Practice Essentials
Tubular cavitation of the spinal cord, along with associated progressive neurologic symptoms, has long attracted medical interest. An accumulation of cerebrospinal fluid (CSF) may lead to simple distention of the central canal of the spinal cord; in such cases, the cavity is lined by ependymal cells (ie, hydromyelia). Alternatively, an accumulation of CSF may dissect into the surrounding white matter to form a paracentral cavity, in which case none of the cavity is lined by ependyma (ie, syringomyelia). In many, if not most, cases, both hydromyelia and syringomyelia are present (ie, syringohydromyelia). As the syringomyelic cavity expands, the initial hydromyelic cavity compresses, and the communication between the 2 cavities may atrophy and be lost. Hydromyelia and syringomyelia may be difficult to distinguish even after a detailed histologic examination. [1, 2, 3, 4, 5, 6, 7, 8]
Syringohydromyelia may be asymptomatic; clinical presentation includes paralysis, sensory loss, and chronic pain. The typical disease course is gradual neurologic deterioration over many years. [9]
For patients in whom syringomyelia is suggested by clinical criteria, the diagnosis should be confirmed by radiographic investigation. MRI can be used to classify intramedullary cavities according to anatomic and pathologic types. [4, 10]
(Characteristics of syringohydromyelia are demonstrated in the images below.)
 T1-weighted sagittal MRI scan demonstrates syringomyelia with a Chiari I malformation without hydrocephalus. The syrinx cavity does not communicate with the fourth ventricle and arises immediately caudal to the descended cerebellar tonsils.
T1-weighted sagittal MRI scan demonstrates syringomyelia with a Chiari I malformation without hydrocephalus. The syrinx cavity does not communicate with the fourth ventricle and arises immediately caudal to the descended cerebellar tonsils.
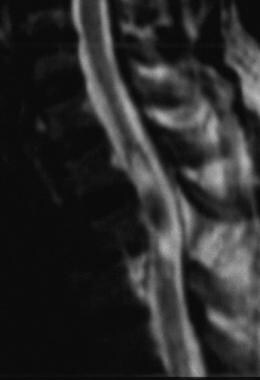
 Midsagittal T1-weighted cervical MRI scan of a young man with a posttraumatic syrinx. Note how the syrinx extends rostrally from the level of the injury. The incidence of significant syringomyelia above the spinal fracture site is approximately 3-5%. With longer survival in paraplegic and quadriplegic patients, the incidence of posttraumatic syringomyelia is likely to increase.
Midsagittal T1-weighted cervical MRI scan of a young man with a posttraumatic syrinx. Note how the syrinx extends rostrally from the level of the injury. The incidence of significant syringomyelia above the spinal fracture site is approximately 3-5%. With longer survival in paraplegic and quadriplegic patients, the incidence of posttraumatic syringomyelia is likely to increase.
Barnett et al published a classic article on the etiology of syringomyelia. [11] The authors classified syringohydromyelic cavities into 5 types:
- Communicating (with the subarachnoid space, usually at the level of the obex at the inferior aspect of the fourth ventricle)
- Posttraumatic
- Tumor-related
- Arachnoiditis-related
- Idiopathic
In a study by Milhorat et al, the intramedullary cavities were classified into communicating, noncommunicating, and atrophic types to conform to the classification of the ventricular enlargements of the brain. [12]
Overall, the etiologies of communicating hydrocephalus include subarachnoid hemorrhage, meningitis, neoplastic seeding of the leptomeninges, and idiopathic causes. A model of the communicating type may be produced by injecting sclerosing agents into the cisterna magna. Obstruction of the basilar subarachnoid cisterns results in symmetric enlargement of the CSF cavities proximal to the blockage, including all 4 cerebral ventricles and the central canal of the spinal cord. [13, 14, 10]
Noncommunicating syringes are subdivided into 6 types [10] :
- Chiari II malformation with hydrocephalus
- Chiari I malformation without hydrocephalus
- Extramedullary compressive lesions at the craniocervical junction or along the length of the spinal canal
- Spinal cord trauma
- Intramedullary tumors and intraperimedullary infections
- Multiple sclerosis
Adhesive spinal arachnoiditis may develop postoperatively or after trauma; following pyogenic, tuberculous, or luetic (syphilitic) meningitis; or after bleeding into the subarachnoid space. Atrophic syringes, which occur with myelomalacia (following trauma or infarction), are associated with a reduction in the transverse dimensions of the spinal cord. Atrophic syringes are limited to a discrete area of myelomalacia in a manner similar to the porencephalic cysts that occur in some cases of encephalomalacia.
Other associated findings include Klippel-Feil anomaly, basilar impression, scoliosis, craniovertebral fusion, and hydrocephalus. A case of idiopathic syringohydromyelia presenting with neurogenic bladder only has been reported. [15]
Radiography
For patients in whom syringomyelia is suggested by clinical criteria, the diagnosis should be confirmed by radiographic investigation.
Associated congenital anomalies include the following:
-
Basilar impression and platybasia
-
Klippel-Feil deformity
-
Atlanto-occipital fusion
-
Spina bifida (which occurs primarily at the C1 vertebra)
Scoliosis, widening of the central spinal canal, and diastematomyelia are additional associated findings.
Peripheral neuropathic joints or even neuropathic alteration of the spine itself may develop in long-standing cases of syringomyelia.
The most common abnormal radiographic musculoskeletal findings are those of joint distention in dislocation, degeneration, and frank joint destruction.
An atrophic form with resorption of the proximal humerus is described frequently in syringomyelia.
The scoliosis in this category is a progressive change that results from the cord cavitation, associated loss of anterior horn cells, and perispinal muscular imbalance, ultimately leading to scoliosis as a secondary phenomenon. Scoliosis associated with markedly destructive changes of shoulder joints should prompt a search for syringomyelia.
Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) has revolutionized the diagnosis and follow-up imaging of syringohydromyelia. Not only is the disorder more common than previously recognized, but it can now be shown to occur in association with a wide variety of congenital and acquired lesions. With the use of MRI, classifying intramedullary cavities according to anatomic and pathologic types is possible (see the images below). [3, 16, 17, 18, 19, 20, 21]
T1-weighted sagittal MRI scan demonstrates syringomyelia with a Chiari I malformation without hydrocephalus. The syrinx cavity does not communicate with the fourth ventricle and arises immediately caudal to the descended cerebellar tonsils.
 Corresponding T2-weighted cervical MRI scan of a patient with a Chiari I malformation (same patient as in the image above). Note the areas of flow void within the syrinx cavity. The flow void in the syrinx cavity is not a distinguishing characteristic of syringomyelia and may be seen in cases associated with Chiari malformations, posttraumatic syringes, and adhesive arachnoiditis. The presence of a cerebrospinal fluid flow void reflects the pulsatile movements of syrinx fluid. Such movements have been proposed as a cause of syrinx propagation, and observation of flow void may have prognostic significance.
Midsagittal T1-weighted cervical MRI scan of a young man with a posttraumatic syrinx. Note how the syrinx extends rostrally from the level of the injury. The incidence of significant syringomyelia above the spinal fracture site is approximately 3-5%. With longer survival in paraplegic and quadriplegic patients, the incidence of posttraumatic syringomyelia is likely to increase.
Corresponding T2-weighted cervical MRI scan of a patient with a Chiari I malformation (same patient as in the image above). Note the areas of flow void within the syrinx cavity. The flow void in the syrinx cavity is not a distinguishing characteristic of syringomyelia and may be seen in cases associated with Chiari malformations, posttraumatic syringes, and adhesive arachnoiditis. The presence of a cerebrospinal fluid flow void reflects the pulsatile movements of syrinx fluid. Such movements have been proposed as a cause of syrinx propagation, and observation of flow void may have prognostic significance.
Midsagittal T1-weighted cervical MRI scan of a young man with a posttraumatic syrinx. Note how the syrinx extends rostrally from the level of the injury. The incidence of significant syringomyelia above the spinal fracture site is approximately 3-5%. With longer survival in paraplegic and quadriplegic patients, the incidence of posttraumatic syringomyelia is likely to increase.
 Midsagittal T2-weighted cervical MRI scan (same patient as in the image above) demonstrates a flow void sign in the center of the posttraumatic syrinx, reflecting pulsatile fluid motion. Detection of cerebrospinal fluid (CSF) movement in a posttraumatic spinal cord lesion may alter therapy. Preoperative assessment may be made on the basis of the presence or absence of the flow void sign on T2-weighted MRI. Symptomatic posttraumatic syringes with positive flow void sign respond favorably to syrinx-subarachnoid shunting.
Midsagittal T2-weighted cervical MRI scan (same patient as in the image above) demonstrates a flow void sign in the center of the posttraumatic syrinx, reflecting pulsatile fluid motion. Detection of cerebrospinal fluid (CSF) movement in a posttraumatic spinal cord lesion may alter therapy. Preoperative assessment may be made on the basis of the presence or absence of the flow void sign on T2-weighted MRI. Symptomatic posttraumatic syringes with positive flow void sign respond favorably to syrinx-subarachnoid shunting.
 Conus ependymoma associated with syringohydromyelia. Gadolinium-enhanced sagittal MRI scan of the thoracolumbar junction demonstrates an enhancing tumor in the conus medullaris. The syrinx extends rostrally into the cervical cord (not shown). MRI studies of syringomyelia should involve the entire cord to exclude associated pathologies and should include intravenous contrast—enhanced MRI studies to exclude tumor.
Conus ependymoma associated with syringohydromyelia. Gadolinium-enhanced sagittal MRI scan of the thoracolumbar junction demonstrates an enhancing tumor in the conus medullaris. The syrinx extends rostrally into the cervical cord (not shown). MRI studies of syringomyelia should involve the entire cord to exclude associated pathologies and should include intravenous contrast—enhanced MRI studies to exclude tumor.
 Postoperative arachnoiditis with secondary syringomyelia. T1-weighted sagittal MRI scan shows L1 vertebral body wedge fracture, extensive laminectomy, and a large loculated syrinx. Deformity of the cord margins may suggest arachnoiditis. Adhesive spinal arachnoiditis may develop after trauma, infection, subarachnoid hemorrhage, and spinal surgery.
Postoperative arachnoiditis with secondary syringomyelia. T1-weighted sagittal MRI scan shows L1 vertebral body wedge fracture, extensive laminectomy, and a large loculated syrinx. Deformity of the cord margins may suggest arachnoiditis. Adhesive spinal arachnoiditis may develop after trauma, infection, subarachnoid hemorrhage, and spinal surgery.
A significant number of syringes are found in association with a variety of intraspinal lesions; the belief that an abnormality of the cervicomedullary junction is almost always present is not correct.
Most syringes do not communicate with the fourth ventricle. Even syringes that obstruct the cervicomedullary junction tend to be found at some distance below the foramen magnum and are separated from it by a syrinx-free segment of normal spinal cord. Septations within the syrinx cavity are common with more extensive lesions; however, these septa are always incomplete and do not separate one part of a syrinx cavity from another.
Syringohydromyelic cavities are frequently associated with intramedullary neoplasia. Nontumoral cysts extending into the parenchyma of the surrounding spinal cord are located at the poles of the tumors and do not enhance on intravenous (IV) contrast-enhanced MRI, whereas cysts within the substance of the tumor are considered intratumoral cysts and typically demonstrate some degree of peripheral contrast enhancement.
Many MRI findings in syringomyelia associated with adhesive spinal arachnoiditis have been described. The most striking findings include deformity of the cord at the site of adhesive arachnoiditis, poor definition of part of the syrinx wall, a fluid flow void within the syrinx cavity or cavities, and an absence of associated contrast enhancement. Meningeal thickening is a rare finding.
Posttubercular adhesive arachnoiditis is a rare, late complication of tubercular meningitis, and its association with syrinx formation is even rarer. Syringomyelia develops as a consequence of intramedullary cystic lesions and cerebrospinal fluid (CSF) flow disturbance around the spinal cord. [22, 23]
The presence of fluid flow voids in the syrinx cavity is not a differentiating characteristic of syringomyelia; flow voids may be seen in cases associated with Chiari malformations, trauma, and adhesive arachnoiditis. Most cavities associated with intramedullary tumors do not demonstrate a flow void, although rare exceptions have been reported.
The presence of fluid flow voids in syrinx cavities is common (40%); such flow voids reflect pulsatile movements of the syrinx fluid. The appearance of these flow voids may vary, depending on the imaging parameters used. As proposed by some authors, these dynamic movements may cause syrinx propagation; therefore, the observation of fluid flow voids within a syrinx cavity may have prognostic significance.
Detection of fluid movement in a posttraumatic spinal cord lesion may lead to changes in therapy. The preoperative assessment is made on the basis of the presence or absence of cyst fluid flow voids on T2-weighted MRI scans.
Quantitative measurement of oscillating CSF flow [4] in the spinal canal is possible using an optimized MRI flow-sensitive protocol, which may reveal stenosis-induced velocity changes. Phase contrast flow imaging has now emerged as the technique of choice.
Obstruction of the foramen magnum in patients with Chiari I malformation causes an abrupt systolic downward displacement of the spinal cord and impairs the recoil of CSF during diastole. These observations may have pathophysiologic implications.
Because there is an impact of Chiari I malformation–associated syringohydromyelia on morbidity and surgical intervention, its diagnosis is critical. Identifying related variables on the basis of imaging may also help identify patients at risk of syrinx formation during their course of disease. A retrospective analysis of the MR imaging studies of 108 consecutive cases of Chiari I malformation considered multiple factors associated with syrinx formation. Craniocervical junction osseous anomalies and a skull base angle of more than 135° were most predictive of syrinx formation. Patients younger than 18 years who developed syringohydromyelia were more likely to have associated skull base osseous anomalies than older individuals. [24]
Cyst fluid flow measurement is a method for direct serial monitoring of patients with syringomyelic cysts. Diastolic and systolic cyst velocities may assist in evaluating the efficacy of surgery.
Asymptomatic localized hydromyelia has been reported; it probably represents the persistence of a fetal configuration of the central canal of the spinal cord. The central canal of the spinal cord is present at birth and normally becomes progressively obliterated. Cadaver studies have shown that it may persist partially or completely. For this reason, an "incidental" syringomyelic cavity may occasionally be encountered in practice.
Gadolinium-based contrast agents have been linked to the development of nephrogenic systemic fibrosis (NSF) or nephrogenic fibrosing dermopathy (NFD). The disease has occurred in patients with moderate to end-stage renal disease after being given a gadolinium-based contrast agent to enhance MRI or MRA scans. NSF/NFD is a debilitating and sometimes fatal disease. Characteristics include red or dark patches on the skin; burning, itching, swelling, hardening, and tightening of the skin; yellow spots on the whites of the eyes; joint stiffness with trouble moving or straightening the arms, hands, legs, or feet; pain deep in the hip bones or ribs; and muscle weakness.
-
T1-weighted sagittal MRI scan demonstrates syringomyelia with a Chiari I malformation without hydrocephalus. The syrinx cavity does not communicate with the fourth ventricle and arises immediately caudal to the descended cerebellar tonsils.
-
Corresponding T2-weighted cervical MRI scan of a patient with a Chiari I malformation (same patient as in the image above). Note the areas of flow void within the syrinx cavity. The flow void in the syrinx cavity is not a distinguishing characteristic of syringomyelia and may be seen in cases associated with Chiari malformations, posttraumatic syringes, and adhesive arachnoiditis. The presence of a cerebrospinal fluid flow void reflects the pulsatile movements of syrinx fluid. Such movements have been proposed as a cause of syrinx propagation, and observation of flow void may have prognostic significance.
-
Midsagittal T1-weighted cervical MRI scan of a young man with a posttraumatic syrinx. Note how the syrinx extends rostrally from the level of the injury. The incidence of significant syringomyelia above the spinal fracture site is approximately 3-5%. With longer survival in paraplegic and quadriplegic patients, the incidence of posttraumatic syringomyelia is likely to increase.
-
Midsagittal T2-weighted cervical MRI scan (same patient as in the image above) demonstrates a flow void sign in the center of the posttraumatic syrinx, reflecting pulsatile fluid motion. Detection of cerebrospinal fluid (CSF) movement in a posttraumatic spinal cord lesion may alter therapy. Preoperative assessment may be made on the basis of the presence or absence of the flow void sign on T2-weighted MRI. Symptomatic posttraumatic syringes with positive flow void sign respond favorably to syrinx-subarachnoid shunting.
-
Conus ependymoma associated with syringohydromyelia. Gadolinium-enhanced sagittal MRI scan of the thoracolumbar junction demonstrates an enhancing tumor in the conus medullaris. The syrinx extends rostrally into the cervical cord (not shown). MRI studies of syringomyelia should involve the entire cord to exclude associated pathologies and should include intravenous contrast—enhanced MRI studies to exclude tumor.
-
Postoperative arachnoiditis with secondary syringomyelia. T1-weighted sagittal MRI scan shows L1 vertebral body wedge fracture, extensive laminectomy, and a large loculated syrinx. Deformity of the cord margins may suggest arachnoiditis. Adhesive spinal arachnoiditis may develop after trauma, infection, subarachnoid hemorrhage, and spinal surgery.



