia, diaphragmatic hernia, thoracic and abdominal masses, and pleural effusion. Associated congenital malformations can also be seen.
Doppler ultrasonography of the fetal pulmonary arteries is a useful study in capable hands. In hypoplasia, the development of pulmonary vasculature is delayed and the vessels are hypoplastic, resulting in increased impedance. This results in increased pulsatility index and decreased peak systolic velocity.
Direct visualization of hypoplasia is possible with proper technique and well-trained ultrasonographers. Associated anomalies, which contribute to development of pulmonary hypoplasia, can be detected with confidence.
Nuclear Imaging
Perfusion scans obtained by using albumin microspheres can show defects due to decreased pulmonary vascularity. This type of scanning is not an important investigation in pulmonary hypoplasia. However, this nuclear imaging can be used to differentiate Swyer-James syndrome (unilateral acquired hyperlucent lung due to obliterative/constrictive bronchiolitis) and proximal pulmonary arterial interruption, which can have similar radiographic appearances.
In Swyer-James syndrome, the perfusion scan is normal, but there is expiratory obstruction seen as a filling defect in ventilatory scans. High-resolution CT scans, however, are usually sufficient to make the diagnosis. In proximal pulmonary arterial interruption, there is complete absence of uptake in perfusion scans, but ventilatory scans are normal.
Angiography
In the past, angiography was commonly used to confirm the diagnosis of pulmonary hypoplasia. Findings include a patent and hypoplastic pulmonary artery (unlike in agenesis, in which it is absent) and an association with a proximally interrupted pulmonary artery with patent intraparenchymal branches that anastomose with systemic collateral vessels. Aberrations and associated scimitar syndrome can also be detected. With the advent of CT angiography and magnetic resonance angiography, conventional angiography is no longer required to confirm the diagnosis.
-
Radiograph showing left pulmonary hypoplasia.
-
Computed tomography scan showing pulmonary hypoplasia on the left side.
-
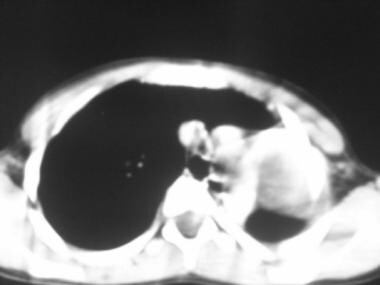
Computed tomography scan (mediastinal window) shows a hypoplastic left lung.
-
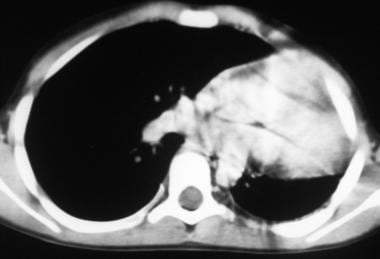
Computed tomography scan (mediastinal window) shows left pulmonary hypoplasia.





