Practice Essentials
Gastric cancer is the most common cancer in the world after lung cancer and is a major cause of mortality and morbidity. Though a marked reduction has been observed in the incidence of gastric carcinoma in North America and Western Europe in the last 50 years, 5-year survival rates are less than 20%, as most patients present late and are unsuitable for curative, radical surgery. The most common sites of metastasis are the peritoneum (61-80%), distant lymph nodes (44-50%), and liver (26-38%). [1] Adenocarcinomas account for approximately 95% of all malignant gastric neoplasms. The remaining 5% of tumors are lymphomas, leiomyosarcomas, carcinoids, or sarcomas. [2, 3] There are a number of gastric cancer subtypes, including papillary, tubular, and signet ring cell forms.
The most popular classification of gastric cancer is the Lauren classification, which divides gastric cancer into 2 subtypes: intestinal and diffuse. The World Health Organization (WHO) classification has issued a very detailed classification system, which describes gastric adenocarcinomas and other types of gastric tumors. [4, 2, 5, 6]
The imaging techniques that are performed for a gastric cancer diagnosis, as well as for staging, include endoscopic ultrasonography (EUS), computed tomography (CT), and positron emission tomography (PET)-CT. [1, 7, 8, 9] Double-contrast barium upper GI examination is widely recognized as the radiologic technique of choice for diagnosing early gastric cancers. Single-contrast barium studies have an overall sensitivity of 75% in the detection of gastric cancer, but double-contrast barium examinations have a sensitivity of 90-95%, which is comparable to that of endoscopy. CT scanning, MRI, and EUS are used in the staging of gastric cancer, but not usually in primary detection of the disease. [10, 11, 12, 13, 14, 15, 16, 17, 18, 19]
(Gastric tumors are shown in the images below.)


Gastric adenocarcinomas are divided into 2 types. Type 1 adenocarcinomas are intestinal tumors and have well-formed glandular structures. This form of gastric carcinoma is more likely to involve the distal stomach and to occur in patients with atrophic gastritis (seen in the image below). It has a strong environmental association. A type 2 adenocarcinoma is a diffuse type with poorly cohesive cells, which tend to infiltrate the gastric wall. Tumors of this type may involve any part of the stomach, especially the cardia; they have a worse prognosis than type 1 tumors.
Guidelines
National Comprehensive Cancer Network (NCCN) guidelines for the diagnosis of gastric cancer include the following [20] :
-
Endoscopy is the primary procedure for diagnosis, surveillance, and staging of gastric cancer.
-
Endoscopic ultrasound (EUS) is preferred if early stage disease is suspected or if early versus locally advanced disease needs to be determined.
-
Multiple biopsies should be performed, especially with ulcerated lesions.
-
Endoscopic mucosal resection (EMR) or endoscopic submucosal dissection (ESD) of small lesions (eg, focal nodules ≤2 cm) can be safely performed to provide a larger specimen that may contribute to accurate staging of early stage cancers; in addition, such excisional biopsies are potentially therapeutic.
-
Chest/abdomen/pelvic CT with oral and IV contrast are recommended.
-
PET/CT evaluation (skull base to mid-thigh) is recommended if there is no evidence of M1 disease and if clinically indicated.
-
Biopsy of metastatic disease is recommeded as clinically indicated.
-
High microsatellite instability/deficient mismatch repair (MSI-H/dMMR) testing is recommended if metastatic disease is documented or suspected.
-
HER2 and PD-L1 testing is recommended if metastatic adenocarcinoma is documented or suspected.
The 2019 British Society of Gastroenterology guidelines on the diagnosis and management of patients at risk of gastric adenocarcinoma recommends image-enhanced endoscopy as the best imaging modality to accurately diagnose and stage early gastric cancer. [21]
Prognosis and staging
The prognosis of gastric carcinoma is related to the stage of the disease at the time of diagnosis and to the histologic grade of the carcinoma. [22, 23, 24, 25, 26, 27, 28]
Pathologic staging of these neoplasms is based on tumor stage, nodal stage, and metastasis stage (TNM). The stages are as follows [29] :
The T stage, representing the extent of penetration through the gastric wall, is categorized as follows:
-
Tis - Carcinoma in situ: intraepithelial tumor without invasion of the lamina propria
-
T1 - Tumor invades lamina propria, muscularis mucosae, or submucosa
-
T1a - Tumor invades lamina propria or muscularis mucosae
-
T1b - Tumor invades submucosa
-
T2 - Tumor invades muscularis propria
-
T3 - Tumor penetrates subserosal connective tissue without invasion of visceral peritoneum or adjacent structures
-
T4 - Tumor invades serosa (visceral peritoneum) or adjacent structures
-
T4a - Tumor invades serosa (visceral peritoneum)
-
T4b - Tumor invades adjacent structures
The N stage, representing the number and site of draining lymph nodes involved, is categorized as follows:
-
N0 - No lymph nodes involved
-
N1 - Metastasis in 1-2 regional lymph nodes
-
N2 - Metastasis in 3-6 regional lymph nodes
-
N3 - Metastasis in 7 or more regional lymph nodes
-
N3a - Metastasis in 7-15 regional lymph nodes
-
N3b - Metastasis in 16 or more regional lymph nodes
The M stage, representing the presence of metastases, is categorized as follows:
-
M0 - No distant metastases
-
M1 - Distant metastases
Table: Staging and 5-Year survival rates (Open Table in a new window)
Stage |
TNM Stage |
5-Year Survival |
1 |
T1N0-1M0 or T2N0M0 |
76.5% |
2 |
T1N2-3M0, T2N1-2M0, T3N0-1M0 or T4aN0M0 |
46.3% |
3 |
T2N3M0, T3N2-3M0, T4aN1-3M0 or T4bN0-3M0 |
18.3% |
4 |
TxNxM1* |
5.7% |
*Tx indicates any T stage; Nx, any N stage. |
||
Radiography
Early gastric cancer
Double-contrast barium upper GI examination is widely recognized as the radiologic technique of choice for diagnosing early gastric cancers. These lesions are confined to the mucosa or submucosa and are classified into 3 types:
-
Type I - Elevated lesions that protrude more than 5 mm into the lumen
-
Type II - Superficial lesions that are elevated (IIa), flat (IIb), or depressed (IIc)
-
Type III - Shallow, irregular ulcers surrounded by nodular, clubbed mucosal folds
Advanced carcinoma
Gastric carcinomas are occasionally seen on plain abdominal radiographs as abnormalities in the gastric contour or as soft-tissue masses indenting the gastric contour. Rarely, mucin-producing carcinomas may show areas of punctate calcification.
On barium studies, gastric carcinomas may be polypoidal, ulcerative, or infiltrating lesions.
Polypoid carcinomas (an example of which appears below) are lobulated masses that protrude into the lumen. They may contain 1 or more areas of ulceration.
With ulcerated carcinomas, an irregular crater is located in a rind of malignant tissue. Seen en face, tumor nodules may be in the adjacent mucosal folds; the mucosal folds that converge to the edge of the ulcer may be blunted, nodular, or clubbed from tumor infiltration. Seen in profile, these lesions are intraluminal, whereas benign ulcers project beyond the contour of the stomach. The radiating folds associated with a benign ulcer are regular and extend close to the ulcer margins (see the image below). Endoscopy and biopsy are generally required to confirm or rule out malignancy in most cases of gastric ulcers.
 Gastric ulcer with symmetrical, radiating mucosal folds. At histologic evaluation, no evidence of malignancy was observed.
Gastric ulcer with symmetrical, radiating mucosal folds. At histologic evaluation, no evidence of malignancy was observed.
Infiltrating carcinomas result in irregular narrowing of the stomach, with nodularity or spiculation of the mucosa (see the image below).
Special considerations
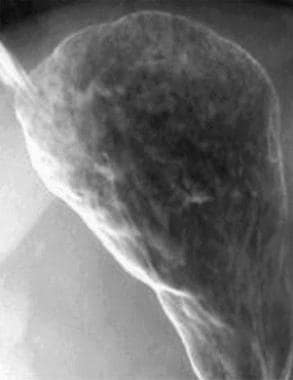
Scirrhous carcinomas typically cause irregular narrowing and rigidity of the stomach, giving rise to the typical linitis plastica, or "leather bottle," appearance (as seen in the image below). Although some are lobulated lesions in the fundus or body, others consist of thickened, irregular mucosal folds and nodularity without significant narrowing.

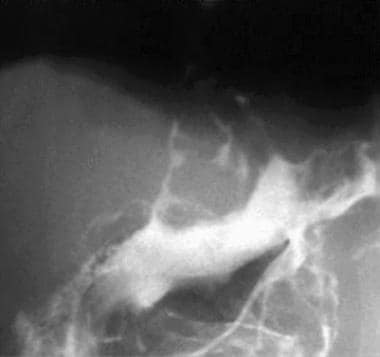
Carcinomas of the cardia are often missed during single-contrast examinations. In double-contrast studies, normal anatomic landmarks are obliterated and replaced by a plaquelike lesion with nodularity or ulceration. The distal esophagus is often involved. (See the images below.)

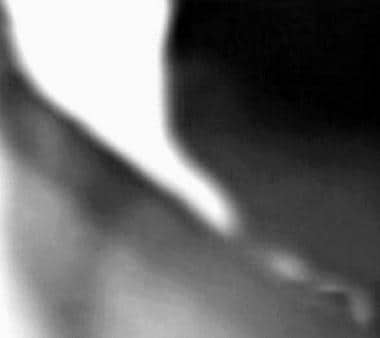
Submucosal spread of tumors may result in pseudoachalasia or secondary achalasia with tapered, beaklike narrowing of the distal esophagus and infiltration of the gastric cardia (see the images below).
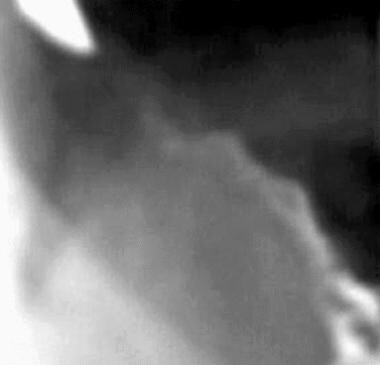 Note malignant infiltration of the cardia (same patient as in the previous image).
Note malignant infiltration of the cardia (same patient as in the previous image).
Degree of confidence
Double-contrast studies have a sensitivity comparable to that of endoscopy.
The appearance of gastric carcinomas on barium studies must be distinguished from the appearances of benign gastric ulcers and polyps, gastric lymphomas, and focal gastritis. Malignant stromal tumors may also cause confusion. Although linitis plastica is usually caused by gastric carcinoma, it can also be caused by metastatic breast cancer.
In rare cases, radiation therapy, Crohn disease, tuberculosis, sarcoidosis, and syphilis may simulate gastric carcinoma, and primary esophageal adenocarcinoma may invade the stomach. Gastric varices and inadequate distention may mimic tumors of the gastric fundus.
Computed Tomography
CT is used preoperatively primarily to determine the stage and extragastric spread of a gastric carcinoma. This information is vital in deciding between palliative surgery and curative radical surgery (ie, identifying patients who would not benefit from radical surgery). Additionally, CT is used to monitor a patient's response to treatment. [18, 19, 30, 31, 32]
Detection of gastric carcinoma is improved by using thin-section sequences and helical or multidetector-row CT (MDCT). [33] When thin collimation is used, near-isotropic imaging of the stomach is possible, allowing high-quality multiplanar reformation and 3-dimensional reconstruction of gastric images. An intravenous contrast medium is used, along with water or gas as a negative intraluminal agent (the results of which are seen in the image below). Prone views improve visualization of tumors of the cardia and distal stomach.
 The stomach is distended by using water as a negative intraluminal contrast agent. Results of this examination are normal.
The stomach is distended by using water as a negative intraluminal contrast agent. Results of this examination are normal.
Helical scanning allows for a biphasic technique. [34] The early arterial phase is used to assess enhancement of the gastric wall; the later portal venous phase is used to assess the liver parenchyma for metastases.
CT scans may show the following:
-
Polypoidal mass with or without ulceration
-
Focal wall thickening with mucosal irregularity or ulceration
-
Wall thickening with the absence of normal mucosal folds (infiltrative lesions)
-
Focal infiltration of the gastric wall (see the image below)
 Carcinoma of the lesser curve. Note the focal mural thickening due to a tumor plaque.
Carcinoma of the lesser curve. Note the focal mural thickening due to a tumor plaque.
-
Variable thickening of the wall and marked contrast enhancement (typical of scirrhous lesions)
-
Mucinous carcinomas, which have low attenuation due to their high mucin content and which may contain calcification

T staging
The depth of tumor invasion is not accurately assessed with CT.
Tumor invasion of the perigastric fat is seen as soft-tissue stranding. Tiny 4- to 8-mm nodules may be observed. These may coalesce into sheets of tumor in advanced cases.
Direct extension of the tumor is relatively common. The pancreas is invaded via the lesser sac; the transverse colon, via the gastrocolic ligament; and the liver, via the gastrohepatic ligament.
Longitudinal spread to the distal esophagus occurs in as many as 60% of patients with carcinoma of the cardia (see the images below). However, the duodenum is involved in only 5-20% of antral carcinomas.

Overall, the accuracy of determining the T-stage with CT is approximately 66%.
N staging
Lymph node metastases occur in approximately 80% of patients with gastric cancer (see the images below). The frequency is related to the size and depth of the tumor; local perigastric nodes are involved first, followed by the regional (celiac, hepatic, left gastric, splenic) and distant (left supraclavicular and axillary) nodes.
 Carcinoma of the body of the stomach associated with regional lymphadenopathy and ascites.
Carcinoma of the body of the stomach associated with regional lymphadenopathy and ascites.
 Enlarged porta hepatis lymph nodes, ascites, and omental involvement (same patient as in the previous image).
Enlarged porta hepatis lymph nodes, ascites, and omental involvement (same patient as in the previous image).
CT depicts 75% of nodes larger than 5 mm in diameter, but it does not depict tumor in normal-sized nodes. CT is not useful in distinguishing between enlarged nodes due to reactive changes and those due to tumor.
The local nodes (N1) are located in the prepyloric region and in the gastrocolic and gastrohepatic ligaments. These nodes are removed by performing the standard gastrectomy procedure. The regional nodes (N2), located in the porta hepatis, hepatoduodenal ligament, and peripancreatic region, are not removed by the gastrectomy procedure; thus, their detection is more important.
M staging
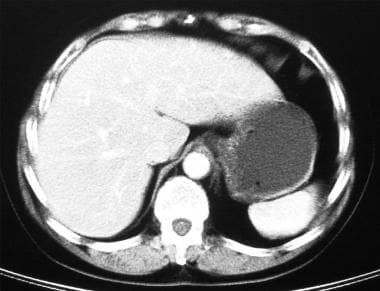
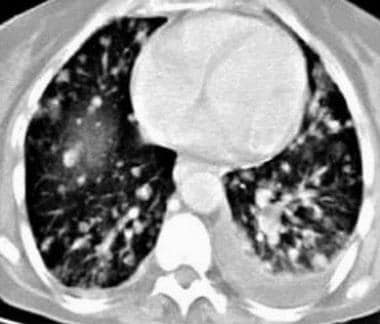
Because the portal vein drains the stomach, the liver is the most common site for hematogenous metastases (see the first image below). Less common sites are the lungs (see the second image below), adrenal glands, and kidneys. Bony and cerebral metastases are uncommon.
 Celiac-axis nodes measure 8-12 mm and are from carcinoma of the cardia. Note the irregular liver metastasis and adjacent rounded cyst.
Celiac-axis nodes measure 8-12 mm and are from carcinoma of the cardia. Note the irregular liver metastasis and adjacent rounded cyst.
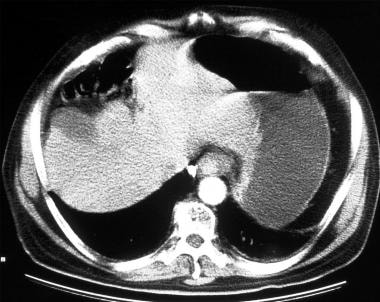
Intraperitoneal and omental metastases are common in advanced gastric cancer. They consist of nodules, localized fluid collections, and irregular thickening and stranding of the mesentery and omentum. Ascites and small-bowel obstruction may occur.
Gastric carcinoma is the most common primary tumor to metastasize to the ovaries. These ovarian metastases are usually bilateral and are known as Krukenberg tumors.
Degree of confidence
In T staging, CT is 43-65% accurate; however, the accuracy of CT increases with the use of the helical biphasic technique. In N staging, CT is 48-70% accurate. Inflammation may cause enlarged nodes. CT scanning has several pitfalls. A pseudomass as a result of a normal gastroesophageal junction may be seen, underdistention of the stomach may simulate wall thickening, and T2 and T3 lesions may be difficult to distinguish.
Moreover, loss of a fat plane between the gastric wall and the left lobe of the liver may be seen. Loss of a fat plane between the tumor and pancreas may be due to an inflammatory reaction. In cachectic patients, a loss of fat planes may simulate direct organ invasion.
Small nodes may contain tumor, and large nodes may result from inflammatory causes. Perigastric nodes may not be observed if the stomach is not well distended.
CT may fail to depict tiny omental and peritoneal deposits; small pelvic deposits may be overlooked as well.
In a study by Jiang et al, the sensitivity of MDCT for a nodal diagnosis of advanced gastric cancer was as high as 91, but specificity was as low as 47% because of the small size of the nodes. [35]
Magnetic Resonance Imaging
MRI studies in which a breath-hold, fast-imaging technique and water were used showed accuracy rates comparable to those of helical, biphasic CT scanning. The fast-imaging technique was found to be superior to CT in detecting serosal invasion. [16]
In T staging, the accuracy of MRI is 73%, compared with 67% for CT. In N staging, the accuracy of MRI is 55%, compared with 59% for CT.
MRI is limited by the presence of respiratory and peristaltic artifacts, the lack of suitable oral contrast media, and a higher cost than that of CT scanning.
Ultrasonography
The primary role of transabdominal ultrasonography (US) is to detect liver metastases. These metastases are usually hyperechoic, but they may be hypoechoic. CT scanning and endoscopic ultrasonography (EUS) are complementary. CT scanning is used first to stage the gastric carcinoma; if no metastases and no invasion of local organs are found, EUS is used to refine the local stage. The depth of tumor invasion is not accurately assessed with CT, and the investigation of choice for this indication is EUS. [10]
Gastric carcinomas are occasionally identified during US of the upper abdomen.
EUS has improved the accuracy of local staging of gastric carcinomas. Its role is to assess the depth of local invasion and the presence or absence of perigastric nodes. Unlike CT and MRI, EUS can depict individual layers of the gastric wall, with a rotating high-frequency probe inserted via an endoscope. EUS is limited to an area 5 cm from the probe. It cannot be used to assess distant metastases or nodes more than 5 cm away from the probe.
The gastric wall is visualized as 5 concentric bands:
-
Mucosa - Echogenic
-
Muscularis mucosa - Hypoechoic
-
Submucosa - Echogenic
-
Muscularis propria - Hypoechoic
-
Serosa - Echogenic
A gastric tumor is demonstrated as a hypoechoic mass with varying mural invasion. Its depth may be overestimated because of the inflammatory response around the tumor, or it may be underestimated because of microscopic spread.
With T1 tumors, wall thickening is limited to the mucosa and submucosa. Regarding N staging, involved nodes are rounder and more hypoechoic than normal nodes.
Degree of confidence
In the detection of liver metastases, sensitivities as high as 85% have been reported.
Overstaging is due to the peritumoral inflammatory response.
In T staging, EUS is 89-92% accurate, and CT is 43-65% accurate; however, the accuracy of CT increases with the use of the helical biphasic technique. In N staging, EUS is 60-85% accurate, and CT is 48-70% accurate. Inflammation may cause enlarged nodes. EUS has a high specificity (90%) but low sensitivity (53-80%) because it has a range of 5 cm from the gastric wall for nodes of normal size; thus, it does not permit assessment of the full extent of lymphadenopathy. Involved small nodes are not detected.
Intraoperative US and laparoscopy have an accuracy of 81% in T staging and an accuracy of 93% in N staging; however, the necessary equipment and expertise are not widely available.
Nuclear Imaging
Fluorodeoxyglucose (FDG) positron-emission tomography (PET) scanning may be useful in the staging and postoperative assessment of gastric carcinomas. FDG-PET depicts the primary tumor, but involved perigastric lymph nodes are not identified separately from the primary tumor. Thus, the role of PET scanning is limited in staging. The use of combined PET-CT scanning may improve diagnostic accuracy. [17, 36]
Indium-111 (111In)–labeled monoclonal antibody has been used for intraoperative imaging to detect nodes, with an accuracy of 72%.
FDG-PET may be useful in evaluating patients with recurrent gastric cancer; findings can help localize the disease when CT findings are not diagnostic. Imaging evaluation with PET may also impact the clinical management of patients with recurrent gastric cancer.
-
Polypoid carcinoma of the body of the stomach.
-
Atrophic gastritis.
-
Gastric ulcer with symmetrical, radiating mucosal folds. At histologic evaluation, no evidence of malignancy was observed.
-
Infiltrating carcinoma involving the greater curve of the stomach.
-
Linitis plastica.
-
Extensive carcinoma involving the cardia and fundus.
-
Carcinoma of the cardia with involvement of the distal esophagus.
-
Secondary or pseudoachalasia due to infiltrating carcinoma of the cardia.
-
Note malignant infiltration of the cardia (same patient as in the previous image).
-
The stomach is distended by using water as a negative intraluminal contrast agent. Results of this examination are normal.
-
Carcinoma of the lesser curve. Note the focal mural thickening due to a tumor plaque.
-
Carcinoma of the cardia. Note the liver metastasis.
-
Tumor extension to the distal esophagus (same patient as in the previous image).
-
Carcinoma of the antrum. Note the circumferential mural thickening.
-
Celiac-axis nodes measure 8-12 mm and are from carcinoma of the cardia. Note the irregular liver metastasis and adjacent rounded cyst.
-
Carcinoma of the body of the stomach associated with regional lymphadenopathy and ascites.
-
Enlarged porta hepatis lymph nodes, ascites, and omental involvement (same patient as in the previous image).
-
Extensive mesenteric, omental, and peritoneal metastases (same patient as in the 2 previous images).
-
Pulmonary metastases and left pleural effusion from a gastric carcinoma.
Tables
Stage |
TNM Stage |
5-Year Survival |
1 |
T1N0-1M0 or T2N0M0 |
76.5% |
2 |
T1N2-3M0, T2N1-2M0, T3N0-1M0 or T4aN0M0 |
46.3% |
3 |
T2N3M0, T3N2-3M0, T4aN1-3M0 or T4bN0-3M0 |
18.3% |
4 |
TxNxM1* |
5.7% |
*Tx indicates any T stage; Nx, any N stage. |
||




