Practice Essentials
Testicular torsion, also termed torsion of the spermatic cord, is a relatively common and potentially devastating acute condition resulting from obstruction of the arterial blood supply to the testis. [1] Fortunately, this entity is relatively well known, and it usually occurs with enough discomfort to lead to its diagnosis and subsequent testicular salvage. However, atypical presentations of testicular torsion, delayed recognition of the condition, and its confusion with other causes of acute scrotal pain can potentially delay diagnosis and lead to testicular infarct/necrosis necessitating orchiectomy. Other diagnoses in the differential of acute scrotal pain include epidydmitis with or without orchitis, trauma, incarcerted hernia, and torsion of the appendix testis. Accurate diagnosis is imperative because testicular torsion is treated surgically, whereas epididymitis with or without orchitis is treated medically. The optimal timeframe for diagnosis of tosion for salvage of the affected testicle is within 6 hours of the onset of symptoms. Testicular torsion can occur at any age but commonly affects 1 in 4000 males 25 years old or younger. [2, 3, 4, 5, 6]
Testicular torsion can be complete, partial, or intermittent. Complete torsion occurs when the testis twists 360° or more, usually leading to absence of intratesticular blood flow that can be identified on color Doppler ultrasound examination. In partial or incomplete torsion, the spermatic cord is twisted less than 360°, allowing some residual blood perfusion to the testis. Intermittent torsion or torsion-detorsion is defined as sudden onset of unilateral testicular pain of short duration with spontaneous resolution. [7]
Diagnostic imaging, particularly Doppler ultrasonography, plays an important role in the assessment of patients with acute scrotal pain. If the history and physical examination strongly suggest testicular torsion and detorsion procedures do not work, the patient may possibly unfergo surgery without any delays to perform imaging studies. When there is a low suspicion of testicular torsion, color Doppler and power Doppler ultrasonography can be used to demonstrate arterial and venous blood flow to the testicle while providing information about scrotal anatomy and other testicular disorders. The whirlpool sign—a spiral-like pattern seen on assessment of the spermatic cord using standard high-resolution ultrasonography and/or color Doppler sonography—is a definitive sign for testicular torsion in pediatric and adult patients, but it has a limited role in neonates. Some studies suggest that MRI, particularly with contrast enhancement, is highly accurate for testicular torsion, particularly when torsion knot or whirlpool patterns are evident. Changes in the testes depend on the duration of torsion and the degree of rotation of the spermatic cord. [1, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17]
(See the images below.)
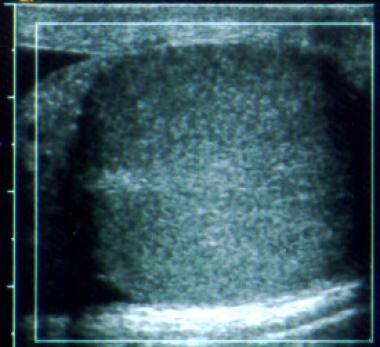
 Normal testis. Transverse color Doppler image demonstrates uniform echogenicity and flow throughout the testicle
Normal testis. Transverse color Doppler image demonstrates uniform echogenicity and flow throughout the testicle
 Normal testes. Transverse color Doppler images of both testes demonstrate symmetric echogenicity and flow.
Normal testes. Transverse color Doppler images of both testes demonstrate symmetric echogenicity and flow.
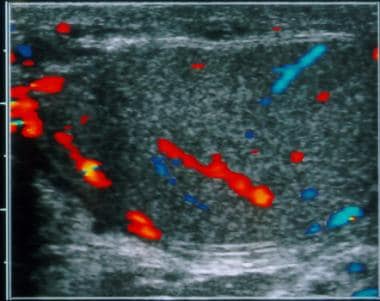
 Normal testis and epididymis. Longitudinal color Doppler image shows diffuse, normal flow to the testis and epididymis.
Normal testis and epididymis. Longitudinal color Doppler image shows diffuse, normal flow to the testis and epididymis.
 Testicular torsion. Longitudinal color Doppler image demonstrates no flow to the testicle and enlargement of the epididymis and spermatic cord, which are avascular as well.
Testicular torsion. Longitudinal color Doppler image demonstrates no flow to the testicle and enlargement of the epididymis and spermatic cord, which are avascular as well.
 Testicular torsion. Longitudinal color Doppler image of the left testicle without evident flow.
Testicular torsion. Longitudinal color Doppler image of the left testicle without evident flow.
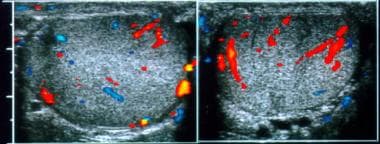
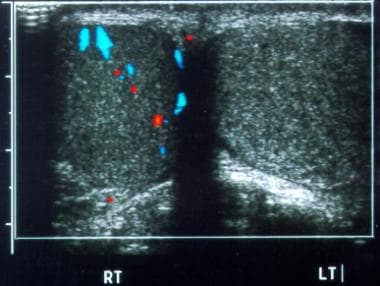 Testicular torsion. Transverse color Doppler image of both testes demonstrates enlargement, slightly decreased echogenicity, and absent flow on the left side.
Testicular torsion. Transverse color Doppler image of both testes demonstrates enlargement, slightly decreased echogenicity, and absent flow on the left side.
Preferred examination
In general, laboratory tests are not diagnostically useful in distinguishing torsion from other acute scrotal syndromes. Urinalysis results are negative in 98% of cases, and a mild leukocytosis may occur in as many as 30% of patients, which can be nonspecific.
Ultrasonography with color and power Doppler imaging has emerged as the primary imaging modality for the diagnosis of testicular torsion. [9, 10, 18, 19, 20, 21, 22] It not only helps in corroborating the diagnosis by evaluation of the testicular echotexture but also provides valuable information on vascular perfusion of the testes. In addition, sonographic findings frequently allow other diagnoses to be made in those patients presenting with acute scrotal pain who do not have torsion. [23]
Gray-scale Doppler ultrasonography is less accurate than color Doppler in assessing testicular blood flow. Early in the course of testicular torsion, gray-scale ultrasonographic examination may be normal.
Ultrasonographic findings suggestive of acute testicular torsion include the following [14, 24, 16] :
-
Absent or decreased blood flow in the affected testicle
-
Decreased flow velocity in the intratesticular arteries
-
Increased resistive indices in the intratesticular arteries
-
Hypervascularity with a low resistance flow pattern (after partial torsion-detorsion)
Color Doppler ultrasonography is highly operator dependent. In the diagnosis of testicular torsion, gray-scale findings are combined with dynamic flow information. Inaccurate results may be obtained in the prepubertal patient with small testicular volume or in cases with multiple imaging and Doppler artifacts. Such imaging artifacts may result from inappropriate gain settings and the non-use of slow-flow techniques. [7, 9, 10, 11, 13, 16, 25]
Guidelines on scrotal ultrasound examination have been published by the American College of Radiology, Society of Pediatric Radiology, Royal College of Surgeons, and Society of Radiologists in Ultrasound for both testicular and extratesticular structures. [11, 16, 26]
Before the development of high-resolution, real-time ultrasonography coupled with color Doppler, nuclear scintigraphy was the mainstay of tests available to evaluate the acute scrotum. Given associated radiation, less widespread availability, limited ancillary information, and the accuracy of color Doppler imaging, scrotal scintigraphy is no longer used as frequently. [27, 28, 29] In cases with a clinically ambiguous picture or with indeterminate sonographic findings, scintigraphy remains a viable imaging alternative. [30] Testicular scintigraphy is straightforward, although it requires intravenous access. An infiltrated radionuclide bolus can prevent an adequate examination. False-negative results are rare. False-positive results are more frequent because of the changing scintigraphic appearance of infarction over time and potential interpretation errors.
Information about the role of MRI in the diagnosis of torsion is limited, although MRI is likely to be highly sensitive. [8, 12, 16, 24, 31, 32] However, with its limited availability, the length of examination, and its cost, MRI is unlikely to become a front-line examination for the patient presenting with acute scrotal pain.
Magnetic Resonance Imaging
Some studies suggest a high degree of accuracy with MRI, particularly when it is performed with contrast enhancement. These finding are corroborated by results of controlled animal models. In addition, phosphorus-31 magnetic resonance spectroscopy can demonstrate rapidly decreasing levels of adenosine triphosphate (ATP) associated with ischemia. [8, 12, 16, 31, 32, 24]
The most sensitive MRI finding in torsion is decreased or lack of perfusion on dynamic contrast-enhanced MRI. Other characteristics include low or very low signal intensities with spotty or streaky patterns on fat-suppressed T2-weighted, heavily T2-weighted, or T2*-weighted images. The use of a combination of dynamic contrast-enhanced T1-weighted MRI with T2-weighted and T2*-weighted sequences may help distinguish patients with torsion alone from those with torsion and hemorrhagic necrosis. [8, 12, 16, 24, 31, 33, 34]
If the torsion knot or whirlpool patterns are recognized in conjunction with testicular enlargement and absent vascularity, the diagnosis is virtually certain. [15, 16, 24]
Ultrasonography
On normal gray-scale and color Doppler images, the testes are homogeneous and symmetrical in echotexture, as shown on straddle views. The testes are relatively symmetrical in size, but the normal range varies widely. On color or power Doppler ultrasonography, flow to the testes and epididymides should be symmetrical. However, flow may be difficult to visualize in young patients. In patients with torsion, gray-scale images may show testicular enlargement due to engorgement. The testicles may be uniformly hypoechoic during early tosrion or heterogeneously hypoechoic, indicating necrosis and nonviability. Echogenic areas inside the infarcted testis may represent hemorrhage. Twisting of the swollen cord, which gives the appearance of a knot (an echogenic or complex extratesticular mass) can be seen. The tunica albuginea and mediastinum may also demonstrate increased echogenicity (ie, target sign, which is more common in neonatal torsion). [7, 8, 11, 13, 14, 15, 16, 35, 36]
(See the images below.)
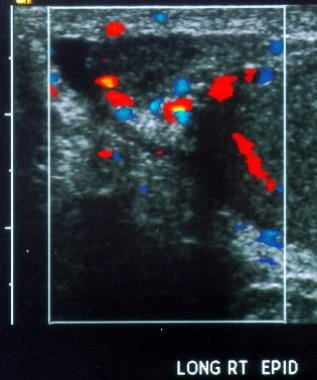
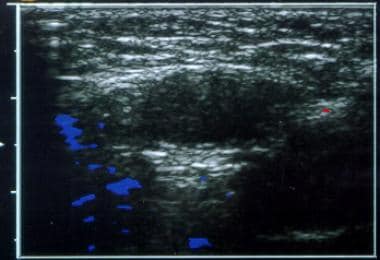 Testicular torsion. Transverse color Doppler image of the left groin illustrates an undescended testicle without flow.
Testicular torsion. Transverse color Doppler image of the left groin illustrates an undescended testicle without flow.
 Testicular torsion. Epididymitis. Longitudinal color Doppler image depicts normal vascularity of the right testicle, with increased flow in the epididymal tail and a small hydrocele.
Testicular torsion. Epididymitis. Longitudinal color Doppler image depicts normal vascularity of the right testicle, with increased flow in the epididymal tail and a small hydrocele.
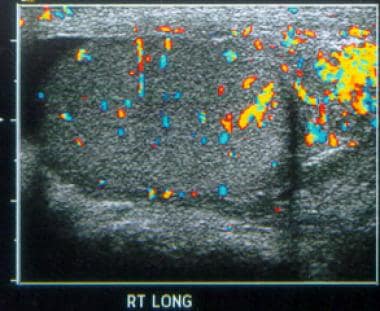
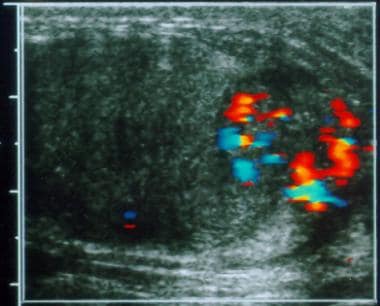
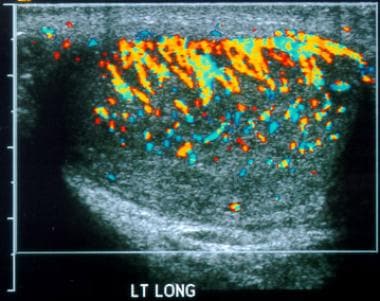 Testicular torsion. Epididymo-orchitis. Longitudinal color Doppler image of the left testis shows diffuse, markedly increased vascularity.
Testicular torsion. Epididymo-orchitis. Longitudinal color Doppler image of the left testis shows diffuse, markedly increased vascularity.
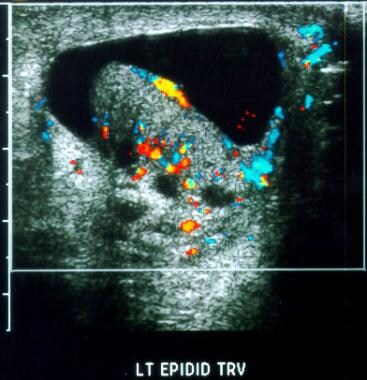 Testicular torsion. Epididymo-orchitis. Transverse color Doppler image demonstrates increased epididymal flow and a hydrocele.
Testicular torsion. Epididymo-orchitis. Transverse color Doppler image demonstrates increased epididymal flow and a hydrocele.
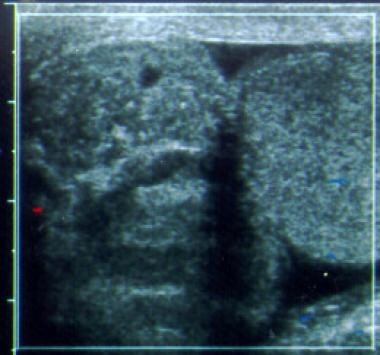
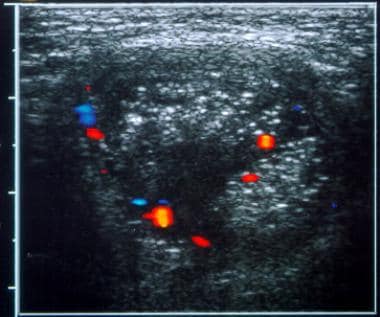 Testicular torsion. Scrotal hernia. Transverse color Doppler image of the left hemiscrotum shows heterogeneous mass superior to the testicle, with small vessels depicted.
Testicular torsion. Scrotal hernia. Transverse color Doppler image of the left hemiscrotum shows heterogeneous mass superior to the testicle, with small vessels depicted.
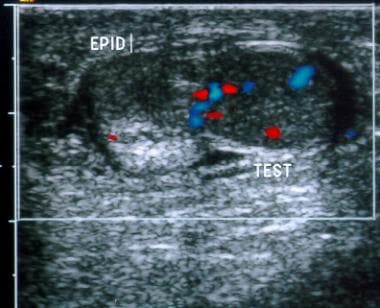 Testicular torsion. Scrotal trauma. Transverse color Doppler image demonstrates an enlarged, non-hypervascular epididymis (EPID) adjacent to the upper testicle (TEST).
Testicular torsion. Scrotal trauma. Transverse color Doppler image demonstrates an enlarged, non-hypervascular epididymis (EPID) adjacent to the upper testicle (TEST).
 Testicular torsion. Testicular tumor. Transverse color Doppler image displays a hypervascular mass in the periphery of the testis.
Testicular torsion. Testicular tumor. Transverse color Doppler image displays a hypervascular mass in the periphery of the testis.
Color and/or power Doppler imaging should be performed in all cases. Flow to the affected testicle is absent, although normal or increased flow may be seen with spontaneous torsion-detorsion. The symptomatic side should be compared with the asymptomatic side by using the straddle view obtained with optimal technical settings.
Epididymitis is visualized as an enlarged, hyperemic epididymis, usually with a heterogeneously echoic area. [37, 38] Involvement of the testis (orchitis) also produces enlargement and increased vascularity. A scrotal abscess, whether intratesticular or extratesticular, is typically seen as a complex fluid collection. Torsion of the epididymal appendage is easily recognized as a mass adjacent to the epididymal head without flow; this mass does not affect the testicular vasculature. Finally, an intratesticular hematoma may mimic a necrotic testis, but it typically has normal surrounding blood flow. An extratesticular hematoma appears as a complex, cystic collection separate from, but possibly displacing, the testis.
An absence of flow in an enlarged testicle, with flow demonstrated in the contralateral testicle, is highly specific for torsion. Power Doppler and color Doppler imaging should be used together in prepubertal boys, but it demonstrates flow in only 79-90% of normal cases. [39, 40, 41] Color Doppler and power Doppler sonography both demonstrate flow in almost 100% of postpubertal testes. [42] Color Doppler and power Doppler imaging have similar sensitivities for demonstrating flow in small testes, although the combination of the 2 techniques has a sensitivity that exceeds the sensitivity of each alone. Overall, the specificity is 77-100%, and the sensitivity is 86-100%.
In a systematic review and meta-analysis of 26 studies with 2116 patients, ultrasound examination for testicular torsion in adult patients with acute scrotal pain had an overall diagnostic sensitivity of 0.86 [95% confidence interval (CI) 0.79-0.91] and specificity of 0.95 (95% CI: 0.92-0.97). [13]
Posttorsion hyperemia may be confused with epididymo-orchitis, producing a false-negative finding. Capsular blood flow must be distinguished from intratesticular arterial flow; these observations may produce false-negative results. Although flow may be visible in one testis and is usually evident in the other, false-positive findings are possible in the young child. Technical factors (eg, erroneous flow settings, motion artifacts on power Doppler images) may produce false-positive or false-negative results.
A scrotal abscess may cause a false-positive diagnosis of torsion because of the depiction of hyperemia surrounding a fluid collection. Ultrasonography can be used to distinguish abscess from testicular torsion because of its combination of characteristic imaging and flow dynamics. [43]
Nuclear Imaging
Technetium-99m pertechnetate is the agent of choice in nuclear imaging, with an adult dose of 10-20 mCi and a pediatric dose of at least 5 mCi. Typically, immediate radionuclide angiograms are obtained, with subsequent static images as well. In the healthy patient, images show symmetric flow to the testes, and delayed images show uniformly symmetric activity.
The appearance of testicular torsion on scintigraphy depends on the chronicity. In acute torsion (usually < 7 hr), blood flow may range from normal to absent on the involved side, and a nubbin sign may be visible. The nubbin sign is a focal medial projection from the iliac artery representing reactive increased flow in the spermatic cord vessels terminating at the site of torsion. (This sign can also be seen in later stages.) Static images demonstrate a photopenic area in the involved testis. In the subacute and late phases of torsion (missed torsion), there is often increased flow to the affected hemiscrotum via the pudendal artery with a photopenic testis and a rim of surrounding increased activity on static images. This has been called a rim, doughnut, or bull's-eye sign. An abscess, tumor, or hematoma may produce false-positive findings (rim sign). A hyperemic epididymis may be misinterpreted as a halo.
Acute epididymitis generally appears as an area of focal or diffuse increased activity in the involved hemiscrotum. Testicular appendix torsion has a variable appearance: it may have a normal scan or a focal area of increased or decreased activity. An abscess, tumor, or hematoma may be indistinguishable from a torsed testicle, demonstrating a hyperemic rim surrounding an area of decreased activity.
Scintigraphy has a sensitivity of 90% and a specificity of 60% in the diagnosis of testicular torsion. Color Doppler ultrasonography has distinct advantages in diagnosing nonvascular causes of acute scrotum. Scintigraphy may be more sensitive in the neonatal period than at other times because of the difficulty in detecting flow by means of Doppler imaging. Scrotal scintigraphy may be more sensitive than color or power Doppler imaging to the presence or absence of flow in the prepubescent testicle. [23, 28, 29, 30]
-
Normal testis. Transverse color Doppler image demonstrates uniform echogenicity and flow throughout the testicle
-
Normal testes. Transverse color Doppler images of both testes demonstrate symmetric echogenicity and flow.
-
Normal testis and epididymis. Longitudinal color Doppler image shows diffuse, normal flow to the testis and epididymis.
-
Testicular torsion. Longitudinal color Doppler image demonstrates no flow to the testicle and enlargement of the epididymis and spermatic cord, which are avascular as well.
-
Testicular torsion. Longitudinal color Doppler image of the left testicle without evident flow.
-
Testicular torsion. Transverse color Doppler image of both testes demonstrates enlargement, slightly decreased echogenicity, and absent flow on the left side.
-
Transverse power Doppler image of both testes again illustrates an enlarged, avascular left testicle.
-
Testicular torsion. Transverse color Doppler image of the left groin illustrates an undescended testicle without flow.
-
Testicular torsion. Epididymitis. Longitudinal color Doppler image depicts normal vascularity of the right testicle, with increased flow in the epididymal tail and a small hydrocele.
-
Testicular torsion. Epididymo-orchitis. Longitudinal color Doppler image of the left testis shows diffuse, markedly increased vascularity.
-
Testicular torsion. Epididymo-orchitis. Transverse color Doppler image demonstrates increased epididymal flow and a hydrocele.
-
Testicular torsion. Scrotal hernia. Transverse color Doppler image of the left hemiscrotum shows heterogeneous mass superior to the testicle, with small vessels depicted.
-
Testicular torsion. Scrotal trauma. Transverse color Doppler image demonstrates an enlarged, non-hypervascular epididymis (EPID) adjacent to the upper testicle (TEST).
-
Testicular torsion. Testicular tumor. Transverse color Doppler image displays a hypervascular mass in the periphery of the testis.




