Practice Essentials
The scaphoid is the most frequently fractured carpal bone, accounting for 60-70% of all carpal bone fractures and 2-7% of all fractures. Scaphoid fractures often occur in young and middle-aged adults, typically those aged 15-60 years, after a fall on an outstretched arm that results in acute dorsal flexion of the wrist. About 5-12% of scaphoid fractures are associated with other fractures, and approximately 1% of scaphoid fractures are bilateral. Scaphoid fracture diagnosis is important because 90% of all acute scaphoid fractures heal if treated early. The scaphoid bone can be divided into a distal pole, a waist, and a proximal pole. The most common radiographic findings are scaphoid cortical disruption, hypoechoic radiocarpal fluid due to hemarthrosis, and scapho-trapezium-trapezoid effusion. [1, 2, 3]
Imaging modalities
Radiographic evaluation of a scaphoid fracture begins with conventional radiography. [4] Early diagnosis of a scaphoid fracture is important because nonunion is more likely if treatment is delayed. The initial assessment of stability influences management; a careful evaluation is required. [5, 6, 7]
CT scanning is excellent in the initial evaluation of a scaphoid fracture, particularly in a high-performance athlete in whom initial radiographic findings are normal. Also, CT scanning can demonstrate healing, which is sometimes misleading on radiographs, particularly with hardware in place.
Instead of CT scanning, MRI can be used as a screening tool for patients with negative radiographic results. Also, MRIs may define bone contusions rather than fracture as the source of pain. It has been used in the evaluation of complications, particularly osteonecrosis, but care should be emphasized in the diagnosis of avascularity, because some ischemia is expected in the proximal pole after waist and proximal-pole fractures. Typically, MRI is not useful in the evaluation of healing. [8, 9, 10, 11]
Backer et al performed a meta-analysis comparing the diagnosis of clinically suspected scaphoid fractures in 2507 patients using radiographs, MRI, CT scans, and ultrasonography. Overall, 21.8% of scaphoid fractures were missed on initial radiographs but identified on advanced imaging. MRI was superior to CT and ultrasound, with sensitivities of 94.2%, 81.5%, and 81.5%, respectively, and specificities of 97.7%, 96.0%, and 77.4%. [12]
Ultrasonography can detect dislocated fractures of the scaphoid waist on the basis of cortical disruption. According to Herrera et al, a finding of cortical disruption has a sensitivity of 100%, specificity of 96.5%, postive predictive value (PPV) of 83%, and negative predictive value (NPV) of 100%. However, a diagnosis based on cortical disruption alone is associated with a high false positive rate. Cortical disruption must be associated with articular effusion. [1]
Ultrasonography is limited by the difficulties in scanning the proximal and distal thirds of the scaphoid. Nondislocated fractures are also difficult to detect. Ultrasonography can be used for position monitoring of previously identified childhood fractures, but it requires high operator expertise. [4]
(See the images below.)
 A transscaphoid, perilunate dislocation is present with a fracture of the ulnar styloid. Note the typical dorsal position of the distal carpal row. The distal pole of the scaphoid maintains its relationship to the distal carpal row, while its proximal pole retains its relationship to the proximal carpal row.
A transscaphoid, perilunate dislocation is present with a fracture of the ulnar styloid. Note the typical dorsal position of the distal carpal row. The distal pole of the scaphoid maintains its relationship to the distal carpal row, while its proximal pole retains its relationship to the proximal carpal row.
 Images show delayed union of a scaphoid waist fracture. The radiograph (left) demonstrates the fracture as well as resorption around this 5-month-old fracture. T1-weighted (middle) and fat-suppressed T2-weighted (right) MRI scans demonstrate the fracture without clear evidence of synovial fluid tracking between the fragments. Eventually, this fracture healed.
Images show delayed union of a scaphoid waist fracture. The radiograph (left) demonstrates the fracture as well as resorption around this 5-month-old fracture. T1-weighted (middle) and fat-suppressed T2-weighted (right) MRI scans demonstrate the fracture without clear evidence of synovial fluid tracking between the fragments. Eventually, this fracture healed.
 Scaphoid waist fracture with some resorption, as seen on a posteroanterior image.
Scaphoid waist fracture with some resorption, as seen on a posteroanterior image.
Stress fractures of the scaphoid are rare and have been attributed to repeated or excessive dorsal flexion of the wrist. Carpal scaphoid stress fractures have been reported in athletes engaging in gymnastics, shot put, diving, badminton, tennis, soccer, and cricket. [13]
According to Evenski et al, scaphoid fractures are often missed in children because of their rarity and because of the difficulty in making a radiographic diagnosis. Of 104 cases with high clinical suspicion but no radiographic evidence of scaphoid fracture, 31 (30%) were found to have scaphoid fractures at radiographic follow-up. Volar tenderness over the scaphoid, pain with radial deviation, and pain with active wrist range of motion were identified as significant predictors. As a result of their findings, the investigators recommended that clinically suspected pediatric scaphoid fractures be immobilized, with repeat radiographs and a clinical examination at 2 weeks. [14]
Pierre-Jerome et al studied 125 cases of acute trauma with negative radiographs, but with clinical examination findings suggesting wrist or distal forearm fracture, and they found occult bone injuries in 78 (62.4%) of the 125 wrists. The occult bone injuries included 53 (68%) of the 78 wrists having more than one injured bone and 25 (32%) having one injured bone. The distal radius was the most frequent location for an occult fracture line. The injuries without a fracture line (contusion) were present in 49 (63%) of 78 wrists and were found most frequently in the scaphoid (35 cases). [15]
Ramos-Escalona et al in a retrospective review of radiographs of 66 scaphoid fractures, to evaluate ulnar variance, found that 21 patients (31.8%) had an ulna-neutral wrist; 6 patients (9.1%) had an ulna-plus wrist; and 39 patients (59.1%) had an ulna-minus wrist. The mean ulnar variance was -1.3 mm (range -5.5, 2.5). [16]
Classification
Scaphoid fractures have been classified according to various criteria. For example, they can be grouped according to the anatomic location, as follows (see the image below):
-
Tubercle fractures - These are usually uncomplicated, and if nonunion occurs, they are frequently asymptomatic.
-
Distal-pole fractures - Such fractures are usually uneventful. This group can be subdivided into the following: fractures that involve the articulation with the trapezium and trapezoid; and fractures that do not involve this articulation
-
Proximal-pole fractures - The more proximally located the fracture plane is, the greater the risk of delayed union, nonunion, and avascular necrosis (AVN). [17]
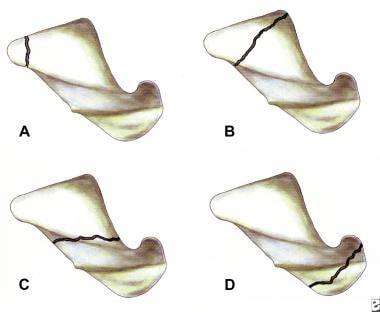 Pictures show the locations of fracture within the scaphoid bone: (A) tubercle; (B) distal pole, or extra-articular (vs intra-articular to scaphotrapezium or trapezoid joint); (C) waist; and (D) proximal pole.
Pictures show the locations of fracture within the scaphoid bone: (A) tubercle; (B) distal pole, or extra-articular (vs intra-articular to scaphotrapezium or trapezoid joint); (C) waist; and (D) proximal pole.
Scaphoid fractures can also be classified according to the plane of fracture with respect to the long axis of the scaphoid, being grouped into horizontal oblique, transverse, and vertical oblique fractures. Increased shear forces in vertical oblique fractures may prolong the time for fracture healing (see the image below).
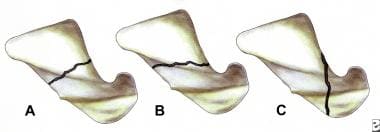 Classification of scaphoid fracture by fracture orientation: (A) transverse, (B) oblique, and (C) vertical.
Classification of scaphoid fracture by fracture orientation: (A) transverse, (B) oblique, and (C) vertical.
Another classification system categorizes scaphoid fractures according to the time of injury and subsequent healing, as follows:
-
Acute
-
Delayed union - An incomplete union after 4 months of cast immobilization
-
Nonunion - An unhealed fracture with smooth, polished surfaces of fibrocartilage
This classification system is used in treatment planning, because a delayed union may be successfully treated with prolonged casting, whereas a nonunion requires internal fixation. About 90% of all acute scaphoid fractures heal if treated early.
The most important classification scheme distinguishes stable scaphoid fractures from unstable ones (see the image below).
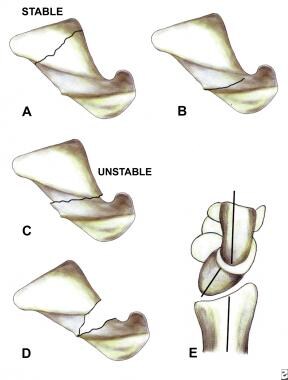 Images illustrate fracture stability. Nondisplaced (A) and incomplete (B) fractures are stable. Displaced fractures (C), angulated fractures (D), and associated ligamentous instability (E), such as dorsal intercalated segmental instability (DISI), are unstable.
Images illustrate fracture stability. Nondisplaced (A) and incomplete (B) fractures are stable. Displaced fractures (C), angulated fractures (D), and associated ligamentous instability (E), such as dorsal intercalated segmental instability (DISI), are unstable.
Stable fractures are incomplete or, if they appear complete, are likely to have an incompletely disrupted articular surface (that is, intact overlying cartilage). Neither displacement nor motion about the fracture occurs with wrist motion. Stable fractures are not associated with ligamentous injury. They are treated with immobilization alone, although stable fractures usually heal regardless of the type of treatment and can even do so without treatment.
Unstable fractures are complete fractures with motion about the fracture site. Findings that indicate instability include cortical offset greater than 1 mm, fracture angulation, associated ligamentous injury, and motion with ulnar or radial deviation. Ligamentous injury most frequently involves the scapholunate ligament; the scapholunate interval may widen, or a dorsal intercalated segment instability (DISI) pattern may be seen on a lateral view. Unstable fractures require fixation; it is impossible to maintain reduction of an unstable fracture with cast immobilization alone.
Diagnostic considerations
When displacement occurs about the scaphoid fracture, ligamentous injury and instability should be suspected. Posttraumatic instability typically involves the proximal carpal row, which acts as a link between the distal radius and distal carpal row. This instability may be static or dynamic. With static instability, the patient is unable to position the carpal bones normally, and the abnormal alignment is readily visible on routine radiographs. With dynamic instability, the carpal alignment appears normal on radiographs, but it becomes abnormal in certain positions or with motions of the wrist.
The most common carpal instability pattern is scapholunate dissociation. It is frequently the first radiographic sign to suggest instability. However, although the scapholunate ligament may be disrupted, the scapholunate interval may be normal. A scapholunate distance of 2-3 mm or more on a routine posteroanterior (PA) view suggests elongation and possible disruption of the scapholunate ligament. A distance greater than 4 mm is considered to be diagnostic of a scapholunate ligament disruption, although this distance should be viewed in the context of the other intercarpal distances.
Recognition of carpal instability is important and helpful in treatment planning, because such instability reflects a more serious injury. Instability patterns may not be recognized on the initial radiographs and should be evaluated with every follow-up study. Intercarpal collapse may predispose the patient to nonunion and degenerative arthritis.
Radiography
The initial radiographic assessment of scaphoid fractures is performed with plain radiography. Standard views vary among institutions, but most use a minimum of 3 views: PA, true lateral, and semipronated oblique with, in many instances, ulnar deviation.
The patient with a scaphoid fracture often holds the wrist in radial deviation, thereby shortening the scaphoid and limiting its evaluation. To elongate the scaphoid, a scaphoid view is often obtained by positioning the wrist in ulnar deviation and angling the tube cranially by 20-40°. A myriad of additional views have been described for better evaluation of different areas of the scaphoid. [18, 19, 20, 21, 22]
A fracture is typically identified as a lucent line with at least one disrupted cortex. Occasionally, an opaque line is seen as a result of overriding fragments, a stress fracture, or fracture healing. Angulation of the scaphoid or separate fracture fragments may be observed. Fractures may be difficult to see; only 25% are visible on all views. The PA view allows visualization of 75% of visible fractures; the semipronated view, 77%; the lateral view, 22%; and the semisupinated view, 22%. About 2-5% of scaphoid fractures, particularly incomplete fractures along the capitate-side surface, cannot be seen on the initial image.
Evaluation of the soft tissues may aid in the radiologist's evaluation. The scaphoid, or navicular, fat stripe consists of fat that is interposed between the radial collateral ligament and the tendons of the abductor pollicis longus and the extensor pollicis brevis. It is visible in 90% of healthy individuals when the soft tissues are visualized. It may be obscured if the wrist is held in radial deviation.
Obliteration or displacement of the fat stripe usually occurs within 1 hour after the scaphoid fracture occurs. Frequently, dorsal soft-tissue swelling is present. These findings are nonspecific and can be seen with other fractures and soft-tissue injuries about the wrist. Because a normal fat stripe with a scaphoid fracture is exceedingly uncommon, a scaphoid fracture is virtually excluded when the scaphoid fat stripe is normal (see the images below).
 Images obtained in a patient who fell onto the left wrist. Initial radiograph (left) demonstrates a bulging fat stripe (arrows). A cast was applied, and the patient returned for follow-up radiography. This study included a scaphoid view (right), which better demonstrates the tubercle fracture. The injury is more prominent because of resorption about the fracture.
Images obtained in a patient who fell onto the left wrist. Initial radiograph (left) demonstrates a bulging fat stripe (arrows). A cast was applied, and the patient returned for follow-up radiography. This study included a scaphoid view (right), which better demonstrates the tubercle fracture. The injury is more prominent because of resorption about the fracture.
 Image shows a normal scaphoid fat stripe. Fat is seen to be interposed between the radial collateral ligament and the tendons of the abductor pollicis longus (APL) and the extensor pollicis brevis (EPB). An overlying vessel may sometimes obscure a portion of the fat stripe.
Image shows a normal scaphoid fat stripe. Fat is seen to be interposed between the radial collateral ligament and the tendons of the abductor pollicis longus (APL) and the extensor pollicis brevis (EPB). An overlying vessel may sometimes obscure a portion of the fat stripe.
The type and location of the scaphoid fracture may influence how conspicuous it is. Small avulsions and incomplete horizontal-oblique or distal-pole fractures are more difficult to detect than are complete transverse-oblique fractures. Fractures of the distal pole and tubercle may require special views. Technical factors also influence the detectability of scaphoid fractures. Underexposure or overexposure and patient motion limit bone detail. The film-screen combination used can greatly affect bone detail and, therefore, the visibility of subtle fractures. These factors are typically not addressed when comparative image studies are performed.
The stability of the fracture should be addressed at the initial examination, as well as at all follow-up examinations. A stable fracture is nondisplaced and does not have evidence of ligamentous instability. An unstable fracture is displaced by more than 1 mm, is angulated, or has a pattern of associated ligamentous instability. The 2 most common patterns of ligamentous instability are scapholunate dissociation and dorsal intercalated segment instability (DISI).
Although scaphoid fracture displacement and angulation can be assessed on conventional radiographs, difficulty may arise because of superimposed bone or an inability to position the patient properly. Often, displacement in the coronal plane is readily seen on conventional radiographs; however, CT scanning allows the evaluation of displacement in all planes of orientation. Three-dimensional, reformatted images also may demonstrate rotational patterns of displacement.
Angulation of the scaphoid at the fracture is often called the humpback deformity. This angulation is associated with a greater likelihood of nonunion, worse clinical outcome, and arthritis. Determination of the intrascaphoid angle can be difficult to make on conventional radiographs and is usually more easily made on a tomographic image. [23]
Amadio and colleagues used trispiral tomography scanning to determine the normal and abnormal intrascaphoid angle. [24] In their study, the tomographic scan that best displayed the scaphoid was chosen. The articular surfaces were identified, and a line was drawn to connect the extremes of the proximal and distal convex articular surfaces. A perpendicular to each line was drawn, and the resultant angle was noted. The intrascaphoid angle was evaluated in the coronal and sagittal planes.
In the Amadio et al study, [24] 10 normal wrists were studied to determine the normal range. A total of 46 scaphoids with fractures also were evaluated, and the patients were followed up for a mean period of 63 months. The normal sagittal, intrascaphoid angle was 15-34° (mean, 24° ± 5). An angle of 45° was chosen as abnormal to include most patients with poor clinical outcomes and a minimum of those with good clinical results. The coronal intrascaphoid angle was 32-46° (mean, 40° ± 4). However, the lateral intrascaphoid angle was a better clinical discriminator (see the image below)
 Images show a normal intrascaphoid angle. With a lateral radiograph, computed tomography (CT) scan, or magnetic resonance imaging (MRI) scan, the extent of the articular margin is estimated by using the curved lines. The ends of the curves at each pole are connected, and a line is drawn. Perpendicular lines from these lines are used to determine the intrascaphoid angle.
Images show a normal intrascaphoid angle. With a lateral radiograph, computed tomography (CT) scan, or magnetic resonance imaging (MRI) scan, the extent of the articular margin is estimated by using the curved lines. The ends of the curves at each pole are connected, and a line is drawn. Perpendicular lines from these lines are used to determine the intrascaphoid angle.
Amadio and coauthors [24] also developed a second method to assess the intrascaphoid angle. This method, the cortical technique, may be somewhat more reproducible because it is less dependent on the observer to define the convex articular surface. On a sagittal image, a line is drawn over the flattened volar cortex between the proximal convexity and the curve distal to the waist of the scaphoid. A second line is drawn over the dorsal flattening between the waist and the distal convexity. The lateral intrascaphoid angle with this technique is 31.9° ± 8.5. The authors suggested that an abnormal intrascaphoid angle is greater than 42°. This study did not address clinical outcome.
Although polytomography scanning was used in both of these studies, the results should be valid for conventional radiography, CT scanning, and MRI, if the landmarks are visualized.
Degree of confidence
If clinical concern persists despite normal radiographic results, the clinician has 2 main options. First, the patient's hand and wrist can be immobilized, and radiographs can be repeated after 2 weeks to detect an initially occult fracture. Second, additional imaging modalities may be used as alternatives. Radionuclide bone scintigraphy, polytomography scanning, CT scanning, and MRI have been advocated.
A linear lucency may be suggested by a prominent trabecular pattern across the waist of the scaphoid (see the image below). This pseudofracture may be particularly suspicious when it is adjacent to a small tubercle on the radial margin of the scaphoid, a normal structure that may be more prominent in some individuals. The distinguishing feature is an intact cortical margin; careful examination reveals trabeculae that traverse the lucency.
 Images show a pseudofracture. The initial radiograph of the wrist (left) demonstrates the normal fat stripe (wide arrow) with a questioned cortical disruption (thin arrow). A posteroanterior view (middle) obtained 1 week later demonstrates a similar appearance in the questioned lucency across the waist. Note that the line is not straight (arrows) and that trabeculae cross the lucency. A long-axis, oblique, sagittal computed tomography (CT) scan (right) obtained after an additional 2 weeks, with the wrist in a cast, reveals demineralization from disuse, but it does not show a fracture.
Images show a pseudofracture. The initial radiograph of the wrist (left) demonstrates the normal fat stripe (wide arrow) with a questioned cortical disruption (thin arrow). A posteroanterior view (middle) obtained 1 week later demonstrates a similar appearance in the questioned lucency across the waist. Note that the line is not straight (arrows) and that trabeculae cross the lucency. A long-axis, oblique, sagittal computed tomography (CT) scan (right) obtained after an additional 2 weeks, with the wrist in a cast, reveals demineralization from disuse, but it does not show a fracture.
Abdel-Salam and colleagues recommend the acquisition of a comparable view of the contralateral wrist if the pseudofracture line persists at the 2-week follow-up examination. [25] If the appearance is the same in both wrists, a fracture is excluded. If the appearance is different, a fracture is likely. Additional imaging with CT scanning or MRI may be used at this point. Rarely, an accessory ossicle, the os carpi centrale, can create a Mach line that overlies the waist of the scaphoid and gives the appearance of a fracture.
About 2-5% of scaphoid fractures, particularly incomplete fractures that are located along the capitate-side surface, cannot be seen on the initial image.
Computed Tomography
A section thickness of 1-2 mm is typical, whether sequence or spiral acquisition is used. A 1-mm scanning allows the production of excellent reformatted images. The oblique sagittal plane through the long axis of the scaphoid may be the preferred plane of orientation. [26, 27, 28, 29, 30, 31] When the mechanism of injury is being considered, optimal display of the volar and dorsal cortices is preferred {see the images below). Presumably, incomplete fractures may be missed on oblique coronal images. Axial imaging with reformatted images can be obtained, provided that the reformatted images are in the planes of the scaphoid and not in the anatomic planes. Edge detail is lost, and some blurring is inherent to spiral techniques, although many clinicians find them to be adequate.
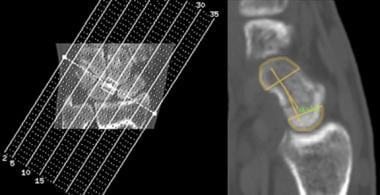
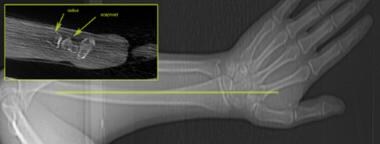 Images show positioning for direct sagittal image acquisition. Care must be taken to position the arm obliquely above the patient's head. This patient's arm was positioned horizontally, and although the beam penetrated the long axis of the scaphoid (yellow line), the beam-hardening artifact does not allow evaluation of the scaphoid (inset). Even on the most recent scanners, this can remain a problem depending on technique. Similar information loss is found if the wrist is placed on the abdomen of a large patient.
Images show positioning for direct sagittal image acquisition. Care must be taken to position the arm obliquely above the patient's head. This patient's arm was positioned horizontally, and although the beam penetrated the long axis of the scaphoid (yellow line), the beam-hardening artifact does not allow evaluation of the scaphoid (inset). Even on the most recent scanners, this can remain a problem depending on technique. Similar information loss is found if the wrist is placed on the abdomen of a large patient.
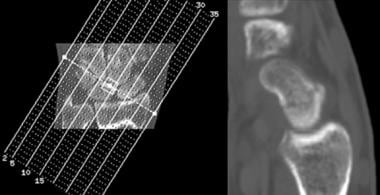 Images demonstrate the reformation of 1-mm images into a sagittal, long-axis image for improved visualization of the scaphoid. Note the nondisplaced fracture through the waist of the scaphoid.
Images demonstrate the reformation of 1-mm images into a sagittal, long-axis image for improved visualization of the scaphoid. Note the nondisplaced fracture through the waist of the scaphoid.
Several studies have demonstrated the superior ability of cone-beam CT (CBCT) compared to radiographs for the diagnosis of scaphoid fractures. [32, 33, 34] Additional advantages of CBCT are that it uses low-dose radiation and it allows the radiation-sensitive organs to be shielded because of scanner design, which can further reduce the effective dose of the examination. [34]
In a study by Snaith et al of 55 patients with a normal or equivocal radiograph who underwent subsequent cone-beam CT scanning, 9 additional radiocarpal fractures were identified that were not originally detected on radiography. [35]
In a study of 91 patients with suspected scaphoid fracture by Daniels et al, high-resolution peripheral quantitative CT (HR-pQCT) revealed a scaphoid fracture in 24 patients (26%), and conventional CT revealed a scaphoid fracture in only 15 patients (16%). [36]
Degree of confidence
CT scanning permits an accurate anatomic assessment of the fracture. Bone contusions are not evaluated with CT scanning, but true fractures can be excluded. CT scanning also allows volumetric analysis for determining the graft size that is needed to correct an angular deformity.
Pseudofractures are a plain radiographic phenomenon and are not depicted on CT scans. Occasionally, an entering vessel may cause the cortex to be incomplete. This is usually distinguished on adjacent images. As the vessel enters the bone, the walls have a thin, dense rim not found about a fracture line.
Magnetic Resonance Imaging
MRI has been suggested as an easy, quick, and perhaps cost-effective method to evaluate acute scaphoid fractures. T1-weighted images obtained in a single plane (coronal) are typically sufficient to determine the presence of a scaphoid fracture. This limited evaluation can be cost-effective, and unlike CT scanning, it does not require special positioning of the patient's hand, which may be an important consideration in the patient with a painful wrist. [37, 8, 9, 10, 11, 38, 39, 40]
The classic pattern of a fracture on an MRI scan is a linear focus of decreased signal intensity on T1-weighted images. Increased signal intensity in a distribution similar to that of the T1-weighted images is seen with T2-weighted sequences. The fracture line may be more difficult to see on T2-weighted images.
Short-tau inversion recovery (STIR) and fat-suppressed, T2-weighted sequences are very sensitive to edema. Although they are more sensitive to edema than are T1-weighted images, fractures may be overdiagnosed. A localized or diffuse region of decreased signal intensity without a discrete fracture line is consistent with the microtrauma associated with the impaction of the bone trabeculae, as found in bone bruises and contusions (see the image below).
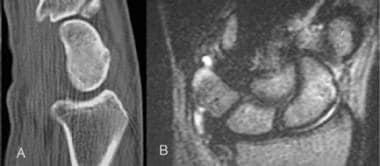 Images obtained in a patient who fell on an outstretched hand, with pain in the anatomic snuff box. The initial radiographs were normal. The representative oblique, sagittal computed tomography (CT) scan (A) does not reveal a fracture. The T2-weighted magnetic resonance imaging (MRI) scan (B) demonstrates edema without a fracture line; these findings are consistent with a contusion. T2-weighted images without fat-suppression are no longer commonly used. The edema-pattern with a short-tau inversion recovery (STIR) sequence would probably be more impressive; this finding could potentially lead to the overdiagnosis of a fracture.
Images obtained in a patient who fell on an outstretched hand, with pain in the anatomic snuff box. The initial radiographs were normal. The representative oblique, sagittal computed tomography (CT) scan (A) does not reveal a fracture. The T2-weighted magnetic resonance imaging (MRI) scan (B) demonstrates edema without a fracture line; these findings are consistent with a contusion. T2-weighted images without fat-suppression are no longer commonly used. The edema-pattern with a short-tau inversion recovery (STIR) sequence would probably be more impressive; this finding could potentially lead to the overdiagnosis of a fracture.
Gadolinium-based contrast agents have been linked to the development of nephrogenic systemic fibrosis (NSF) or nephrogenic fibrosing dermopathy (NFD). The disease has occurred in patients with moderate to end-stage renal disease after being given a gadolinium-based contrast agent to enhance MRI or magnetic resonance angiography (MRA) scans. NSF/NFD is a debilitating and sometimes fatal disease. Characteristics include red or dark patches on the skin; burning, itching, swelling, hardening, and tightening of the skin; yellow spots on the whites of the eyes; joint stiffness with trouble moving or straightening the arms, hands, legs, or feet; pain deep in the hip bones or ribs; and muscle weakness.
Degree of confidence
MRI results can lead to the overdiagnosis of scaphoid fractures. Lepisto and colleagues evaluated the use of MRI within 4 weeks of injury in 18 consecutive patients. [41] Of the 11 diagnosed fractures, the fracture line was clearly seen in only 2. The authors did not consider bone contusions as a separate entity and believed that hemorrhage and edema obliterated the actual fracture line. They offered no follow-up report for the patients examined.
In a separate study by Imaeda and colleagues, an oblique image that was obtained through the long axis of the scaphoid allowed visualization of 11 of 11 fracture lines. [42] In 10 of 11 fractures, the fracture line was visible in the coronal plane. High signal intensity, seen in the distal fragment on T2-weighted images, was characteristic of recent fractures. T1-weighted coronal images allow identification of the fracture, which is often seen on an initial coronal scout image. This suggests that limited MRI scans in only one imaging plane may cause some fractures to be missed.
Sahu et al found that in 15 out of 100 patients, MRI identified fractures that radiographs and CT did not. [37]
When edema is present, contusions may be falsely identified as fractures.
Ultrasonography
Ultrasonography is limited by the difficulties in scanning the proximal and distal thirds of the scaphoid. Nondislocated fractures are also difficult to detect. Ultrasonography can be used for position monitoring of previously identified childhood fractures, but it requires high operator expertise. [4]
To evaluate the scaphoid bone by US, a linear high-frequency probe (>12 Mhz) is required, and both the normal and the painful wrist should be observed, with the normal side observed first. The probe should be placed on the hand over the area between the scaphoid tuberosity and the radius. The scaphoid should be evaluated in the longitudinal and transverse planes from the dorsal, lateral, and palmar directions in both normal and ulnar deviation positions. [1, 43]
The most common findings are disruption of the scaphoid cortical (direct sign), hypoechoic radiocarpal fluid due to hemarthrosis, and scapho-trapezium-trapezoid effusion (indirect sign). [1]
The finding of cortical disruption has a sensitivity of 100%, a specificity of 96.5%, a postive predictive value (PPV) of 83%, and a negative predictive value (NPV) of 100%. [1]
Nuclear Imaging
Radionuclide bone scanning is typically performed 3-7 days after the initial injury if the radiographic findings are normal. Bone scan findings are considered positive for a fracture when intense, focal tracer accumulation is identified. [44] Negative bone scan results virtually exclude scaphoid fracture. Injury to other carpal bones may also be discovered with radionuclide bone scanning.
According to some studies, 25-60% of scaphoid fractures that are suspected on the basis of bone scan results are never confirmed at radiography. Most of these suspected fractures are probably bone contusions or incomplete cortical fractures. Treatment can be based on the results of bone scintigraphy, although this practice results in substantial overtreatment of patients, because most small, incomplete cortical fractures and bone contusions are likely to heal, even without treatment.
Scaphoid activity on a bone scan is not specific for a fracture, because bone contusions, degenerative disease, intraosseous ganglion, or another physiologically active process may have increased activity within the scaphoid.
As with any fracture, scintigraphic results are positive in all phases of a 3-phase bone scan. This finding helps in distinguishing chronic processes from an acute fracture.
-
A transscaphoid, perilunate dislocation is present with a fracture of the ulnar styloid. Note the typical dorsal position of the distal carpal row. The distal pole of the scaphoid maintains its relationship to the distal carpal row, while its proximal pole retains its relationship to the proximal carpal row.
-
Posteroanterior view of the wrist demonstrates a healed radius fracture and ulnar styloid. A nonunited fracture of the proximal pole of the scaphoid also is present; this was likely missed when the radius fracture was diagnosed. No sclerotic margins are present to indicate an unequivocal diagnosis of nonunion.
-
Images show delayed union of a scaphoid waist fracture. The radiograph (left) demonstrates the fracture as well as resorption around this 5-month-old fracture. T1-weighted (middle) and fat-suppressed T2-weighted (right) MRI scans demonstrate the fracture without clear evidence of synovial fluid tracking between the fragments. Eventually, this fracture healed.
-
Radiographs obtained in this patient, who has a history of scaphoid fracture, demonstrated increased opacity in the proximal pole. A computed tomography (CT) scan was obtained to evaluate healing and possible osteonecrosis. Increased density is demonstrated, but the previous fracture has completely healed. Without collapse or fragmentation, this should not be considered avascular necrosis.
-
Nonunion of the proximal-pole scaphoid fracture is demonstrated by the smooth, sclerotic margins on both sides of the fracture. Note mild arthritis at the radioscaphoid joint.
-
Avascular necrosis of the proximal pole in this chronic nonunion is evidenced by the collapse of the proximal pole. This patient does not have fragmentation at this time. Note the arthritis in the midcarpal joint consistent with a scaphoid nonunion advanced collapse (SNAC) wrist.
-
Vascular anatomy of the scaphoid. The number of perforators along the scaphoid waist is variable; therefore, among patients with a fracture in this same location, some have a better prognosis. (A) Dorsal view of the scaphoid. (B) Volar, or palmar, view of the scaphoid.
-
Lateral view of the wrist at the time of impact during a fall on an outstretched hand shows the force (arrow) applied to the scaphoid bone (red).
-
Pictures show the locations of fracture within the scaphoid bone: (A) tubercle; (B) distal pole, or extra-articular (vs intra-articular to scaphotrapezium or trapezoid joint); (C) waist; and (D) proximal pole.
-
Classification of scaphoid fracture by fracture orientation: (A) transverse, (B) oblique, and (C) vertical.
-
Images illustrate fracture stability. Nondisplaced (A) and incomplete (B) fractures are stable. Displaced fractures (C), angulated fractures (D), and associated ligamentous instability (E), such as dorsal intercalated segmental instability (DISI), are unstable.
-
Images obtained in a patient who fell onto the left wrist. Initial radiograph (left) demonstrates a bulging fat stripe (arrows). A cast was applied, and the patient returned for follow-up radiography. This study included a scaphoid view (right), which better demonstrates the tubercle fracture. The injury is more prominent because of resorption about the fracture.
-
Image shows a normal scaphoid fat stripe. Fat is seen to be interposed between the radial collateral ligament and the tendons of the abductor pollicis longus (APL) and the extensor pollicis brevis (EPB). An overlying vessel may sometimes obscure a portion of the fat stripe.
-
Images show a normal intrascaphoid angle. With a lateral radiograph, computed tomography (CT) scan, or magnetic resonance imaging (MRI) scan, the extent of the articular margin is estimated by using the curved lines. The ends of the curves at each pole are connected, and a line is drawn. Perpendicular lines from these lines are used to determine the intrascaphoid angle.
-
Images show a pseudofracture. The initial radiograph of the wrist (left) demonstrates the normal fat stripe (wide arrow) with a questioned cortical disruption (thin arrow). A posteroanterior view (middle) obtained 1 week later demonstrates a similar appearance in the questioned lucency across the waist. Note that the line is not straight (arrows) and that trabeculae cross the lucency. A long-axis, oblique, sagittal computed tomography (CT) scan (right) obtained after an additional 2 weeks, with the wrist in a cast, reveals demineralization from disuse, but it does not show a fracture.
-
Images show positioning for direct sagittal image acquisition. Care must be taken to position the arm obliquely above the patient's head. This patient's arm was positioned horizontally, and although the beam penetrated the long axis of the scaphoid (yellow line), the beam-hardening artifact does not allow evaluation of the scaphoid (inset). Even on the most recent scanners, this can remain a problem depending on technique. Similar information loss is found if the wrist is placed on the abdomen of a large patient.
-
Images demonstrate the reformation of 1-mm images into a sagittal, long-axis image for improved visualization of the scaphoid. Note the nondisplaced fracture through the waist of the scaphoid.
-
Images obtained in a patient who fell on an outstretched hand, with pain in the anatomic snuff box. The initial radiographs were normal. The representative oblique, sagittal computed tomography (CT) scan (A) does not reveal a fracture. The T2-weighted magnetic resonance imaging (MRI) scan (B) demonstrates edema without a fracture line; these findings are consistent with a contusion. T2-weighted images without fat-suppression are no longer commonly used. The edema-pattern with a short-tau inversion recovery (STIR) sequence would probably be more impressive; this finding could potentially lead to the overdiagnosis of a fracture.
-
Scaphoid waist fracture with some resorption, as seen on a posteroanterior image.









