Practice Essentials
A volvulus is a twisting of the intestine around its blood supply axis. In sigmoid volvulus, the twist occurs at the base of the sigmoid mesentery. This condition most commonly presents in patients who are less mobile; who are bedbound and institutionalized; and who usually have a history of chronic constipation. [1, 2, 3, 4, 5] Sigmoid volvulus is the most common form of volvulus of the gastrointestinal tract; it is responsible for 8% of all intestinal obstructions. Sigmoid volvulus is particularly common in elderly persons. However, sigmoid volvulus can occur at any age, with case reports in infants and children, as well as in otherwise healthy teenagers and younger adults. [6, 7] Patients present with abdominal pain, distention, and absolute constipation. [8] Predisposing factors to sigmoid volvulus include chronic constipation, megacolon, and an excessively mobile colon. Plain abdominal radiographic findings are usually diagnostic.
(See the images below.)
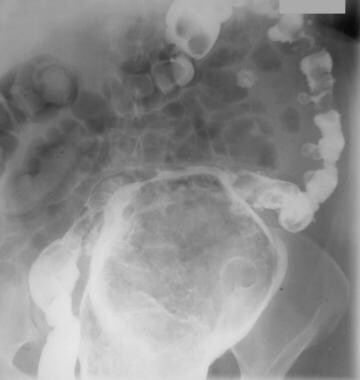
 This radiograph demonstrates a greatly dilated sigmoid that almost fills the entire abdomen. Note the coffee bean sign. The remainder of the large bowel is not dilated, presumably because the proximal point of the twist is not causing obstruction and thus allows drainage into the sigmoid.
This radiograph demonstrates a greatly dilated sigmoid that almost fills the entire abdomen. Note the coffee bean sign. The remainder of the large bowel is not dilated, presumably because the proximal point of the twist is not causing obstruction and thus allows drainage into the sigmoid.
 Erect abdominal radiograph. This image shows fluid levels in the distended sigmoid loop.
Erect abdominal radiograph. This image shows fluid levels in the distended sigmoid loop.
Decompression may be achieved with the introduction of a stiff tube per the rectum, aided by endoscopy or fluoroscopy. The mortality rates associated with sigmoid volvulus are 20-25%, depending on the interval between the time that the diagnosis is made and the time that treatment is rendered. Therefore, early radiographic recognition of sigmoid volvulus is important. [8, 9, 10, 11, 12, 13]
(See the image below.)
 This radiograph shows decompression of the sigmoid loop following retrograde passage of a flatus tube.
This radiograph shows decompression of the sigmoid loop following retrograde passage of a flatus tube.
Imaging modalities
The key radiologic features of sigmoid volvulus are those of a double-loop obstruction, which has been reported in approximately 50% of patients. The key finding consists of a dilated loop of pelvic colon, associated with features of small-bowel obstruction and retention of feces in an undistended proximal colon. The dilated loop usually lies in the right side of the abdomen, and the limbs taper inferiorly into the right lower quadrant. Medial deviation of the distal descending colon is a rare but highly specific finding.
Plain abdominal radiographic findings are usually diagnostic of sigmoid volvulus. Decompression may be achieved by the introduction of a stiff tube per rectum, aided by endoscopy or fluoroscopy. A single-contrast barium enema examination is usually adequate if it is required, as in cases when the diagnosis is in doubt.
Computed tomography (CT) scanning is the least invasive imaging technique that allows assessment of mural ischemia. Unlike barium enema examination, CT scanning has a high likelihood of revealing other causes of abdominal pain if the source of the patient's symptoms is not sigmoid volvulus. The American Society for Gastrointestinal Endoscopy has recommended contrast-enhanced CT as the preferred diagnostic study because of its high sensitivity and specificity. [14]
The coffee-bean sign (also known as the kidney bean sign) is a distended sigmoid loop with an inverted U shape. The whirl, or whirlpool, sign is seen when the bowel rotates around its mesentery, leading to whirls of the mesenteric vessels. [15, 16]
Ishibashi et al retrospectively analyzed 66 patients diagnosed with sigmoid volvulus and proposed a new predictive classification system for sigmoid volvulus based on radiographic findings, classifying patients according to the coffee-bean sign mesenteric axis (AXIS classification: group A, 0-90°; group B, 90-135°; and group C, >135°). The researchers found that patients in group C had a significantly higher frequency of severe sigmoid volvulus (100%) compared to group B (30%) and group A (15%). Overall, AXIS classification was found to be significantly associated with severe sigmoid volvulus, intestinal necrosis, and need for surgery, but not with length of stay or 30-day mortality. [16]
In a study by Kusunoki et al of 30 patients with sigmoid volvulus, the researchers found that initial CT findings of a long and distended sigmoid colon are risk factors for recurrence. Extension findings (ie, sigmoid colon extending to the diaphragm or ventral to the liver) were significantly more frequent in the recurrent group (77.3%) than in the nonrecurrent group (25.0%). In addition, the diameter of distended sigmoid colon was significantly larger in the recurrent group (11.7 ± 3.8 cm) than in the nonrecurrent group (7.1 ± 1.1 cm). [17]
Results of conventional mesenteric angiography with intravenously administered contrast material or magnetic resonance angiography (MRA) may be more definitive in the diagnosis of mesenteric ischemia. [18, 19, 20, 21]
Plain radiographs readily permit the distinction of sigmoid volvulus from primary volvulus of the small intestine and from other nonobstructive surgical emergencies. However, volvulus of the right colon, closed-loop small intestinal obstruction, and sigmoid volvulus complicated by peritonitis may simulate sigmoid volvulus on radiographs. Sigmoidoscopy, rather than barium enema examination, is the procedure of choice if an ileosigmoid knot is suspected.
Diagnostic difficulties may occur with plain abdominal radiographs if the degree of proximal dilatation is so marked that the sigmoid loop may not be recognized as such. Similar difficulties may be encountered when a large amount of fluid is associated with a small amount of air. This situation causes poor definition of the sigmoid colon on a supine radiograph, and the high air-fluid levels demonstrated on erect images may be inadequate to define the sigmoid loop accurately.
Barium enema examination is contraindicated in patients in whom a gangrenous bowel is suspected or when a pneumoperitoneum is noted on a plain abdominal radiograph or erect chest radiograph. Barium enema examination is also contraindicated in patients who have clinical signs of peritonitis.
Ultrasonography might occasionally be useful in assessing large-bowel obstruction. [22, 23] However, the confidence level for ultrasonography in the diagnosis of sigmoid volvulus is low. In the limited experience in diagnosing sigmoid volvulus by ultrasonography, the images fail to depict the cause in most patients. [19]
Radiography
Plain radiographs show a markedly distended sigmoid loop, which assumes a bent inner tube or inverted U -shaped appearance, with the limbs of the sigmoid loop directed toward the pelvis. [24]
The colonic haustra are lost, and progressive distention elevates the sigmoid loop under one side of the diaphragm. An upright radiograph shows a greatly distended sigmoid loop with air-fluid levels mainly on the left side of the abdomen and extending toward the right hemidiaphragm.
The involved bowel walls are edematous, and the contiguous walls form a dense white line on radiographs. This line is surrounded by the curved and dilated gas-filled lumen, resulting in a coffee bean-shaped structure; this is the coffee bean sign. [25, 15, 16] If more fluid than air is in the obstructed loop of the sigmoid, the volvulus may be demonstrable by a soft-tissue mass or a pseudotumor sign. A dilated sigmoid colon that ascends to the transverse colon (northern exposure sign) is said to be a reliable sign of a sigmoid volvulus on a supine abdominal radiograph. [26]
Ishibashi et al retrospectively analyzed 66 patients diagnosed with sigmoid volvulus and proposed a new predictive classification system for sigmoid volvulus based on radiographic findings, classifying patients according to the coffee-bean sign mesenteric axis (AXIS classification: group A, 0-90°; group B, 90-135°; and group C, >135°). The researchers found that patients in group C had a significantly higher frequency of severe sigmoid volvulus (100%) compared to group B (30%) and group A (15%). Overall, AXIS classification was found to be significantly associated with severe sigmoid volvulus, intestinal necrosis, and need for surgery, but not with length of stay or 30-day mortality. [16]
(See the images below.)
This radiograph demonstrates a greatly dilated sigmoid that almost fills the entire abdomen. Note the coffee bean sign. The remainder of the large bowel is not dilated, presumably because the proximal point of the twist is not causing obstruction and thus allows drainage into the sigmoid.
Erect abdominal radiograph. This image shows fluid levels in the distended sigmoid loop.
This radiograph shows decompression of the sigmoid loop following retrograde passage of a flatus tube.
 Supine abdominal radiograph in a 6-year-old child from an area in which roundworms are endemic. This image shows a sigmoid volvulus. The sigmoid loop is dilated and associated with mild proximal large-bowel dilatation.
Supine abdominal radiograph in a 6-year-old child from an area in which roundworms are endemic. This image shows a sigmoid volvulus. The sigmoid loop is dilated and associated with mild proximal large-bowel dilatation.
 This erect radiograph shows fluid levels in the sigmoid loop and in the transverse colon.
This erect radiograph shows fluid levels in the sigmoid loop and in the transverse colon.
 Erect abdominal radiograph demonstrating a giant sigmoid diverticulum. This image shows a dilated loop of bowel with air-fluid levels and intraluminal feces. This appearance mimics that of an enlarged cecum or sigmoid loop.
Erect abdominal radiograph demonstrating a giant sigmoid diverticulum. This image shows a dilated loop of bowel with air-fluid levels and intraluminal feces. This appearance mimics that of an enlarged cecum or sigmoid loop.
 Radiograph from an enema examination with water-soluble contrast material in an unprepared bowel. This image shows a giant sigmoid diverticulum that contains feces.
Radiograph from an enema examination with water-soluble contrast material in an unprepared bowel. This image shows a giant sigmoid diverticulum that contains feces.
Barium enema
A single-contrast barium enema examination is adequate because the barium readily enters the empty rectum and usually encounters a complete stenosis, which is likened to a beak, the so-called bird's beak or bird-of-prey sign.
Barium enema examination demonstrates obstruction at the rectosigmoid junction. The most common and clinically significant twist of the sigmoid occurs in the mesenteric axis, although a less frequent and more benign form of the twist may occur around the longitudinal axis of the sigmoid loop. This longitudinal twist has been variably termed the kink, axial torsion, or physiologic incomplete torsion. Patients with this twist are usually not symptomatic, and it may be an incidental finding on a routine barium enema examination.
If barium can enter the obstructed segment, spiraling of the mucosal folds may be seen. Signs of bowel ischemia, such as thumbprinting, transverse ridging, and mucosal ulceration, may be observed.
Take care not to perform a barium enema examination in patients with suspected gangrenous bowel, a pneumoperitoneum (as seen on plain abdominal radiographs), or clinical signs of peritonitis.
Sigmoidoscopy, rather than barium enema examination, is the procedure of choice if an ileosigmoid knot is suspected.
In 60-70% of patients, the diagnosis of sigmoid volvulus can be made by using plain abdominal radiographic findings. In 20-30% of patients, the 2 limbs of the twisted sigmoid colon may overlap or deviate to the right or left, obscuring the remainder of the colon. In these instances, the findings are those of a nonspecific large-bowel obstruction, and barium enema examination is required for confirmation of the diagnosis.
Other forms of large-bowel obstruction, especially those due to sigmoid colon carcinoma, pseudo-obstruction, cecal volvulus, and an ileosigmoid knot, may mimic or be confused with a sigmoid volvulus. At times, emphysematous cystitis and a giant sigmoid diverticulum may also mimic a sigmoid volvulus.
Computed Tomography
CT scan findings of sigmoid volvulus include the whirl sign, which represents tension on the tightly twisted mesocolon by the afferent and efferent limbs of the dilated colon. [15, 27, 28, 29, 20, 21]
CT scanning may be useful in identifying the etiology and site of the obstruction that are associated with other pathologies, as well as in demonstrating ischemia that results from strangulation. Sigmoid volvulus and acute colonic pseudo-obstruction (ACPO) have similar presentations, and cross-sectional imaging with CT can be used to differentiate between them. ACPO findings include colonic dilatation with a possible transition zone and no obvious mechanical cause of obstruction. [14]
CT scan signs of ischemia include a serrated beak at the site of the obstruction, mesenteric edema or engrossment, and moderate to severe thickening of the bowel wall.
Intramural gas or portal venous gas may be seen (grave prognostic signs), and in patients in whom a perforation has occurred, a large amount of free intraperitoneal gas or fluid may be noted.
Many imaging signs have been described for sigmoid volvulus, but the classic appearance may be absent in up to 50% of scanograms and 25% of CT scans. Levsky et al retrospectively reviewed 36 patients with sigmoid volvulus with an aim to evaluate the features of sigmoid volvulus on CT scanograms and cross-sectional images. Cross-sectional images of classic signs and 2 novel imaging signs (X-marks-the-spot sign and the split-wall sign) were analyzed. The authors concluded that the X-marks-the-spot sign for more complete twisting and the split-wall sign for less severe twisting may improve diagnostic confidence. [30]
CT scanning is the least invasive imaging technique that allows assessment of mural ischemia. This imaging modality helps identify the cause of an acute large-bowel obstruction in 74-86% of cases, although the sensitivity of the investigation is not yet defined.
False-positive findings may involve other forms of volvulus or obstruction and causes of large-bowel ischemia.
In a study by Kusunoki et al of 30 patients with sigmoid volvulus, the researchers found that initial CT findings of a long and distended sigmoid colon are risk factors for recurrence. Extension findings (ie, sigmoid colon extending to the diaphragm or ventral to the liver) were significantly more frequent in the recurrent group (77.3%) than in the nonrecurrent group (25.0%). In addition, the diameter of distended sigmoid colon was significantly larger in the recurrent group (11.7 ± 3.8 cm) than in the nonrecurrent group (7.1 ± 1.1 cm). [17]
Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) has been used successfully in the assessment of large-bowel obstruction (not specifically in sigmoid volvulus). These examinations were performed with the retrograde insufflation of 1000-1200 mL of air through a Foley catheter that was placed in the rectum and with scopolamine to inhibit peristalsis in order to demonstrate the site of bowel obstruction. In addition, MRI has been used in the diagnosis of mural necrosis in infants, and theoretically, this modality can be used in adults. [19, 31]
-
This radiograph demonstrates a greatly dilated sigmoid that almost fills the entire abdomen. Note the coffee bean sign. The remainder of the large bowel is not dilated, presumably because the proximal point of the twist is not causing obstruction and thus allows drainage into the sigmoid.
-
Erect abdominal radiograph. This image shows fluid levels in the distended sigmoid loop.
-
This radiograph shows decompression of the sigmoid loop following retrograde passage of a flatus tube.
-
Supine abdominal radiograph in a 6-year-old child from an area in which roundworms are endemic. This image shows a sigmoid volvulus. The sigmoid loop is dilated and associated with mild proximal large-bowel dilatation.
-
This erect radiograph shows fluid levels in the sigmoid loop and in the transverse colon.
-
Erect abdominal radiograph demonstrating a giant sigmoid diverticulum. This image shows a dilated loop of bowel with air-fluid levels and intraluminal feces. This appearance mimics that of an enlarged cecum or sigmoid loop.
-
Radiograph from an enema examination with water-soluble contrast material in an unprepared bowel. This image shows a giant sigmoid diverticulum that contains feces.



