Practice Essentials
Synovial sarcoma constitutes 8-10% of all sarcomas and usually involves the extremities (as demonstrated in the images below), especially the lower extremities around the knees. Synovial sarcoma is frequently misdiagnosed as a benign condition because of its often small size, slow growth, and well-defined appearance. This malignancy is driven by a translocation between SS18 and SSX 1, 2, or 4 (hybrid transcription factor SS18:SSX). Approximately 1,000 cases a year are diagnosed n the United States, most commonly between 15 and 30 years of age. [1, 2, 3, 4, 5]
As with all sarcomas, magnetic resonance imaging (MRI) is the modality of choice because of its excellent tissue contrast and ability to depict the lesion in multiple planes. MRI is useful for evaluating the extent of the tumor and its involvement with adjacent soft-tissue structures. For instance, MRI is helpful in the differentiation of tumor from muscle tissue and in depicting the involvement of neurovascular structures, tendons, fascial/fat planes, and bone marrow. MRI is also helpful for the differentiation of recurrent soft-tissue tumors from postsurgical or postirradiation changes. Computed tomography (CT) scanning can be used in lieu of MRI in patients who have contraindications to MRI (eg, claustrophobia, pacemakers, aneurysm clips). As with MRI, CT scanning can be useful for determining the gross anatomic extent of the tumor, and this modality is also especially useful for depicting calcifications, bone invasion, or periosteal reaction. [6, 7, 8, 9, 10, 11, 12, 13, 14]
Although MRI has proven to be valuable for the detection and staging of soft-tissue tumors, MRI signal intensity characteristics are usually nonspecific for a histologic diagnosis, with some exceptions (eg, lipomas, some liposarcomas, pigmented villonodular synovitis). Although certain signs can suggest synovial sarcoma in the differential diagnosis, MRI findings are by no means pathognomonic, and histologic analysis of the involved tissue is usually required for definitive diagnosis.
(18)F-fluorodeoxyglucose positron emission tomography (FDG-PET) is useful for risk assessment in several types of sarcomas. [15, 16] In a study by Lisle et al, (18)F-FDG-PET-derived maximum standard uptake value (SUVmax) ranged from 1.2 to 13.0 (median, 4.35). According to the study findings, pretherapy tumor SUV(max) predicted overall survival and progression-free survival. Patients who had an SUVmax greater than 4.35 were shown to have a decreased disease-free survival and were therefore at high risk for local recurrence and metastatic disease. [15]
(See the images below.)
 Lateral radiograph of the foot in a 60-year-old man who presented with a mass on the dorsum of his left foot. The radiograph shows a soft-tissue mass that is anterior to the talus and without obvious underlying bone erosion. Subtle faint calcifications are seen within the mass.
Lateral radiograph of the foot in a 60-year-old man who presented with a mass on the dorsum of his left foot. The radiograph shows a soft-tissue mass that is anterior to the talus and without obvious underlying bone erosion. Subtle faint calcifications are seen within the mass.
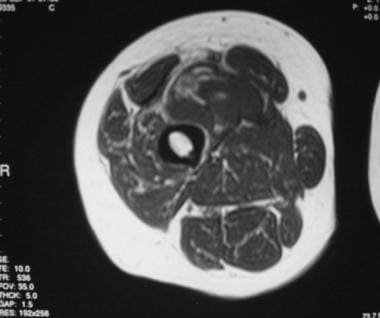 Axial T1-weighted magnetic resonance image of the thigh in a 45-year-old man who presented with a large, right midthigh mass. The anterior mass is well circumscribed, with mostly homogeneous isointensity relative to the muscle. Scattered, small, hyperintense foci probably represent hemorrhage. The fat plane between the mass and the femur is preserved.
Axial T1-weighted magnetic resonance image of the thigh in a 45-year-old man who presented with a large, right midthigh mass. The anterior mass is well circumscribed, with mostly homogeneous isointensity relative to the muscle. Scattered, small, hyperintense foci probably represent hemorrhage. The fat plane between the mass and the femur is preserved.
Synovial sarcoma tumors can appear small, especially those in the hands or head and neck regions, [17, 18, 19] where they come to medical attention earlier. Often, the small size, well-defined margins, and sometimes homogeneous appearance of synovial sarcoma can lead to misdiagnosis as a benign lesion. Berquist et al found that synovial sarcoma was the malignant soft-tissue sarcoma most frequently misdiagnosed as benign. [20] Small, superficial, solid lesions should be approached as a possible sarcoma unless strong signs prove otherwise. [2, 21]
Biopsy guidance
The choice of the imaging modality for biopsy guidance depends on the availability of the equipment, the expertise of the radiologist, and the characteristics of the lesion. CT scanning guidance is optimal for the biopsy of small lesions or those lesions that are near neurovascular bundles or other critical structures. Fluoroscopy is a real-time imaging modality that can be used for the biopsy of larger lesions that are easily seen on 2-dimensional radiographs. Ultrasonography can be used in select cases in which the lesion is more superficial and easily visible on real-time images. [21, 22, 23]
The advantages of ultrasonography over CT scanning include the following: (1) continuous real-time visualization of the needle, (2) the ability to assess regions of viable tissue by using color-flow Doppler imaging, (3) the lack of ionizing radiation, (4) the availability of ultrasound scanners, (5) the reduced procedural time, and (6) overall cost-effectiveness. In some cases in which the tumor is not easily seen on CT scans or in which visualization of the tumor in several planes is desired, MRI-guided biopsy can be performed. [21, 22, 23]
Radiography
Radiography is often the initial study obtained for the evaluation of synovial sarcoma. In 50% of patients with synovial sarcoma, radiographic findings are interpreted as normal (as potentially could occur with the image below). If an abnormality is present, the radiograph may reveal a well-defined, round or lobulated soft-tissue mass that averages approximately 8 cm in its largest dimension. [6]
 Lateral radiograph of the femur in a 45-year-old man who presented with a large, right midthigh mass. This radiograph is remarkable only for a subtle soft-tissue prominence on the anterior aspect of the thigh. No calcifications are depicted.
Lateral radiograph of the femur in a 45-year-old man who presented with a large, right midthigh mass. This radiograph is remarkable only for a subtle soft-tissue prominence on the anterior aspect of the thigh. No calcifications are depicted.
Approximately 30% of patients have calcifications that are detectable radiographically (as in the images below). The calcifications may be focal or spread throughout most of the tumor, and they may appear fine, stippled, or opaque.
Lateral radiograph of the foot in a 60-year-old man who presented with a mass on the dorsum of his left foot. The radiograph shows a soft-tissue mass that is anterior to the talus and without obvious underlying bone erosion. Subtle faint calcifications are seen within the mass.
 Anteroposterior radiograph of the hip in a patient who presented with a mass in the region of the left hip. Opaque, masslike calcifications overlying the femoral neck and inferior pubic ramus are seen.
Anteroposterior radiograph of the hip in a patient who presented with a mass in the region of the left hip. Opaque, masslike calcifications overlying the femoral neck and inferior pubic ramus are seen.
Uncommonly, tumors can erode bone. Adjacent periosteal reaction can be seen in as many as 20% of patients. Distant metastases to bone are usually of the lytic and/or mixed variety.
When the neoplasm is near a joint and causes limitation of movement, periarticular osteoporosis may be seen.
Computed Tomography
CT scan findings are nonspecific and usually demonstrate a single round or lobulated mass with a soft-tissue density. The lesions measure approximately 3-12 cm in their largest dimension and are usually found near a joint. Masses in the head and neck or distal extremities are smaller at presentation, presumably secondary to an early mass effect.
The mass is usually well defined (as in the CT scans below) but can occasionally appear infiltrative and can be homogeneous and show homogeneous enhancement, particularly in smaller lesions; alternatively, if hemorrhage or necrosis has occurred, the lesion may be multiloculated and show heterogeneous enhancement. [18, 24, 9]
 Computed tomography scan through the right thigh. This image demonstrates a round, noncalcified, well-circumscribed mass that displaces, rather than invades, the surrounding muscles. The mass appears to be separate from the bone.
Computed tomography scan through the right thigh. This image demonstrates a round, noncalcified, well-circumscribed mass that displaces, rather than invades, the surrounding muscles. The mass appears to be separate from the bone.
 Computed tomography scan of the thigh in a 45-year-old man who presented with a large, right midthigh mass. A well-defined mass is seen on the anterior aspect of the thigh and appears to be mostly isodense relative to the muscle, with curvilinear areas of slightly increased density. The mass appears apposed to the underlying bone.
Computed tomography scan of the thigh in a 45-year-old man who presented with a large, right midthigh mass. A well-defined mass is seen on the anterior aspect of the thigh and appears to be mostly isodense relative to the muscle, with curvilinear areas of slightly increased density. The mass appears apposed to the underlying bone.
Calcifications are demonstrated in 30% of patients [1] ; typically, diffuse punctate calcifications are revealed. These are often more concentrated at the periphery than at the center. Extensive calcifications can be similar in appearance to osteosarcoma or a calcified chondroid lesion. Densely calcified lesions, when found near a joint, may simulate tumoral calcinosis. Areas of calcification are seen in the image below.
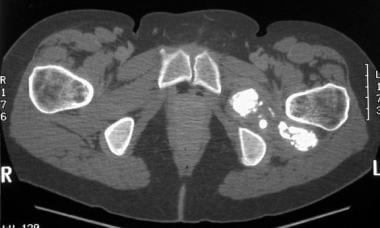 Computed tomography scan of the hip in a patient who presented with a mass in the region of the left hip. The scan was obtained through the mass and demonstrates masslike areas of calcification within the muscle density in the region of the left obturator externus muscle.
Computed tomography scan of the hip in a patient who presented with a mass in the region of the left hip. The scan was obtained through the mass and demonstrates masslike areas of calcification within the muscle density in the region of the left obturator externus muscle.
Involvement of the adjacent bone can cause changes, including cortical invasion with a wide zone of transition, bone remodeling from pressure erosion, and/or adjacent periosteal reaction.
Magnetic Resonance Imaging
Synovial sarcoma tumors tend to be large, averaging approximately 8 cm in their largest dimension, which is usually parallel to the long axis of the body. Approximately 91% of patients have a well-defined, ovoid lesion with rounded or gently lobulated margins (see the image below). [24] The effect on adjacent structures is usually displacement, rather than invasion or destruction. [9]
Axial T1-weighted magnetic resonance image of the thigh in a 45-year-old man who presented with a large, right midthigh mass. The anterior mass is well circumscribed, with mostly homogeneous isointensity relative to the muscle. Scattered, small, hyperintense foci probably represent hemorrhage. The fat plane between the mass and the femur is preserved.
Most tumors display a heterogeneous intermediate signal intensity on T1-weighted MRIs. Lesions smaller than 5 cm are more likely to have a predominantly homogeneous signal intensity that is similar to that of the adjacent muscle (as in the above image). Larger lesions are most often heterogeneous secondary to extensive areas of hemorrhage and necrosis, a characteristic seen in the image below.
 Sagittal T1-weighted magnetic resonance image of the thigh in a patient with a mass in the anterior left upper thigh and/or inguinal region. The image shows large areas of hemorrhage and necrosis, with intermediate signal intensity on a background of a muscle-intensity mass.
Sagittal T1-weighted magnetic resonance image of the thigh in a patient with a mass in the anterior left upper thigh and/or inguinal region. The image shows large areas of hemorrhage and necrosis, with intermediate signal intensity on a background of a muscle-intensity mass.
On T2-weighted images, lesions are usually hyperintense, with a signal intensity similar to or higher than that of fatty tissue (as in the first image below). Considerable inhomogeneity is demonstrated in 82% of lesions, with cystic components seen in 77% (as demonstrated in the second and third images below). Cystic components with striking fluid-fluid levels are demonstrated in 18% of tumors. [24]
 Sagittal T2-weighted magnetic resonance image of the foot in a 60-year-old man who presented with a mass on the dorsum of his left foot. The mass shows predominantly high signal intensity that is hyperintense relative to fat. Scattered areas of hypointensity probably represent calcifications.
Sagittal T2-weighted magnetic resonance image of the foot in a 60-year-old man who presented with a mass on the dorsum of his left foot. The mass shows predominantly high signal intensity that is hyperintense relative to fat. Scattered areas of hypointensity probably represent calcifications.
 Coronal T2-weighted magnetic resonance image of the thigh in a 45-year-old man who presented with a large midthigh mass on the right. On this T2-weighted image, the mass has become markedly heterogeneous, with high signal intensity depicting cystic regions of hemorrhage and necrosis. Note that portions of the mass are hyperintense relative to the subcutaneous fat. The location of the mass is somewhat atypical because it is centered at the level of the midshaft rather than near a joint.
Coronal T2-weighted magnetic resonance image of the thigh in a 45-year-old man who presented with a large midthigh mass on the right. On this T2-weighted image, the mass has become markedly heterogeneous, with high signal intensity depicting cystic regions of hemorrhage and necrosis. Note that portions of the mass are hyperintense relative to the subcutaneous fat. The location of the mass is somewhat atypical because it is centered at the level of the midshaft rather than near a joint.
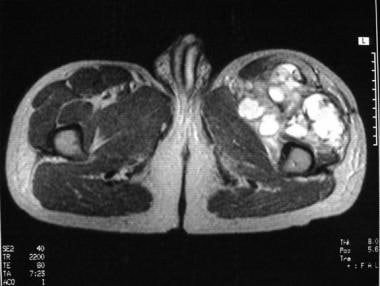 Axial T2-weighted magnetic resonance image of the hip in a patient with a mass in the anterior left upper thigh and/or inguinal region. The mass is inseparable from the underlying femoral cortex and contains strikingly hyperintense cystic areas with irregular septa of intermediate signal intensity.
Axial T2-weighted magnetic resonance image of the hip in a patient with a mass in the anterior left upper thigh and/or inguinal region. The mass is inseparable from the underlying femoral cortex and contains strikingly hyperintense cystic areas with irregular septa of intermediate signal intensity.
Approximately one third of lesions demonstrate the "triple signal pattern" on T2-weighted images; this pattern consists of a combination of (1) hyperintense fluid within cystic components, with or without fluid levels, (2) intermediate signal tissue similar in intensity to that of muscle, and (3) slightly hypointense tissue similar in intensity to that of fibrous tissue.
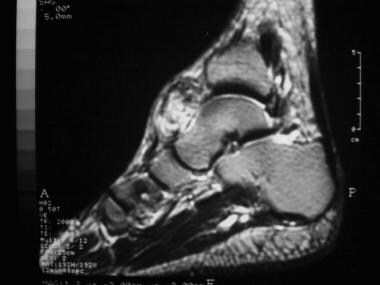
Apposition to bone surfaces without a clear plane of separation is seen in 50-59% of cases, with clear bone erosion (as seen in the superior talus in the image below) or destruction in 22%. Calcifications are not easily seen on MRIs and, when visible, are usually hypointense on all sequences.
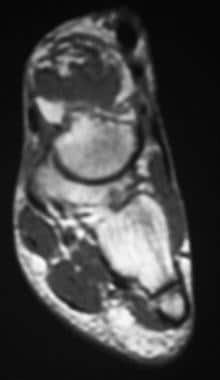 Coronal T1-weighted magnetic resonance image of the foot in a 60-year-old man who presented with a mass on the dorsum of his left foot. A rounded, soft-tissue mass is seen eroding the cortex of the superior talus. The mass is predominantly isointense relative to the muscle, with scattered areas of hyperintensity that are consistent with hemorrhage.
Coronal T1-weighted magnetic resonance image of the foot in a 60-year-old man who presented with a mass on the dorsum of his left foot. A rounded, soft-tissue mass is seen eroding the cortex of the superior talus. The mass is predominantly isointense relative to the muscle, with scattered areas of hyperintensity that are consistent with hemorrhage.
The use of gadolinium-based contrast agents has a limited value in the evaluation of synovial sarcomas. On dynamic imaging, malignant soft-tissue masses have been shown to enhance earlier, faster, and more predominantly peripherally than benign lesions. [25] These findings are believed to be secondary to the effects of tumor angiogenesis. Synovial sarcomas usually demonstrate heterogeneous contrast enhancement, with early enhancement of tumor within 7 seconds of arterial enhancement. [25]
Gadolinium-based agents may be helpful in posttreatment MRIs, in which mild, diffuse, nonfocal contrast enhancement is a typical finding. With recurrent disease, focal nodules with homogeneous enhancement and high signal intensity without cystic components are typically seen on T2-weighted images.
Gadolinium-based contrast agents have been linked to the development of nephrogenic systemic fibrosis (NSF) or nephrogenic fibrosing dermopathy (NFD). For more information, see the eMedicine topic Nephrogenic Systemic Fibrosis. The disease has occurred in patients with moderate to end-stage renal disease after being given a gadolinium-based contrast agent to enhance MRI or MRA scans. NSF/NFD is a debilitating and sometimes fatal disease. Characteristics include red or dark patches on the skin; burning, itching, swelling, hardening, and tightening of the skin; yellow spots on the whites of the eyes; joint stiffness with trouble moving or straightening the arms, hands, legs, or feet; pain deep in the hip bones or ribs; and muscle weakness. For more information, see Medscape.
Ultrasonography
Ultrasonography does not play a significant role in the evaluation of synovial sarcomas. The imaging characteristics cannot be used to establish a precise diagnosis. Grossly, sonograms can provide information regarding the size and consistency of a soft-tissue mass (eg, differentiating cystic from solid masses or a localized mass from diffuse edema). Most commonly, a well-circumscribed, heterogeneous mass, with or without cystic components, is seen.
Ultrasonography can be useful as a real-time imaging technique for guiding diagnostic needle biopsy, especially in large heterogeneous tumors. Color-flow Doppler ultrasonography reveals blood flow in solid soft-tissue masses. [26] Studies have shown that findings in color-flow Doppler ultrasonography are not specific for differentiating benign from malignant tumors; however, the technique may be useful for monitoring the regression of tumor neovascularity after the administration of chemotherapy or irradiation.
Nuclear Imaging
(18)F-fluorodeoxyglucose positron emission tomography (FDG-PET) is useful for risk assessment in several types of sarcomas. In a study by Lisle et al, (18)F-FDG-PET-derived maximum standard uptake value (SUVmax) ranged from 1.2 to 13.0 (median, 4.35). According to the study findings, pretherapy tumor SUV(max) predicted overall survival and progression-free survival. Patients who had an SUVmax greater than 4.35 were shown to have a decreased disease-free survival and were therefore at high risk for local recurrence and metastatic disease. [15]
In a retrospective study of 212 patients (160 patients with soft-tissue sarcomas, 52 patients with osseous sarcomas), Charest et al evaluated, on the basis of fluorodeoxyglucose (FDG) avidity, the sensitivity of FDG positron emission tomography/CT (PET/CT) scanning for the detection of soft-tissue and osseous sarcomas. Among the study's results, the authors determined that FDG-PET/CT scanning had a sensitivity of 80% for synovial sarcomas. [27]
Angiography
Angiography does not play a significant role in the evaluation of synovial sarcoma. Angiography allows the gross evaluation of the tumor's size and vascularity. The tumor appears as a soft-tissue mass with a fine network of tumor vessels and an inhomogeneous capillary blush. The degree of vascularity may vary according to the histopathology.
One study reported that monophasic tumors of synovial sarcoma demonstrate a higher degree of neovascularity than do biphasic tumors. [28]
Questions & Answers
Overview
What is the role of imaging in the diagnosis of synovial sarcoma?
Why are synovial sarcomas the most frequently misdiagnosed soft-tissue carcinoma?
Which imaging modalities should be used to guide biopsy of suspected synovial sarcoma?
Which radiology findings are characteristic of synovial sarcoma?
Which CT findings are characteristic of synovial sarcoma?
Which MRI findings are characteristic of synovial sarcoma?
What is the role of gadolinium-based contrast agents in synovial sarcoma imaging?
What is the role of ultrasonography in the diagnosis of synovial sarcoma?
What is the role of nuclear imaging in the diagnosis of synovial sarcoma?
What is the role of angiography in the diagnosis of synovial sarcoma?
-
Lateral radiograph of the foot in a 60-year-old man who presented with a mass on the dorsum of his left foot. The radiograph shows a soft-tissue mass that is anterior to the talus and without obvious underlying bone erosion. Subtle faint calcifications are seen within the mass.
-
Coronal T1-weighted magnetic resonance image of the foot in a 60-year-old man who presented with a mass on the dorsum of his left foot. A rounded, soft-tissue mass is seen eroding the cortex of the superior talus. The mass is predominantly isointense relative to the muscle, with scattered areas of hyperintensity that are consistent with hemorrhage.
-
Sagittal T2-weighted magnetic resonance image of the foot in a 60-year-old man who presented with a mass on the dorsum of his left foot. The mass shows predominantly high signal intensity that is hyperintense relative to fat. Scattered areas of hypointensity probably represent calcifications.
-
Anteroposterior radiograph of the hip in a patient who presented with a mass in the region of the left hip. Opaque, masslike calcifications overlying the femoral neck and inferior pubic ramus are seen.
-
Computed tomography scan of the hip in a patient who presented with a mass in the region of the left hip. The scan was obtained through the mass and demonstrates masslike areas of calcification within the muscle density in the region of the left obturator externus muscle.
-
Computed tomography scan through the right thigh. This image demonstrates a round, noncalcified, well-circumscribed mass that displaces, rather than invades, the surrounding muscles. The mass appears to be separate from the bone.
-
Lateral radiograph of the femur in a 45-year-old man who presented with a large, right midthigh mass. This radiograph is remarkable only for a subtle soft-tissue prominence on the anterior aspect of the thigh. No calcifications are depicted.
-
Computed tomography scan of the thigh in a 45-year-old man who presented with a large, right midthigh mass. A well-defined mass is seen on the anterior aspect of the thigh and appears to be mostly isodense relative to the muscle, with curvilinear areas of slightly increased density. The mass appears apposed to the underlying bone.
-
Axial T1-weighted magnetic resonance image of the thigh in a 45-year-old man who presented with a large, right midthigh mass. The anterior mass is well circumscribed, with mostly homogeneous isointensity relative to the muscle. Scattered, small, hyperintense foci probably represent hemorrhage. The fat plane between the mass and the femur is preserved.
-
Coronal T2-weighted magnetic resonance image of the thigh in a 45-year-old man who presented with a large midthigh mass on the right. On this T2-weighted image, the mass has become markedly heterogeneous, with high signal intensity depicting cystic regions of hemorrhage and necrosis. Note that portions of the mass are hyperintense relative to the subcutaneous fat. The location of the mass is somewhat atypical because it is centered at the level of the midshaft rather than near a joint.
-
Sagittal T1-weighted magnetic resonance image of the thigh in a patient with a mass in the anterior left upper thigh and/or inguinal region. The image shows large areas of hemorrhage and necrosis, with intermediate signal intensity on a background of a muscle-intensity mass.
-
Axial T2-weighted magnetic resonance image of the hip in a patient with a mass in the anterior left upper thigh and/or inguinal region. The mass is inseparable from the underlying femoral cortex and contains strikingly hyperintense cystic areas with irregular septa of intermediate signal intensity.






