Practice Essentials
Thoracic outlet syndromes (TOSs) are caused by compression of the neurovascular structures passing through the thoracic outlet (see the images below). Three different diagnoses can be made on the basis of the compressed structure: arterial TOS, venous TOS, and neurogenic TOS. Neurogenic TOS is by far the most common type of TOS, constituting 80-90% of all reported cases. A symptom of neurogenic TOS is Gilliatt-Sumner hand, in which there is severe wasting of the fleshy base of the thumb. Neurogenic thoracic outlet syndrome (nTOS) is responsible for approximately 95% of cases of thoracic outlet syndrome. [1, 2, 3, 4] This type of TOS is secondary to compression of the brachial plexus caused by various soft tissue and bony abnormalities at the point where the nerves pass between the anterior and middle scalene muscles. [5]
Venous TOS, which accounts for 12% of TOS cases, often presents as swelling, pain, distended veins in the upper extremity, and occasionally a bluish color of the arm. Symptoms of venous TOS often occur after a venous thrombosis of the upper extremity. [1, 2, 3, 4] Venous thoracic outlet syndrome (vTOS) results from subclavian vein compression, often between the first rib, costoclavicular ligament, and subclavius tendon within the costoclavicular space. [6] Repetitive arm movements traumatize the vein, causing posttraumatic inflammation, focal intimal fibrosis, stenosis, blood flow stasis, and eventual thrombosis leading to acute symptoms of upper extremity deep venous thrombosis. This is referred to as effort thrombosis or Paget-Schroetter syndrome and is often observed in young individuals and competitive athletes who engage in physical activities requiring repetitive arm and shoulder movements. Other terms for this condition include spontaneous thrombosis and traumatic thrombosis. [7]
Arterial TO constitutes 1-2% of cases, with ischemic manifestations such as pain, coldness, and pallor of the arm and peripheral microembolisms. [1, 2, 3, 4] Arterial thoracic outlet syndrome (aTOS) is caused by subclavian artery (SCA) compression [8] and is associated with the most serious complications, including limb ischemia (which may result in the loss of the affected upper extremity).
The American College of Radiology recommends the following imaging modalities [9] :
-
Neurogengic TOS: Chest MRI or radiography.
-
Venous TOS: Upper extremity catheter venography, US duplex Doppler, chest CT, or radiography.
-
Arterial TOS: CT angiography, MR angiography, upper extremity catheter venography, US duplex Doppler, or chest radiography.
CT and MRI are typically performed as 2-step procedures (neutral position and arm abduction) to reproduce the vascular compression seen on provocative maneuvers. CT angiography or venography provides superior analysis of the vasculature in relation to the bony structures, whereas MR angiography or venography is more efficient in the depiction of accessory muscles, muscle hypertrophy, and fibrous bands [6] . Angiography and venography remain the criterion standards for the radiologic diagnosis of these conditions, and they have the added benefit of enabling potential endovascular treatment. [9, 10, 11, 12, 13, 14, 15, 16]
The findings of the Allen maneuver, the hyperabduction maneuver, are considered positive when the radial pulse disappears during extreme abduction of the arm. This finding, however, is also present in individuals who do not have thoracic outlet syndrome and in individuals with asymptomatic cervical ribs; therefore, this finding is not diagnostic.
A positive Adson finding occurs when the radial pulse is reduced or disappears or when the blood pressure changes with the patient (1) in a sitting position, (2) holding a deep inspiration, (3) fully extending the neck, or (4) turning the head toward the ipsilateral and contralateral sides. Some investigators believe that the cause of these findings is compression by the anterior scalene muscle. A supraclavicular bruit may be audible with this maneuver, and it is believed to result from an associated subclavian stenosis.
The costoclavicular maneuver is performed when the patient assumes an exaggerated military posture and positions his or her shoulders back and downward; this positioning induces compression between the clavicle and the first rib.
(See the images of TOS below.)
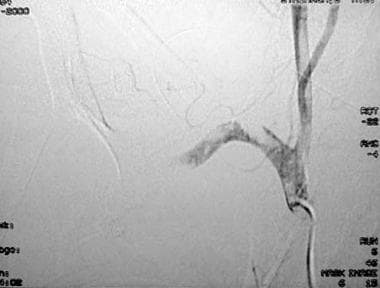
 Thoracic outlet syndrome. An angiogram in a 35-year-old woman with right arm ischemia that demonstrates right subclavian artery occlusion from the medial margin of the first rib to the axillary artery at the level of the humeral head. The patient was successfully treated with right first rib resection.
Thoracic outlet syndrome. An angiogram in a 35-year-old woman with right arm ischemia that demonstrates right subclavian artery occlusion from the medial margin of the first rib to the axillary artery at the level of the humeral head. The patient was successfully treated with right first rib resection.
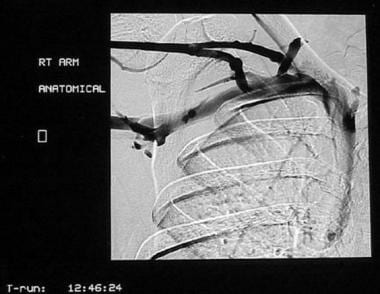
 Thoracic outlet syndrome. This venogram shows occlusion of the right subclavian vein extending to the first rib, with multiple collateral vessels.
Thoracic outlet syndrome. This venogram shows occlusion of the right subclavian vein extending to the first rib, with multiple collateral vessels.
 Thoracic outlet syndrome. A 45-year-old woman with symptoms of progressive right arm ischemia. Occlusion of the right subclavian artery near the junction between the clavicle and first rib is shown.
Thoracic outlet syndrome. A 45-year-old woman with symptoms of progressive right arm ischemia. Occlusion of the right subclavian artery near the junction between the clavicle and first rib is shown.
 Thoracic outlet syndrome. An angiogram obtained in a 45-year-old woman with progressive symptoms of right arm ischemia after 16 hours of thrombolysis that demonstrates a tight residual stenosis in the right subclavian artery. The patient presented emergently 2 days later with repeat occlusion of the right subclavian artery in the same location and was treated with surgical bypass (same patient as in the previous image).
Thoracic outlet syndrome. An angiogram obtained in a 45-year-old woman with progressive symptoms of right arm ischemia after 16 hours of thrombolysis that demonstrates a tight residual stenosis in the right subclavian artery. The patient presented emergently 2 days later with repeat occlusion of the right subclavian artery in the same location and was treated with surgical bypass (same patient as in the previous image).
Rarely, compression of a combination of structures may be responsible for the symptoms. A subset of patients with mixed neurovascular syndrome have been reported. These patients present with nTOS with coexisting arterial involvement and demonstrate better outcomes than those with nTOS only after surgical intervention, with 100% showing improvement or resolution of neurogenic symptoms postoperatively in one study. [5]
Unlike arterial and venous TOS, nTOS diagnosis is largely clinical and subjective in nature, with no definitive imaging or diagnostic studies available to confirm its presence. [5] Because no objective confirmatory test is available for TOS, there is much disagreement with regards to its true incidence. Reported figures range from 1 to 3 cases per 100,000 people. TOS is more common in women, and symptoms usually begin between ages 20 and 50. [17, 18, 1, 4, 19]
Despite considerable investigation into identifying a clinical maneuver for the accurate diagnosis of vascular thoracic outlet syndrome, no clinical test has been shown to have a consistently high degree of accuracy. The same positive findings are occasionally found in individuals without vascular thoracic outlet syndrome; therefore, the clinicians should consider a positive result at clinical examination in context with the clinical history and the results of other diagnostic tests.
Intervention
Prognosis and treatment differ for the 2 types of venous thoracic outlet syndrome.
Patients with primary venous thrombosis more commonly present with acute symptoms, including arm swelling and pain, which often limit their activity. Anticoagulant therapy reduces the extension of thrombus, as well as the associated (minute) risk of pulmonary embolism; however, multiple authors have demonstrated minimal long-term benefits of anticoagulation.
Intervention is often performed early for rapid symptomatic relief, especially in an otherwise healthy patient who requires full use of the affected arm. Catheter-directed thrombolysis and mechanical thrombectomy have significantly expanded the nonsurgical options for treatment. With surgical thoracic outlet decompression, the success rate has averaged 81%. Other advantages to catheter-directed thrombolysis include the ability to perform diagnostic venograms at the time of thrombolysis in various positions to provoke the symptoms and the ability to perform postthrombolysis venograms to document the extent of residual thrombus.
The disadvantages of thrombolysis include the risk of bleeding, which can be minimized by following prescribed dosing guidelines. Another concern is the fact that the underlying thoracic outlet compression is not addressed; therefore, a surgical procedure may still be needed later. Thrombolysis is most effective if performed within 7-10 days; at least 2 studies have shown a significant decrease in the effectiveness of thrombolysis after 10 days.
The timing of thoracic outlet decompressive surgery after thrombolysis has been a source of considerable debate in the literature. The most common approach involves a waiting period of approximately 3 weeks, during which the patient receives oral anticoagulation and the vascular endothelium is allowed to heal. Then, decompressive surgery is performed if a postthrombolysis venogram shows focal extrinsic compression. If extrinsic compression resulting from an anatomic cause is not noted on the follow-up venogram, the need for surgical intervention is less clear.
In a survey by Rutherford and Hurlbert, 86% of vascular surgeons surveyed opted for a conservative approach in this scenario, with anticoagulation therapy administered for 3-6 months, during which the patient is observed for evidence of recurrent thrombosis. If the postthrombolysis venogram reveals an intrinsic stenosis with or without extrinsic compression, percutaneous venoplasty augmented by stent placement becomes an option, although the precise role of venoplasty and stent use remains an area of considerable disagreement. [20]
Most authors do not recommend stent placement without surgical decompression because the stent itself may be compressed or become fragmented by the thoracic outlet narrowing. Dowling et al reported a case of venous thoracic outlet syndrome treated with thrombolysis, angioplasty, and stent placement without immediate first-rib resection. The case was later complicated by stent fracture. [21] Meier et al reported a series of 6 patients who underwent venous stent placements immediately after thrombolysis for venous thoracic outlet syndrome and 2 patients who underwent delayed stent procedures. Two of the 6 patients who underwent immediate stent placement did not undergo immediate surgical rib resection, and both patients had the complication of stent fracture. Long-term (1-3 yr) patency was achieved in 6 of the 8 patients. [22]
The timing of the intervention continues to be debated. Some authors recommend a phase of venous intimal healing after thrombolysis and before venoplasty or stent placement to reduce further damage to the vessel resulting in recurrent thrombosis. Other authors have proposed the use of venoplasty only after surgical resection of the first rib, when the source of the thoracic outlet compression has been removed. Molina has proposed that thrombolysis be performed first, followed by emergency surgery, for the highest likelihood of avoiding recurrent strictures and chronic symptoms. [23]
Kreienberg et al reported their outcomes that support early surgical and radiologic intervention. Twenty-three patients with venous thoracic outlet syndrome were treated with thrombolysis, followed by immediate (within 24 hr) surgical thoracic inlet decompression (including rib resection and removal of the anterior scalene muscle) and then angioplasty within 24 hours. Stents were placed to treat residual venous stenosis (>50%) in 14 patients. Of the veins treated with only angioplasty, all were patent at a mean follow-up of 4 years. Of those additionally treated with stent placement, 9 were patent at a mean follow-up of 3.5 years. No stent fractures were observed. Occluded stents were associated with longer stenoses and hypercoagulable states. From these findings, Kreienberg et al concluded that early surgical intervention followed by early radiologic intervention is safe and effective and that subclavian venous stent use is effective in short venous stenoses. [24]
If the postthrombolysis venogram demonstrates inadequate thrombolysis or residual obstruction, most vascular surgeons favor discontinuation of thrombolysis and initiation of a conservative treatment approach with anticoagulation, elevation, and support of the arm. [20, 25]
 Thoracic outlet syndrome. A venogram of a 20-year-old woman with right arm swelling that shows occlusion of the right subclavian vein as it passes through the thoracic inlet. A wire was advanced across the occlusion into the superior vena cava.
Thoracic outlet syndrome. A venogram of a 20-year-old woman with right arm swelling that shows occlusion of the right subclavian vein as it passes through the thoracic inlet. A wire was advanced across the occlusion into the superior vena cava.
 Thoracic outlet syndrome. A venogram obtained in a 20-year-old woman with right arm swelling after thrombolysis, venoplasty, and stent placement that demonstrates a patent right subclavian vein. Although venous stent placement remains controversial, this patient was doing well at 1-year follow-up (same patient as in the previous image).
Thoracic outlet syndrome. A venogram obtained in a 20-year-old woman with right arm swelling after thrombolysis, venoplasty, and stent placement that demonstrates a patent right subclavian vein. Although venous stent placement remains controversial, this patient was doing well at 1-year follow-up (same patient as in the previous image).
If the patient remains symptomatic with residual stenosis, 80% of vascular surgeons favor surgical intervention with short stenosis (66% favoring jugular vein turndown, 14% favoring claviculectomy) and 48% favor a bypass (either saphenous vein interposition or cephalic vein crossover) with long stenosis. These findings reflect the overall success of surgical intervention. [20]
Secondary venous thrombosis, often associated with central venous catheters, usually occurs with an insidious onset and minimal symptoms if any. Anticoagulation with heparin, followed with the long-term administration of warfarin, is the preferred treatment. In uncomplicated cases, thrombolysis has not had a definite benefit, and it does have significant associated complications.
In patients with a definite contraindication to anticoagulation, McCarthy et al reported success with simple conservative measures such as arm elevation and compressive dressings, and they propose reserving invasive therapies, such as thrombolysis, surgical thrombectomy, and rib resection, for patients with severe symptoms not responsive to anticoagulation. Interventional therapies, such as angioplasty and thrombolysis, are often more difficult to perform in secondary venous thrombosis because these cases are more likely to be chronic. [23, 26, 27, 28, 29, 30, 31, 25, 32, 33, 34]
Radiography
Plain images of the neck and chest with a cervical spine view or thoracic inlet view can effectively depict congenital or acquired bony anomalies that aid in the diagnosis of TOS. Cervical ribs, prominent or elongated C7 transverse processes, abnormal or elongated first ribs, and large fracture calluses are easily detected on plain radiographs.
Radiography is important if prior images are not available. Such findings may help focus subsequent, more complex and more invasive radiologic studies of a particular region. In addition, unsuspected findings such as a Pancoast tumor of the lung may be identified on these initial studies.
Although plain radiography is relatively inexpensive as a radiologic screening test, it is highly limited in its ability to depict the fine anatomic details that contribute to the symptoms of thoracic outlet syndrome. Plain radiography has a lower sensitivity for these findings than other modalities, such as CT. More definitive diagnostic imaging is usually required to establish or exclude a diagnosis of TOS.
Computed Tomography
CT is most helpful when plain radiographs show abnormal findings involving the thoracic outlet. CT scans performed both before and after intravenous administration of contrast agent and CT angiography are useful in identifying lesions (eg, cervical disks, neoplasms, bony spurs) that encroach on the structures of the thoracic outlet. Investigators have reported the use of various sophisticated protocols for spiral CT angiography. After a prospective analysis, Remy-Jardin et al concluded that reconstructed volume-rendering images have the highest sensitivity (95%) and specificity (100%), compared to cross-sectional imaging and image reconstruction with multiplanar and 3-dimensional-shaded surface display techniques. [35] In another study, Remy-Jardin et al described changes in the functional anatomy of the thoracic outlet in 79 patients with symptomatic thoracic outlet syndrome who underwent CT angiography. [36, 37, 38]
Most clinicians consider arteriography or venography to be the definitive tests for identifying vascular lesions and their associated complications. Both CT and MR angiography are relatively new and promising techniques for the vascular evaluation of the thoracic inlet that continue to evolve. [35, 36, 37, 39]
Multidetector computed tomography (MDCT) angiography
Multidetector computed tomography (MDCT) angiography can be used to diagnose aTOS that is commonly associated with the cervical ribs or an anomalous deformed first rib. Cervical ribs are found in less than 1% of the population, and only a small percentage of those patients will have symptoms of aTOS. Cervical ribs that cause symptoms are often large and can have bony fusion to the first rib that results in subclavian artery compression. [6]
The typical symptoms of aTOS are secondary to distal emboli and resultant ischemia, including claudication, pain, paresthesia, and pallor. In patients presenting with these symptoms, the imaging field of view should include runoff of the distal upper extremity arteries to assess for distal arterial emboli. Critical upper extremity ischemia is relatively uncommon because of the presence of a collateral arterial supply around the shoulder. [8]
Imaging with the patient's arms at his or her sides and raised above the head minimizes the chances of a false-negative result. Volume-rendering techniques are particularly valuable for the assessment of dynamic arterial compression, because the osseous and vascular structures can be evaluated simultaneously with excellent spatial resolution and anatomic detail. [8]
Magnetic Resonance Imaging
Multiple MR angiographic sequences and protocols can be used to obtain images of the arterial and venous anatomy of the body, including 2-dimensional (2D) and 3-dimensional (3D) time-of-flight, pulse-echo, and phase-contrast imaging. Compared to conventional angiography, MR imaging combined with MR angiography has the added advantage of enabling visualization of adjacent soft tissue abnormalities; it is particularly useful in evaluating fibromuscular causes of narrowing. Additionally, the specific application of MR angiography to the thoracic outlet has been reported. [12, 40]
Dymarkowski et al reported the use of 3D time-resolved contrast-enhanced MR angiography and T1-weighted spin-echo MR imaging for the evaluation of vascular causes of thoracic outlet syndrome. Five patients with symptoms and clinical examination findings suggestive of arterial or venous thoracic outlet syndrome were studied during ipsilateral arm adduction and hyperabduction. In all patients, 3D MR angiography during hyperabduction revealed the location of the vascular compression, while the images obtained during adduction showed normal vessel patency. The stenoses were precisely located with the maximum intensity projection images. [41]
In 3 patients in the Dymarkowski study, the results of conventional angiography performed within a 2-day interval confirmed the location. The T1-weighted images showed the anatomic etiology of the vascular compression, which was confirmed during surgery. The findings of this small study demonstrate the potential of MR angiography in the diagnosis of vascular causes of thoracic outlet syndrome. [41]
Demondion et al also described the normal MR anatomy of the thoracic outlet and its alteration with positional maneuvers by correlating the gross anatomic images with the corresponding MR images. [42]
Potential drawbacks of MR imaging include factors that may limit the image quality and the relatively time-consuming process of obtaining images. Dymarkowski et al noted that the need for a time interval between the acquisitions of the 2 series of images was a potential drawback to their approach. [41] Additional larger trials are needed to compare the accuracy of MR imaging with that of conventional angiography, as well as to confirm the clinical utility of MR angiography.
Several factors may limit the image quality of MR imaging and contribute to artifacts that reduce its sensitivity. These factors include abrupt changes in the path of a vessel, turbulent flow, changes in the direction of flow relative to the plane of imaging, and patient motion. As MR angiography continues to evolve, newer techniques may be able to overcome many of these pitfalls.
The need to study the patient in different positions (eg, in abduction or in adduction) is important for the physician performing the MR imaging study because a simple image obtained in the anatomic position may obscure unprovoked vascular compression.
Ultrasonography
Duplex ultrasound (DUS) examination is an effective initial approach to confirm a clinical suspicion of vascular TOS. Aneurysmal change, arterial stenosis, and thrombosis can be detected by DUS of the subclavian and axillary arteries. DUS has the advantage of assessing dynamic blood flow during compression maneuvers (hyperabduction), with a decrease in arterial diameter, changes in peak velocity, or reproducible symptoms considered to be diagnostic of aTOS. [6] [43, 44]
The arterial system and the venous system of both upper extremities are usually studied during duplex ultrasonography. The patient lies supine with his or her head turned to the side opposite to that being examined. The arm is initially examined in a neutral position and then at varying degrees of abduction, such as 90°, 135°, and 180°. The subclavian artery and the entire venous circulation, including the internal jugular vein, subclavian vein, axillary vein, and innominate vein (in which the portion just above the superior vena cava may not be visualized), are examined.
The criteria for hemodynamically significant venous compression include the obliteration of flow through the subclavian vein or the loss of normal cardiac pulsatility or respiratory phasicity. The criteria for hemodynamically significant arterial narrowing include a twofold or greater increase in the peak systolic velocity compared to that measured with the arm in the neutral position or the obliteration of flow. Duplex ultrasonography has been useful in the follow-up care of patients after surgical or radiologic intervention, and a baseline postprocedural examination is routinely performed. [45]
Although ultrasonography is a useful noninvasive test, the false-positive rate with the arterial criteria is 20%, and the false-positive rate with the venous criteria is 10%. Another limitation of duplex ultrasonography is the incorrect identification of a large collateral vein as the subclavian vein in subclavian vein thrombosis. Careful delineation of the entire course of the vessel and its relationship to the artery, which normally is posterior to the subclavian vein, is necessary to avoid this mistake. Another study (eg, conventional angiography) is usually performed to confirm abnormalities identified with ultrasonography and for preoperative planning.
Angiography
Arteriography
Arteriography is the most specific diagnostic examination for thoracic outlet syndrome, and it is indicated in a patient with ischemic upper extremity symptoms. The entire arterial circulation of the upper extremity is examined from the aortic arch to the distal arteries of the fingers. Access through the common femoral artery is preferred to evaluate both upper extremities, if necessary, and to evaluate various stress positions. In addition, in the presence of subclavian artery occlusion, delayed imaging after injection may be useful to demonstrate antegrade collateral circulation, with distal reconstitution of the artery beyond the point of obstruction (see the image below).
Thoracic outlet syndrome. An angiogram in a 35-year-old woman with right arm ischemia that demonstrates right subclavian artery occlusion from the medial margin of the first rib to the axillary artery at the level of the humeral head. The patient was successfully treated with right first rib resection.
Examination in a minimum of 3 positions may be required to demonstrate findings that may not be present in one position but are evident in another. In many patients, smooth extrinsic arterial narrowing is seen only on images obtained during stress.
The examination is begun with the patient in the completely adducted neutral position. Although the findings are often limited to minimal narrowing at most (or no findings are seen at all), the neutral position is best for evaluating intrinsic arterial diseases, arterial thrombosis, and poststenotic dilatation or aneurysms.
The Lang maneuver is then performed, with the arm abducted to 90° and with the patient lifting a 2-lb weight 2 cm above a tabletop. Images are obtained during deep inspiration and with the patient's head turned sharply to the opposite side. The Lang maneuver, also called the modified Allen maneuver, elicits sites of compression in the costoclavicular space, the scalene triangle, and the costocoracoid space inferior to the pectoralis minor tendon, a site of compression of the axillary artery; however, evidence of minor compression with this exaggerated stress position has also been shown in persons without thoracic outlet syndrome.
The Adson maneuver consists of depression of the patient's shoulder with his or her head turned to the symptomatic side.
Other positions for imaging include hyperabduction of the arm and the costoclavicular maneuver; the clinical examinations with these positions are equivalent (see the images below).
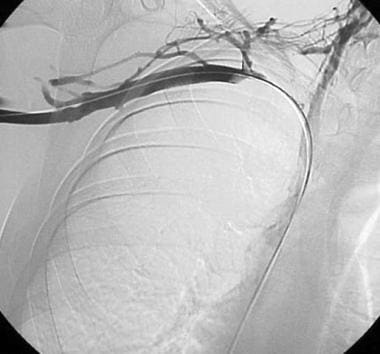
 Thoracic outlet syndrome. A venogram that was obtained in a 28-year-old man complaining of intermittent right arm swelling, taken with his right arm in the anatomic (neutral) position.
Thoracic outlet syndrome. A venogram that was obtained in a 28-year-old man complaining of intermittent right arm swelling, taken with his right arm in the anatomic (neutral) position.
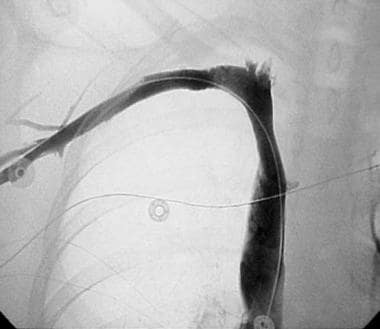
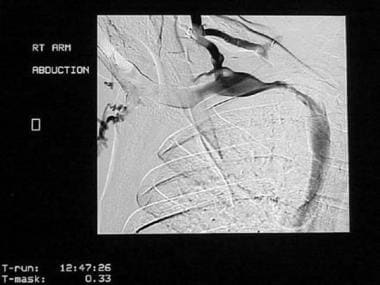 Thoracic outlet syndrome. A venogram of a 28-year-old man complaining of intermittent right arm swelling, obtained with the right arm in abduction. High-grade mid-subclavian venous stenosis in the region of the thoracic inlet is depicted (same patient as in the previous image).
Thoracic outlet syndrome. A venogram of a 28-year-old man complaining of intermittent right arm swelling, obtained with the right arm in abduction. High-grade mid-subclavian venous stenosis in the region of the thoracic inlet is depicted (same patient as in the previous image).
If technically feasible, an evaluation of the patient under conditions that produce the symptoms should be considered. These conditions may include various sitting positions with the arm abducted.
Frequently, findings are readily apparent, with severe narrowing of the subclavian artery accompanied by poststenotic dilatation or a subclavian artery aneurysm. Such findings are strong indicators of a hemodynamically significant lesion. Other findings that may indicate extrinsic compression of the subclavian artery include a ridgelike defect of the inferior margin, which indicates compression against the first rib; a similar defect combined with an impression along its superior margin, which indicates narrowing of both the scalene triangle and the costoclavicular space; or a tapered cutoff of the artery as it emerges from the scalene tunnel, which indicates compression within the scalene triangle and the scalene tunnel.
Another finding that is not accepted as a strong indicator of a hemodynamically significant lesion includes an oblique compression defect or a twist of the subclavian artery as it passes through the scalene tunnel. [46, 47]
Venography
Ascending brachial venography is the preferred and most definitive examination for diagnosing venous thrombosis. Collateral veins are more evident with venography than with ultrasonography, and therapeutic techniques, such as thrombolysis, can be readily performed if necessary. Venography is indicated in patients with definite symptoms of venous obstruction or when a duplex ultrasonography finding suggests venous abnormalities.
During the procedure, the patient's arm is placed in slight abduction to prevent artificial venous occlusion. Because the cephalic vein may lead to collateral vessels that bypass the site of thrombosis in the subclavian or axillary veins, the basilic vein is injected to ensure complete opacification around the venous thrombosis. One potential drawback of venography is that the proximal extent of the thrombus may be difficult to accurately identify.
Two major findings of upper extremity venous thrombosis are described. The first finding is a short area of obstruction at the subclavian-axillary vein junction between the first rib and the clavicle at the thoracic inlet. A variable number of adjacent collateral veins are visualized. This finding is often seen with acute obstruction. The second finding is a long area of obstruction extending distally from the axillary vein and possibly into the brachial vein. Approximately 75% of cases also involve the subclavian vein, though innominate vein involvement is rare (see the image below). Chronic and intermittent venous obstruction with or without a thrombus may be seen as an area of scarring or narrowing at the subclavian-axillary vein junction.
Thoracic outlet syndrome. This venogram shows occlusion of the right subclavian vein extending to the first rib, with multiple collateral vessels.
Angiography is also used in the preoperative care of TOS to evaluate for residual stenoses that can be managed with angioplasty or, in cases refractory to angioplasty, with stent placement. [48]
-
Thoracic outlet syndrome. An angiogram in a 35-year-old woman with right arm ischemia that demonstrates right subclavian artery occlusion from the medial margin of the first rib to the axillary artery at the level of the humeral head. The patient was successfully treated with right first rib resection.
-
Thoracic outlet syndrome. A venogram that was obtained in a 28-year-old man complaining of intermittent right arm swelling, taken with his right arm in the anatomic (neutral) position.
-
Thoracic outlet syndrome. A venogram of a 28-year-old man complaining of intermittent right arm swelling, obtained with the right arm in abduction. High-grade mid-subclavian venous stenosis in the region of the thoracic inlet is depicted (same patient as in the previous image).
-
Thoracic outlet syndrome. This venogram shows occlusion of the right subclavian vein extending to the first rib, with multiple collateral vessels.
-
Thoracic outlet syndrome. A venogram of a 20-year-old woman with right arm swelling that shows occlusion of the right subclavian vein as it passes through the thoracic inlet. A wire was advanced across the occlusion into the superior vena cava.
-
Thoracic outlet syndrome. A venogram obtained in a 20-year-old woman with right arm swelling after thrombolysis, venoplasty, and stent placement that demonstrates a patent right subclavian vein. Although venous stent placement remains controversial, this patient was doing well at 1-year follow-up (same patient as in the previous image).
-
Thoracic outlet syndrome. A 45-year-old woman with symptoms of progressive right arm ischemia. Occlusion of the right subclavian artery near the junction between the clavicle and first rib is shown.
-
Thoracic outlet syndrome. An angiogram obtained in a 45-year-old woman with progressive symptoms of right arm ischemia after 16 hours of thrombolysis that demonstrates a tight residual stenosis in the right subclavian artery. The patient presented emergently 2 days later with repeat occlusion of the right subclavian artery in the same location and was treated with surgical bypass (same patient as in the previous image).




