Practice Essentials
Reactive arthritis (formerly Reiter syndrome) is used to describe an acute arthritis complicating an infection elsewhere in the body in which the infecting organism cannot be cultured from the joint fluid or synovium. [1, 2, 3, 4] Many organisms have been associated with reactive arthritis, including Chlamydia trachomatis, Shigella flexneri, Salmonella enteritidis, Campylobacter jejuni, Clostridium difficile, Ureaplasma urealyticum, Escherichia coli, Borrelia burgdorferi, Neisseria gonorrhoeae, and Chlamydia pneumoniae. [5] Reactive arthritis has been reported following COVID-19 infection. [6, 7, 8, 9] It has also been identified as a complication of Bacillus Calmette-Guerin (BCG) treatment for bladder cancer. [10]
The incidence of reactive arthritis is about 2-4% after a urogenital infection (mainly with C trachomatis) and is 0-15% after gastrointestinal infections (Salmonella, Shigella, Campylobacter, Yersinia). The incidence in population-based studies has been reported to be 0.6 to 27 per 100,000. [11, 12, 13, 14]
Approximately 80% of patients are positive for the histocompatibility antigen called human leukocyte antigen (HLA)-B27; therefore, reactive arthritis is strongly associated with HLA-B27. Because of its association with HLA-B27 and its clinical overlap with ankylosing spondylitis and psoriatic arthritis, reactive arthritis is classified as a seronegative (for rheumatoid factor) spondyloarthropathy. [15, 16]
Radiography is most important imaging technique for the detection of reactive arthritis. The general radiographic changes are similar to those of psoriatic arthritis, but the characteristic sites of abnormality are the small joints of the foot, the calcaneus, the ankle, the knee, and the sacroiliac joint. Nonspecific soft-tissue swelling is frequently seen in the toes and fingers, resulting in sausage-shaped digits.
Computed tomography (CT) can demonstrate small structural alterations of cortical and spongy bone, and magnetic resonance imaging (MRI) can identify bone marrow edema. [17]
CT is useful in localized evaluations or in determining the extent of complications, such as bony ankylosis, when plain radiographs are inconclusive. CT is also useful in interventions, such as CT-guided injections of the sacroiliac joint, and in the management of chronic, severe sacroiliac joint pain. MRI has extremely high sensitivity for reactive arthritis but low specificity. Correlation with clinical and radiographic findings is usually necessary to differentiate reactive arthritis from other seronegative arthropathies.
(Images of reactive arthritis are provided below.)
 Reactive arthritis. Radiograph of the feet in a 27-year-old man shows erosions in all the left metatarsophalangeal (MTP) joints with subluxation and valgus deformity of most of the toes. Smaller erosions in the four and fifth MTP joints of the right foot are also shown.
Reactive arthritis. Radiograph of the feet in a 27-year-old man shows erosions in all the left metatarsophalangeal (MTP) joints with subluxation and valgus deformity of most of the toes. Smaller erosions in the four and fifth MTP joints of the right foot are also shown.
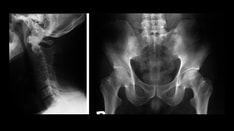
 Reactive arthritis. Radiography of the pelvis reveals bilateral, asymmetrical sacroiliitis.
Reactive arthritis. Radiography of the pelvis reveals bilateral, asymmetrical sacroiliitis.

Radiography
Radiographs are a reliable means of diagnosing reactive arthritis, particularly if the typical clinical features are present. In the early stage, radiographs are normal. The synovial joint, symphyses, and entheses are affected. An asymmetrical distribution with predominant involvement of lower extremities is seen.
The general radiographic changes are similar to those of psoriatic arthritis, but the characteristic sites of abnormality are the small joints of the foot, the calcaneus, the ankle, the knee, and the sacroiliac joint. Nonspecific soft-tissue swelling is frequently seen in the toes and fingers, resulting in sausage-shaped digits.
Periarticular osteoporosis is seen with an acute episode of arthritis. Diffuse loss of the articular space is characteristic and frequently affects the small joints of the foot, hand, wrist, knee, and ankle. Bone erosions may also occur at these joints, resulting in sacroiliitis. Erosions initially occur at the joint margins and later progress to involve subchondral bone in the central portion.
Bone proliferation is characteristic of all seronegative spondyloarthropathies and is the most helpful radiographic feature in distinguishing these conditions from rheumatoid arthritis. Linear and fluffy periosteal bone proliferations are common, especially in the calcaneus; knee; and metacarpal, metatarsal, and phalangeal shafts. A second variety of bone proliferation occurs at the sites of tendon and ligament attachments to the bone.
Intra-articular bony ankylosis is seen in small joints of the hands and feet but is less common than it is in ankylosing spondylitis and psoriatic arthritis.
Forefoot
Radiographs of the foot show asymmetrical involvement of the metatarsophalangeal and interphalangeal joints. Any joint may be affected; the joints of the great toe are commonly involved, as shown in the image below.
Reactive arthritis. Radiograph of the feet in a 27-year-old man shows erosions in all the left metatarsophalangeal (MTP) joints with subluxation and valgus deformity of most of the toes. Smaller erosions in the four and fifth MTP joints of the right foot are also shown.
Calcaneum
Calcaneal enthesopathy is characteristic of reactive arthritis and occurs in 25-50% of cases. The posterior and plantar aspects of the bone are affected, as shown in the image below. Bilateral changes are common.
 Reactive arthritis. Lateral radiograph of the foot (same patient as in the previous image) reveals a calcaneal spur and enthesitis.
Reactive arthritis. Lateral radiograph of the foot (same patient as in the previous image) reveals a calcaneal spur and enthesitis.
Ankle
Radiographic findings are seen in 30-50% of patients. Changes include soft-tissue swelling, linear or fluffy periostitis of the distal tibial and fibular diaphyses and metaphysis, and articular space loss and marginal erosions.
Knee
Knee changes are seen in 25-50% of patients. The most common abnormality is joint effusion.
Hand and wrist
Changes in the upper extremity are seen in 10-30% of cases. Abnormalities of the proximal interphalangeal joint are more common than changes in the metacarpophalangeal and distal interphalangeal joints. Involvement of the wrist is usually asymmetrical. Erosion of the metacarpal heads is demonstrated in the image below. [18]
 Reactive arthritis. Radiograph of both hands shows small erosive changes in both first metacarpal heads associated with minimal subluxation. Bone density is normal.
Reactive arthritis. Radiograph of both hands shows small erosive changes in both first metacarpal heads associated with minimal subluxation. Bone density is normal.
Manubriosternal joint and symphysis pubis
Osseous erosions and adjacent bony proliferation at the manubriosternal joints are seen in reactive arthritis and may be associated with local pain and tenderness. Similar changes are seen at the symphysis pubis.
Temporomandibular joint
Patients with reactive arthritis often have condylar erosions that cause pain and dysfunction in the temporomandibular joints. These abnormalities can be demonstrated by plain radiography. When the radiographs are inconclusive, the changes can be depicted by magnetic resonance imaging (MRI) or computed tomography (CT) scanning. [18, 19]
Sacroiliac joint
Sacroiliitis is common in reactive arthritis; while it is seen in only 5-10% of patients with acute disease, it is present in 40-60% of patients with chronic, severe disease. If supplemented with radionuclide investigation, sacroiliitis is found in 60-75% of patients.
Bilateral, asymmetrical changes, demonstrated in the image below, are most typical. Less commonly, unilateral abnormalities of the sacroiliac joint are seen in reactive arthritis, particularly early in the disease process.
Reactive arthritis. Radiography of the pelvis reveals bilateral, asymmetrical sacroiliitis.
Spine
Spinal changes are less common than the other changes in reactive arthritis and are seen less often than in ankylosing spondylitis and psoriatic arthritis. An early finding in reactive arthritis is the appearance of paravertebral syndesmophytes about the lower 3 thoracic and upper 3 lumbar vertebrae, as shown in the image below.
 Reactive arthritis. Image in 40-year-old man with nonmarginal syndesmophytes predominantly in the lower thoracic and upper lumbar spine.
Reactive arthritis. Image in 40-year-old man with nonmarginal syndesmophytes predominantly in the lower thoracic and upper lumbar spine.
Computed Tomography
Sacroiliitis is demonstrable on CT scanning earlier than on plain radiography. Early sacroiliitis manifests with small joint erosions and irregularities in the articular surfaces of the sacroiliac joint, as shown in the image below. Unilateral or asymmetrical involvement of the sacroiliac joints is also common. Enthesopathies are also demonstrable.
The high radiation dose to the patient makes CT an unattractive modality for screening large areas of the body in cases of suspected reactive arthritis, but CT is useful in localized evaluations or in determining the extent of complications, such as bony ankylosis, when plain radiographs are inconclusive.
CT is also useful in interventions, such as CT-guided injections of the sacroiliac joint (shown in the image below), and in the management of chronic, severe sacroiliac joint pain.
 Reactive arthritis. This scan, obtained in the same patient as in the previous image, shows a needle introduced into the right sacroiliac joint under CT guidance. An injection of 0.5% bupivacaine hydrochloride 5 mL (Marcaine) and methylprednisolone acetate 40 mg (Depo-Medrol) resulted in permanent relief of the patient's intractable sacroiliac pain.
Reactive arthritis. This scan, obtained in the same patient as in the previous image, shows a needle introduced into the right sacroiliac joint under CT guidance. An injection of 0.5% bupivacaine hydrochloride 5 mL (Marcaine) and methylprednisolone acetate 40 mg (Depo-Medrol) resulted in permanent relief of the patient's intractable sacroiliac pain.
Magnetic Resonance Imaging
In reactive arthritis, MRI reveals the extent of the process; the presence of bursitis and tenosynovitis, especially in the peroneal, anterior tibial, and posterior tibial tendons; and the presence of complications, such as synovial cysts. Erosive arthritis and synovitis may develop in the hands and wrists.
Synovitis and tenosynovitis are hypointense on T1-weighted images and hyperintense on T2-weighted, spin-echo images. These appearances reflect the water content of the affected areas. Short-tau inversion recovery (STIR) images reveal strong hyperintensity in the affected joints and adjacent marrow, as well as in sites of enthesitis, as shown in the images below.
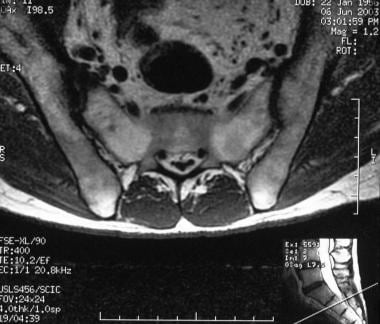 Reactive arthritis. Axial T1-weighted spin-echo image in a 47-year-old man shows widening and irregularity of upper right sacroiliac joint suggestive of unilateral sacroiliitis.
Reactive arthritis. Axial T1-weighted spin-echo image in a 47-year-old man shows widening and irregularity of upper right sacroiliac joint suggestive of unilateral sacroiliitis.
 Reactive arthritis. Coronal oblique short-tau inversion recovery (STIR) image through the sacroiliac (SI) joints in the same patient as in the previous image shows widening of the right SI joint, which contains fluid. These findings confirm right sacroiliitis.
Reactive arthritis. Coronal oblique short-tau inversion recovery (STIR) image through the sacroiliac (SI) joints in the same patient as in the previous image shows widening of the right SI joint, which contains fluid. These findings confirm right sacroiliitis.
 Reactive arthritis. Sagittal short-tau inversion recovery (STIR) image of a foot shows increased thickness of the plantar fascia (< 8 mm) with edema in the fascia, surrounding soft tissues, and adjacent marrow. These findings are diagnostic of plantar fasciitis.
Reactive arthritis. Sagittal short-tau inversion recovery (STIR) image of a foot shows increased thickness of the plantar fascia (< 8 mm) with edema in the fascia, surrounding soft tissues, and adjacent marrow. These findings are diagnostic of plantar fasciitis.
Ultrasonography
Plantar fasciitis is the most common cause of inferior heel pain, and reactive arthritis is one of the causes of plantar fasciitis. High-resolution ultrasonography reveals decreased echogenicity and increased thickness of the plantar fascia (normal thickness, 3-4 mm). [20]
In addition to reactive arthritis, a variety of rheumatologic conditions can cause plantar fasciitis. Examples include rheumatoid arthritis, ankylosing spondylitis, systemic lupus erythematosus, and gout. The ultrasonographic findings of these conditions are identical. These other diseases should be considered in the differential diagnosis and excluded with clinical history taking and other means.
Nuclear Imaging
Bone scintigraphy with bone-seeking radiopharmaceutical agents allows the early detection of reactive arthritis and provides accurate details about the extent of the disease. The distribution of abnormal radionuclide accumulation parallels that obtained by radiographic examination and may occur before radiographic and clinical alterations are apparent. Asymmetrical involvement of the lower extremity is usually seen. Increasing radioactivity related to the plantar and posterior aspects of the calcaneus is observed.
Scintigraphy provides high sensitivity but low specificity for the diagnosis of sacroiliitis. The interpretation of scintigraphic abnormalities at sacroiliac joints is difficult, because prominent uptake at this site is a normal finding. Other seronegative spondyloarthropathies, such as psoriatic arthritis, may have similar findings.
-
Reactive arthritis. Radiograph of the feet in a 27-year-old man shows erosions in all the left metatarsophalangeal (MTP) joints with subluxation and valgus deformity of most of the toes. Smaller erosions in the four and fifth MTP joints of the right foot are also shown.
-
Reactive arthritis. Lateral radiograph of the foot (same patient as in the previous image) reveals a calcaneal spur and enthesitis.
-
Reactive arthritis. Radiograph of both hands shows small erosive changes in both first metacarpal heads associated with minimal subluxation. Bone density is normal.
-
Reactive arthritis. Radiography of the pelvis reveals bilateral, asymmetrical sacroiliitis.
-
Reactive arthritis. Image in 40-year-old man with nonmarginal syndesmophytes predominantly in the lower thoracic and upper lumbar spine.
-
Reactive arthritis. Prone pelvic CT scan shows right unilateral sacroiliitis.
-
Reactive arthritis. This scan, obtained in the same patient as in the previous image, shows a needle introduced into the right sacroiliac joint under CT guidance. An injection of 0.5% bupivacaine hydrochloride 5 mL (Marcaine) and methylprednisolone acetate 40 mg (Depo-Medrol) resulted in permanent relief of the patient's intractable sacroiliac pain.
-
Reactive arthritis. Axial T1-weighted spin-echo image in a 47-year-old man shows widening and irregularity of upper right sacroiliac joint suggestive of unilateral sacroiliitis.
-
Reactive arthritis. Coronal oblique short-tau inversion recovery (STIR) image through the sacroiliac (SI) joints in the same patient as in the previous image shows widening of the right SI joint, which contains fluid. These findings confirm right sacroiliitis.
-
Reactive arthritis. Sagittal short-tau inversion recovery (STIR) image of a foot shows increased thickness of the plantar fascia (< 8 mm) with edema in the fascia, surrounding soft tissues, and adjacent marrow. These findings are diagnostic of plantar fasciitis.