Practice Essentials
Although symmetry is a characteristic of the external mammalian phenotype and of some internal organs, notably the genitourinary system, much of our internal anatomy, notably the cardiovascular, pulmonary, and gastrointestinal systems, is asymmetrical. An example of polysplenia is seen in the ultrasonogram below (see also the discussions under the different imaging modalities). No single examination is best for the evaluation of heterotaxy. Frequently, the initial examination performed in patients with this condition is plain chest radiography, which is often performed in patients with suspected congenital heart disease (for which the patients may seek clinical attention in the first place). [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13]
Plain radiographs can be helpful in delineating an abnormal visceroatrial situs. A midline heart and liver, with a midline or right-sided stomach, and symmetrical bronchial branching are diagnostic findings. However, many patients with situs ambiguus do not have any of these findings, and plain radiographic findings may erroneously suggest situs solitus or situs inversus totalis.
Patients with an abdominal catastrophe, such as midgut or gastric volvulus, also undergo plain radiography as part of their initial diagnostic imaging examination. [14, 9] On the other hand, patients with biliary atresia do not undergo plain radiography as part of their initial workup.
Historically, the diagnosis often depends on the angiographic findings in the cardiac and abdominal structures or on the results of abdominal examination via an iatrogenic pneumoperitoneum. However, ultrasonography, computed tomography (CT) scanning, and magnetic resonance imaging (MRI) are all useful in assessing the various viscerovascular abnormalities in patients with heterotaxy. [15, 16, 10, 11, 17, 18, 19, 20, 21] MRI is particularly useful, because it can also delineate cardiac defects.
CT scanning may be limited in young infants, because they have little body fat, especially if the contrast agent bolus is suboptimal.
Fetal magnetic resonance imaging (MRI) is an important adjunct imaging modality to ultrasound and has been shown to provide optimal anatomical characterization of the bronchial, hepatic, intestinal, and splenic anatomy. In cases of suspected heterotaxy on prenatal ultrasound, MRI can be useful in determining the status of the spleen and ruling out associated abnormalities, such as biliary atresia and intestinal malrotation, which might influence the prognosis. [12] MRI is limited by patient motion and its relatively long imaging times, which require optimal sedation.
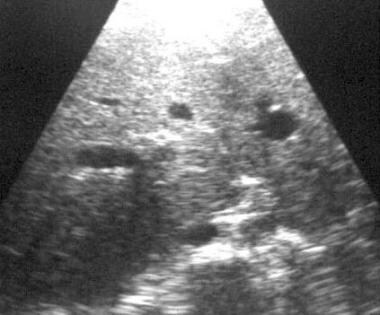
Ultrasonography (see the image below) is extremely useful, but it is operator dependent, and findings may be unrevealing in cases in which the operator fails to understand the complex anatomic relationships that result from derangement of the normal laterality.
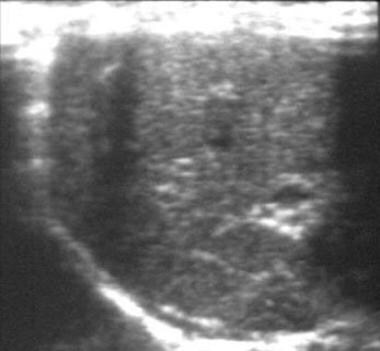
 Polysplenia. Ultrasonogram of the left upper quadrant reveals multiple, widely spaced splenules above the left kidney. Reproduced with permission.
Polysplenia. Ultrasonogram of the left upper quadrant reveals multiple, widely spaced splenules above the left kidney. Reproduced with permission.
The asymmetry is specific and originates in the genetic and molecular identity of the embryonic midline developmental field complex. [22, 23, 24] This normal asymmetrical arrangement is called situs solitus, a descriptive term derived from the Latin situs, which means position, and solitus, which means customary. Thus, situs solitus signifies the customary, or normal, asymmetrical arrangement of the viscerovascular anatomy. [25]
Situs inversus is the mirror image of situs solitus in toto. Although this condition is embryologically related to other situs anomalies, situs inversus must be strictly differentiated, because it has significantly different pathophysiologic and clinical implications. All other conditions occur in a spectrum called situs ambiguus, which is commonly changed to the Anglican situs ambiguous.
The concept of situs or laterality of the viscerovascular anatomy is important to the understanding, imaging, and interpretation of congenital visceral and vascular malformations. Assignment of laterality can be inherently difficult and affected by specific clinical biases. For example, to the cardiologist applying the concept of segmental classification of cardiac anomalies, situs refers to atrial morphology. [26] The pulmonologist is likely to assess lung lobation and bronchovascular anatomy. The gastroenterologist may focus on the presence or absence of the spleen. [27]
Situs ambiguus is associated with conditions of major clinical relevance, such as intestinal malrotation, biliary atresia, splenic abnormalities and consequent immunologic derangements, faulty gastric suspension mechanisms, displacement of abdominal viscera, and aberrant vascular structures and vascular connections. Each of these abnormalities is derived from an embryologic inability to determine laterality and establish the complex solitus asymmetry, whereas symmetrical structures remain unaffected. [28]
Patients with situs ambiguus tend to be grouped with those in whom right- or left-sided structures predominate. Generalizations may be made in these groups. Patients with right-sided symmetry typically lack a spleen, whereas patients with left-sided symmetry typically have a segmented spleen or multiple splenules. [29, 30] Spenules are usually located in the greater gastric curvature, and up to 16 spenules have been reported. [31]
These common characteristics have led to the somewhat arbitrary classification of asplenia and polysplenia. However, situs ambiguus, also called heterotaxia, occurs in a continuum; this is acknowledged in the classification of polyasplenia syndrome. This term recognizes the fact that left- and right- sided tendencies are on a continuum of heterotaxy or midline derangement. Polysplenia is usually associated with other congenital anomalies, such as agenesis or hypoplasia of the inferior vena cava, intestinal malrotation, or agenesis of the dorsal pancreas. [13]
Radiologists and other clinicians must be cognizant of the viscerovascular arrangements that are possible in infants with these conditions, and they must describe the specific viscerovascular anomalies in the patient. Many infants with situs ambiguus present with severe congenital cardiac anomalies. In these patients, knowing if an associated interruption of the inferior vena cava is present is helpful before performing cardiac catheterization. [32]
Radiography
As discussed previously, plain radiography is the first study conducted in patients with suspected heterotaxy. In many patients with situs ambiguus, radiographs provide the initial clues to the diagnosis, which should be made in patients with a midline liver, in those with a right-sided or midline stomach, and in patients with mesocardia or dextrocardia (see the images below). Special attention should be directed to the pulmonary hila for the detection of inverted or symmetrical anatomy. This evaluation is often not possible in infants, in whom the overlying thymus effectively obscures the pulmonary hila anatomy.
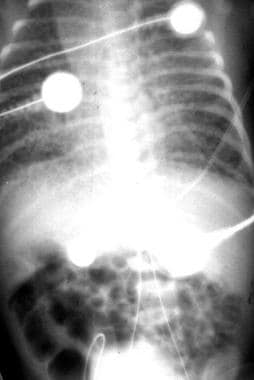
 Total anomalous pulmonary venous connection (TAPVC). Radiograph from a newborn following insertion of an umbilical catheter. This image shows dextrocardia, a midline liver, an abnormal course of the umbilical catheters, and a venous line that courses to the left of the arterial line. Findings of heterotaxy or situs ambiguus are present. This radiograph also reveals severe pulmonary edema. In this setting, the findings strongly suggest the presence of TAPVC with obstruction to the venous outflow.
Total anomalous pulmonary venous connection (TAPVC). Radiograph from a newborn following insertion of an umbilical catheter. This image shows dextrocardia, a midline liver, an abnormal course of the umbilical catheters, and a venous line that courses to the left of the arterial line. Findings of heterotaxy or situs ambiguus are present. This radiograph also reveals severe pulmonary edema. In this setting, the findings strongly suggest the presence of TAPVC with obstruction to the venous outflow.
 Polysplenia. Upper gastrointestinal (UGI) radiograph in a patient who presented with vomiting. Although many patients with heterotaxy present with severe congenital cardiac malformations, (eg, truncus arteriosus, anomalous pulmonary venous connections, atrioventricular septal defects), not all do. Some patients have milder forms of congenital heart disease, such as ventricular septal defect (VSD), or no cardiac disease. Patients with these conditions may have other anomalies, such as vomiting due to malrotation, duodenal stenosis, or jaundice due to biliary atresia. UGI studies in a patient who presented with vomiting revealed a right-sided stomach, malrotation, and a duodenal diaphragm. Findings from further evaluation were diagnostic of polysplenia. Rarely, asymptomatic manifestations, such as interruption of the inferior vena cava and polysplenia, may be discovered during medical imaging performed for unrelated complaints.
Polysplenia. Upper gastrointestinal (UGI) radiograph in a patient who presented with vomiting. Although many patients with heterotaxy present with severe congenital cardiac malformations, (eg, truncus arteriosus, anomalous pulmonary venous connections, atrioventricular septal defects), not all do. Some patients have milder forms of congenital heart disease, such as ventricular septal defect (VSD), or no cardiac disease. Patients with these conditions may have other anomalies, such as vomiting due to malrotation, duodenal stenosis, or jaundice due to biliary atresia. UGI studies in a patient who presented with vomiting revealed a right-sided stomach, malrotation, and a duodenal diaphragm. Findings from further evaluation were diagnostic of polysplenia. Rarely, asymptomatic manifestations, such as interruption of the inferior vena cava and polysplenia, may be discovered during medical imaging performed for unrelated complaints.
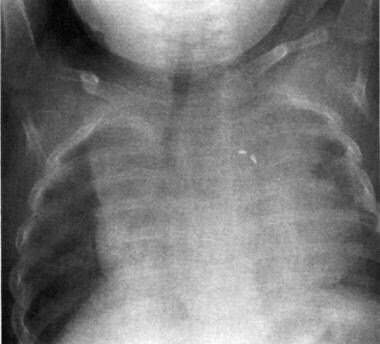
 Chest and abdominal radiograph in a neonate with asplenia. This image demonstrates a midline liver, mesocardia, and a right-sided stomach. Severe pulmonary edema is present, with a normal heart size; this finding is strongly suggestive of total anomalous pulmonary venous connection (TAPVC) with obstruction, which most likely drains subdiaphragmatically. Note the extension of the liver into both upper quadrants.
Chest and abdominal radiograph in a neonate with asplenia. This image demonstrates a midline liver, mesocardia, and a right-sided stomach. Severe pulmonary edema is present, with a normal heart size; this finding is strongly suggestive of total anomalous pulmonary venous connection (TAPVC) with obstruction, which most likely drains subdiaphragmatically. Note the extension of the liver into both upper quadrants.
When identified, bilateral eparterial bronchi (bronchus above the artery, as in a typical right hilum) are suggestive, but not diagnostic, of asplenia, whereas bilateral hyparterial bronchi (bronchus underneath the artery, as in a typical left hilum), seen in the image below, are suggestive, but not diagnostic, of polysplenia. The presence of a large azygous arch with the absence of the caval shadow on the lateral view further confirms heterotaxy, and these findings are highly suggestive of the polysplenia complex because of the interruption of the inferior vena cava with a right- or left-sided azygous continuation.
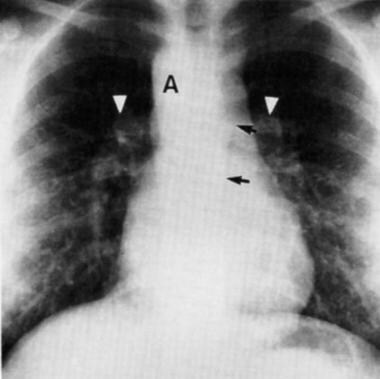 Chest radiograph in a female adolescent with polysplenia. This image demonstrates characteristic findings such as an enlarged, left-sided azygous arch (black arrows) that indicates inverted caval interruption anatomy. Bilateral hyparterial bronchi also strongly suggest heterotaxy with a left-sided tendency. The aortic arch (A) is on the right, and the cardiac apex and stomach are on the left. The white arrowheads point to symmetrical epibronchial pulmonary arteries. Reproduced with permission.
Chest radiograph in a female adolescent with polysplenia. This image demonstrates characteristic findings such as an enlarged, left-sided azygous arch (black arrows) that indicates inverted caval interruption anatomy. Bilateral hyparterial bronchi also strongly suggest heterotaxy with a left-sided tendency. The aortic arch (A) is on the right, and the cardiac apex and stomach are on the left. The white arrowheads point to symmetrical epibronchial pulmonary arteries. Reproduced with permission.
The laterality of the aortic arch is relatively unhelpful because a right-sided aortic arch occurs frequently in situs solitus, and the arch may be either right- or left-sided in situs ambiguus.
Contrast-enhanced studies of the gastrointestinal tract invariably demonstrate a rotational anomaly, which encompasses a wide spectrum. Malrotation, nonrotation, mirror-image nonrotation, and reversed rotation can all be seen in individual patients (see the images below). Duodenal atresia and/or stenosis, sometimes due to an annular pancreas, may also be present. The external indentation of a preduodenal portal vein may also be identified.
 Abnormalities of rotation. Upper gastrointestinal image demonstrates inverted nonrotation and a right-sided stomach in a patient with polysplenia.
Abnormalities of rotation. Upper gastrointestinal image demonstrates inverted nonrotation and a right-sided stomach in a patient with polysplenia.
 Abnormalities of rotation. Image obtained during a barium enema examination in a patient with polysplenia (same patient as in the previous image). This radiograph demonstrates inverted nonrotation.
Abnormalities of rotation. Image obtained during a barium enema examination in a patient with polysplenia (same patient as in the previous image). This radiograph demonstrates inverted nonrotation.
Degree of confidence
Gastrointestinal anomalies detected with contrast-enhanced examinations are present in all patients with situs ambiguus. However, these anomalies may also be present in situs solitus. Therefore, outside the clinical context, these findings are not specific for situs ambiguus.
Interruption of the inferior vena cava with azygous continuation should suggest situs ambiguus, particularly polysplenia. However, this finding is not specific, and it can be seen as an isolated anomaly in those in whom a solitus condition is otherwise present.
A right-sided aortic arch is most frequently encountered in patients with situs solitus. Typically, it indicates congenital heart disease, particularly tetralogy and truncus arteriosus, if mirror-image branching is present. The presence of a vascular ring is strongly suggested in cases of non–mirror-image branching. In situs ambiguus, the aortic arch could be either right- or left-sided. Thus, a right-sided aortic arch should not be initially construed as an indicator of a derangement in the laterality. Rotational anomalies of the midgut are most often encountered in individuals with a solitus condition.
In some series, radiographic results in as many as 50% of patients with situs ambiguus have falsely suggested either situs solitus or situs inversus totalis (see the image below).
 Radiograph in an infant with polysplenia. This image seems to demonstrate solitus anatomy. The cardiac apex and stomach lie on the left side. A large thymic shadow overlies and obscures the hilar anatomy. A surgical clip is noted on the left. Reproduced with permission.
Radiograph in an infant with polysplenia. This image seems to demonstrate solitus anatomy. The cardiac apex and stomach lie on the left side. A large thymic shadow overlies and obscures the hilar anatomy. A surgical clip is noted on the left. Reproduced with permission.
Computed Tomography
CT scanning may be helpful in delineating viscerovascular abnormalities in patients with heterotaxy and in determining whether they should be grouped with patients who have asplenia and a right-sided tendency or with those who have polysplenia and a left-sided tendency. [33, 6]
The collimation should be set to encompass the smallest structures of interest; therefore, the scanner setting varies with the age of the patient. In infants, 3-mm collimation is necessary to illustrate the bronchovascular anatomy. Intravenously administered contrast material is essential for delineation of the cardiovascular anatomy, as well as for adequate evaluation of the abdominal visceral anatomy.
An abnormal bronchial situs is highly likely in patients with these conditions; bilateral eparterial bronchi suggest asplenia, whereas bilateral hyparterial bronchi suggest polysplenia. Bilateral superior vena cavae are often present, or a single vena cava may be present on the right or left side. Malseptation of the cardiac chambers may be seen with contrast enhancement.
Conotruncal anomalies, such as transposition with anterior placement of the aorta or truncus arteriosus, may be identified.
Abnormal drainage of the pulmonary veins can also be defined. The common pulmonary vein is a contrast-enhancing chamber dorsal to the atrium that resembles cor triatriatum.
In the abdomen, the presence of abnormal splenic tissue may be identified along the greater curvature of the stomach with contrast enhancement (see the image below). Splenules are highly variable and may consist of multiple small structures, a few small structures, or a large or lobulated spleen. Lack of any splenic tissue and the absence of a splenic artery and vein indicate asplenia.
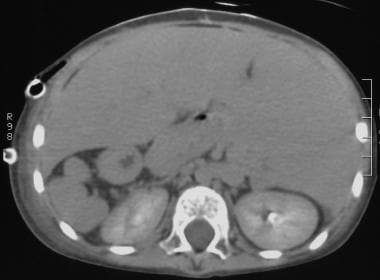 Computed tomography scan obtained in the excretory phase during the intravenous administration of contrast material in a patient with polysplenia. This image demonstrates multiple splenules in the right upper quadrant, along the greater curvature of the right-sided stomach. Note that the liver extends over the splenic mass.
Computed tomography scan obtained in the excretory phase during the intravenous administration of contrast material in a patient with polysplenia. This image demonstrates multiple splenules in the right upper quadrant, along the greater curvature of the right-sided stomach. Note that the liver extends over the splenic mass.
Anomalies of the pancreas may be somewhat more difficult to assess in the absence of the spleen because of the lack of splenic vascular landmarks, particularly in young patients in whom pancreatic attenuation may be similar to that of the surrounding tissue and in whom abdominal fat is scarce or absent. Lateralization of the liver, anomalous hepatic venous anatomy, and malpositioning or absence of the gallbladder are evident.
A preduodenal portal vein is characterized by an anterior course of the superior mesenteric venous–portal junction ventral to the pancreas. Interruption of the intrahepatic inferior vena cava occurs when this vessel is absent; instead, a large right- or left-sided azygous vein is seen adjacent to the aorta in the retrocrural area. This finding is far more characteristic of polysplenia than of asplenia. When the inferior vena cava is present, it typically lies to either side of the midline in both conditions.
Infradiaphragmatic drainage of the total anomalous pulmonary venous connection (TAPVC) can be identified by following the vertical vessel that arises in the common pulmonary vein through the esophageal hiatus into its abdominal insertion. Malrotation is also evidenced by the lack of the normal retroperitoneal course of the duodenum and the abnormal position of the cecum.
Degree of confidence
For the constellation of findings described above, the degree of confidence for CT scanning is 100%. By definition, the absence of the spleen or the presence of multiple splenules is likewise a diagnostic finding. However, for any one of the associated abnormalities, the degree of confidence can be substantially lower, depending on the particular abnormality.
Discordant positioning of the heart and abdominal viscera is characteristic and diagnostic of heterotaxy. Ambiguity of the atrial morphology and symmetrical bronchial branching are also characteristic. However, individual lesions, including conotruncal anomalies, anomalous pulmonary venous connections, intrahepatic interruption of the inferior vena cava, malrotation, and biliary atresia, may be seen in patients with normal solitus anatomy. Bilobed spleens and accessory spleens can be seen in 10% of the healthy population.
Magnetic Resonance Imaging
In many ways, MRI is an ideal modality for the examination of patients with heterotaxic conditions. As with CT scanning, the section thickness should be set to the diameter that encompasses the structures of interest. Cardiac gating is needed in the evaluation of the cardiovascular system. [17, 20, 34, 7]
Abnormal bronchial and pulmonary arterial branching anatomy are evident in the coronal and axial MRI planes. The anatomy of the superior cavae, anomalous pulmonary venous connections, conotruncal anomalies, ventricular inversion, and atrial and ventricular divisions can be identified (see the images below).
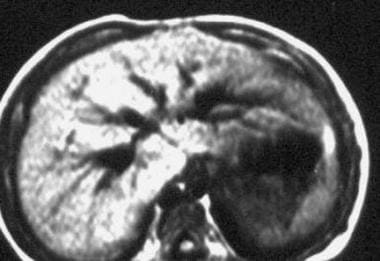
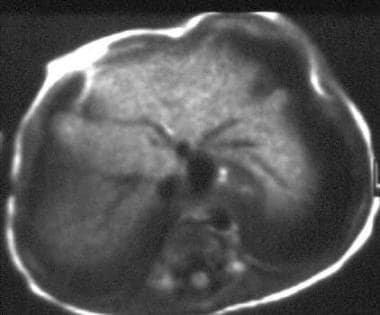 Total anomalous pulmonary venous connection (TAPVC). Axial T1-weighted magnetic resonance image in a patient with asplenia and TAPVC below the diaphragm. This image shows the anomalous vessel anterior to the gastroesophageal junction (high-intensity focus). The hepatic draining vein is the smaller-caliber vessel immediately anterior to the anomalous vessel. The caliber difference indicates the presence of an obstruction. The intrahepatic vena cava is seen to the right, and the aorta is anterior to the spine to the left of the midline.
Total anomalous pulmonary venous connection (TAPVC). Axial T1-weighted magnetic resonance image in a patient with asplenia and TAPVC below the diaphragm. This image shows the anomalous vessel anterior to the gastroesophageal junction (high-intensity focus). The hepatic draining vein is the smaller-caliber vessel immediately anterior to the anomalous vessel. The caliber difference indicates the presence of an obstruction. The intrahepatic vena cava is seen to the right, and the aorta is anterior to the spine to the left of the midline.
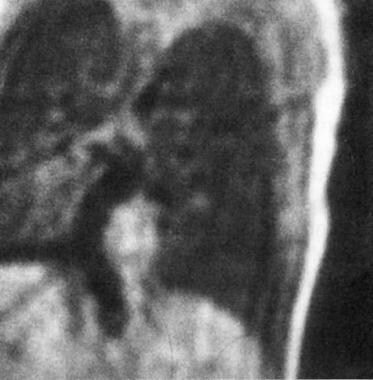 Total anomalous pulmonary venous connection (TAPVC). Coronal T1-weighted magnetic resonance image obtained in a patient with asplenia and TAPVC below the diaphragm (same patient as in the previous image). The anomalous vessel receives the pulmonary veins in the chest and courses below the diaphragm. Reproduced with permission.
Total anomalous pulmonary venous connection (TAPVC). Coronal T1-weighted magnetic resonance image obtained in a patient with asplenia and TAPVC below the diaphragm (same patient as in the previous image). The anomalous vessel receives the pulmonary veins in the chest and courses below the diaphragm. Reproduced with permission.
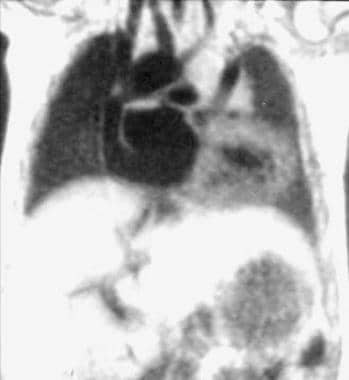 Bilateral superior cavae. Coronal T1-weighted magnetic resonance image in a patient with polysplenia. This image demonstrates bilateral superior cavae, a large atrial septal defect, and a single-ventricle anatomy. Portions of a transverse aortic arch and pulmonary outflow tract are also visible.
Bilateral superior cavae. Coronal T1-weighted magnetic resonance image in a patient with polysplenia. This image demonstrates bilateral superior cavae, a large atrial septal defect, and a single-ventricle anatomy. Portions of a transverse aortic arch and pulmonary outflow tract are also visible.
 Conotruncal anomalies and total anomalous pulmonary venous connection (TAPVC). Axial T1-weighted magnetic resonance image in a patient with asplenia. This image demonstrates truncus arteriosus type II, with pulmonary arteries arising from the arterial trunk. A single right-sided superior vena cava is noted to the right of the truncus.
Conotruncal anomalies and total anomalous pulmonary venous connection (TAPVC). Axial T1-weighted magnetic resonance image in a patient with asplenia. This image demonstrates truncus arteriosus type II, with pulmonary arteries arising from the arterial trunk. A single right-sided superior vena cava is noted to the right of the truncus.
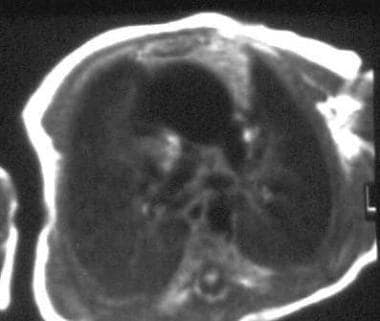
 Conotruncal anomalies and total anomalous pulmonary venous connection (TAPVC). Axial T1-weighted magnetic resonance image in a patient with asplenia (same patient as in the previous image). This image demonstrates the common pulmonary vein is dorsal to the ambiguus atrium and receives pulmonary venous return. The signal intensity of the lung fields is relatively high; this finding indicates increased water content in the edematous lung, which is due to obstruction of pulmonary venous return. Note the single-atrium, single-ventricle anatomy. The descending aorta lies to the left of the spine. The cardiac apex is to the right.
Conotruncal anomalies and total anomalous pulmonary venous connection (TAPVC). Axial T1-weighted magnetic resonance image in a patient with asplenia (same patient as in the previous image). This image demonstrates the common pulmonary vein is dorsal to the ambiguus atrium and receives pulmonary venous return. The signal intensity of the lung fields is relatively high; this finding indicates increased water content in the edematous lung, which is due to obstruction of pulmonary venous return. Note the single-atrium, single-ventricle anatomy. The descending aorta lies to the left of the spine. The cardiac apex is to the right.
Abdominal findings, including hepatic laterality, hepatic vascular anatomy, interruption or malpositioning of the inferior vena cava, positioning and size of the stomach, and presence or absence of splenic tissue, are clearly delineated with MRI. Intra-abdominal connections of the common pulmonary vein in cases of TAPVC can also be identified (see the images below).
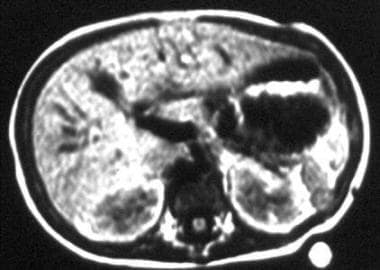 T1-weighted magnetic resonance image obtained in a patient with polysplenia. Multiple widely spaced splenules are obvious along the greater curvature of the left-sided stomach. Reproduced with permission from Hernanz-Schulman M et al. AJR Am J Roentgenol. 1990;154(4):797-802.
T1-weighted magnetic resonance image obtained in a patient with polysplenia. Multiple widely spaced splenules are obvious along the greater curvature of the left-sided stomach. Reproduced with permission from Hernanz-Schulman M et al. AJR Am J Roentgenol. 1990;154(4):797-802.
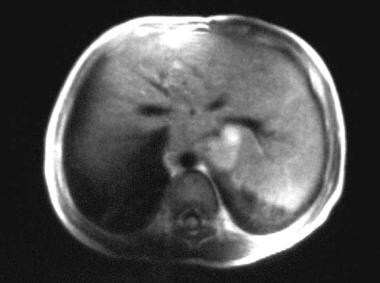
 Interruption of the inferior vena cava. Axial T1-weighted magnetic resonance image of the abdomen. This image demonstrates a large retrocrural vessel, which is similar in size and adjacent to the right side of the aorta, a finding that indicates azygous continuation and caval interruption.
Interruption of the inferior vena cava. Axial T1-weighted magnetic resonance image of the abdomen. This image demonstrates a large retrocrural vessel, which is similar in size and adjacent to the right side of the aorta, a finding that indicates azygous continuation and caval interruption.
 Interruption of the inferior vena cava. Coronal T1-weighted magnetic resonance image of the abdomen in a patient with polysplenia. This image demonstrates the enlarged azygous vein, which is parallel to the aorta and to its right. A partial volume-averaging artifact is present in the azygous vein and arch.
Interruption of the inferior vena cava. Coronal T1-weighted magnetic resonance image of the abdomen in a patient with polysplenia. This image demonstrates the enlarged azygous vein, which is parallel to the aorta and to its right. A partial volume-averaging artifact is present in the azygous vein and arch.
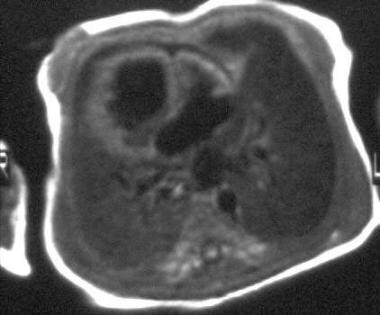
 Axial T1-weighted magnetic resonance image in a patient with asplenia. This image demonstrates hepatic extension over the greater curvature of the stomach. Mesogastria and microgastria are also present. Reproduced with permission.
Axial T1-weighted magnetic resonance image in a patient with asplenia. This image demonstrates hepatic extension over the greater curvature of the stomach. Mesogastria and microgastria are also present. Reproduced with permission.
Ultrasonography
In addition to MRI, ultrasonography may also be an ideal imaging modality in the examination of patients with situs ambiguus. Its advantages are the same as those of other modalities: ultrasonography is noninvasive, does not require radiation, and can be used to image pathology in its own plane.
An appropriate transducer, usually one of 6-MHz or higher, should be used for neonates or young infants. The infant is best examined after feeding, to prevent him or her from swallowing large amounts of air during crying and to help the infant remain quiet or asleep, factors that enable detailed imaging.
In infants, chest ultrasonography can be used to evaluate the mediastinal anatomy via the poorly calcified chest wall with the use of large cartilaginous windows and the thymic window. Laterality or bilaterality of the superior vena cavae, great vessel anatomy, ventricular position and relationships, and intracardiac anatomy can be readily assessed. The common pulmonary vein is identified dorsal to the left atrium. These findings are routinely made with echocardiography.
Abdominal ultrasonography is best begun by determining the position of the stomach. This can be found by identifying the esophagus at the midline hiatus and by following it either to the right or to the left. Splenic tissue, when present, is found along the greater curvature of the stomach. Usually, finding the adrenal gland ipsilateral to the stomach is best. Scanning along this plane reveals the splenic tissue, if present.
The appearance of the spleen, again, is highly variable; it may range from a large, septate spleen to one with multiple, small splenules that may lie close together (see the images below).
Polysplenia. Ultrasonogram of the left upper quadrant reveals multiple, widely spaced splenules above the left kidney. Reproduced with permission.
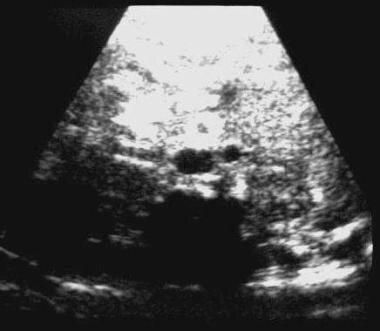
 Polysplenia. Ultrasonogram of the left upper quadrant reveals a few closely spaced splenules above the left kidney. The adrenal gland lies medial and immediately adjacent to the splenules. Reproduced with permission.
Polysplenia. Ultrasonogram of the left upper quadrant reveals a few closely spaced splenules above the left kidney. The adrenal gland lies medial and immediately adjacent to the splenules. Reproduced with permission.
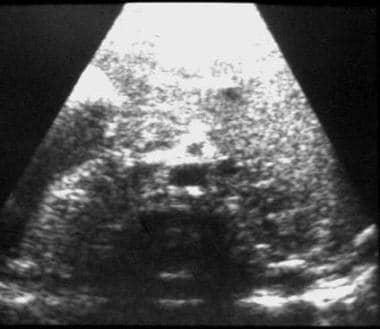
In some patients with asplenia, the liver extends across the midline and overlies the stomach; it may resemble splenic tissue. However, close attention to the internal architecture of the organ reveals the important differences. Splenic tissue has large, hilar vascular structures, whereas hepatic extension has only small, peripheral branches, which can be followed to larger trunks within the main hepatic mass (see the image below).
 Left coronal ultrasonogram obtained along the greater curvature of the stomach in a patient with asplenia. Although identification of a solid viscus in the expected location of the spleen may be misleading, note the absence of a splenic hilum and the characteristic portal echoes that parallel the long axis of the organ. These findings reveal that the solid viscus represents extension of the liver rather than splenic tissue. Reproduced with permission.
Left coronal ultrasonogram obtained along the greater curvature of the stomach in a patient with asplenia. Although identification of a solid viscus in the expected location of the spleen may be misleading, note the absence of a splenic hilum and the characteristic portal echoes that parallel the long axis of the organ. These findings reveal that the solid viscus represents extension of the liver rather than splenic tissue. Reproduced with permission.
The position of the liver in the abdomen, the location of the gallbladder, and the hepatic venous anatomy can be easily evaluated. The course of the portal vein, whether preduodenal or retroduodenal, can also be evaluated in the longitudinal and transverse planes. In the longitudinal plane, the superior mesenteric vein extends anterior to the pancreas and duodenum and courses ventrally into the liver; on transverse images, its cross-section is seen anterior to the pancreas (see the images below).
 Preduodenal portal vein. Transverse ultrasonogram obtained just caudal to the pancreas in an infant with polysplenia. This image demonstrates the superior mesenteric vein just ventral to and to the left of the superior mesenteric artery (denoted by the characteristic hyperechoic halo). The relationship of the artery and vein is abnormal; the vein is to the left and anterior to the artery, rather than to the right and in the same plane as the artery in the normal relationship. Reproduced with permission.
Preduodenal portal vein. Transverse ultrasonogram obtained just caudal to the pancreas in an infant with polysplenia. This image demonstrates the superior mesenteric vein just ventral to and to the left of the superior mesenteric artery (denoted by the characteristic hyperechoic halo). The relationship of the artery and vein is abnormal; the vein is to the left and anterior to the artery, rather than to the right and in the same plane as the artery in the normal relationship. Reproduced with permission.
 Preduodenal portal vein. Transverse ultrasonogram obtained at the level of the pancreas in an infant with polysplenia (same patient as in the previous image). This image demonstrates that the superior mesenteric vein lies ventral to the pancreas and is separated from the superior mesenteric artery (denoted by the characteristic hyperechoic halo) by the pancreas. Reproduced with permission.
Preduodenal portal vein. Transverse ultrasonogram obtained at the level of the pancreas in an infant with polysplenia (same patient as in the previous image). This image demonstrates that the superior mesenteric vein lies ventral to the pancreas and is separated from the superior mesenteric artery (denoted by the characteristic hyperechoic halo) by the pancreas. Reproduced with permission.
 Preduodenal portal vein. Sagittal ultrasonogram obtained in an infant with polysplenia (same patient as in previous 2 images). This image demonstrates the superior mesenteric vein, which courses ventral to the pancreas, in a staircase configuration. Reproduced with permission.
Preduodenal portal vein. Sagittal ultrasonogram obtained in an infant with polysplenia (same patient as in previous 2 images). This image demonstrates the superior mesenteric vein, which courses ventral to the pancreas, in a staircase configuration. Reproduced with permission.
 Preduodenal portal vein. Sagittal ultrasonogram in an infant with asplenia. This image demonstrates the characteristic staircase configuration of the ventral course of the superior mesenteric–portal junction anterior to the pancreas and duodenum. The hyperechoic triangular structure indicates gas within the duodenal cap.
Preduodenal portal vein. Sagittal ultrasonogram in an infant with asplenia. This image demonstrates the characteristic staircase configuration of the ventral course of the superior mesenteric–portal junction anterior to the pancreas and duodenum. The hyperechoic triangular structure indicates gas within the duodenal cap.
Azygous continuation of an interrupted intrahepatic inferior vena cava is best evaluated on the transverse view. The intrahepatic cava is absent. Instead, a vessel is present adjacent to the aorta in the retrocrural region; it represents the right- or left-sided azygous continuation. Doppler ultrasonographic imaging can reveal the arterial signal of the aorta and the venous signal of the azygous vein. On coronal images, the 2 parallel vessels are seen along the retroperitoneum, entering the chest cavity. An intact inferior vena cava tends to line up with the aorta to either side of the midline and to cross over in piggyback fashion, when necessary, to enter the ambiguus atrium (see the images below).
 Interruption of the inferior vena cava. Transverse ultrasonogram of the abdomen in a patient with polysplenia. This image demonstrates a large retrocrural vessel, which is similar in size and adjacent to the right side of the aorta, a finding that indicates azygous continuation and caval interruption.
Interruption of the inferior vena cava. Transverse ultrasonogram of the abdomen in a patient with polysplenia. This image demonstrates a large retrocrural vessel, which is similar in size and adjacent to the right side of the aorta, a finding that indicates azygous continuation and caval interruption.
 Intact inferior vena cava. Transverse ultrasonogram of the abdomen in patient with polysplenia. This image demonstrates an antecrural vessel, a finding that indicates an intact inferior vena cava, which is in the process of crossing over anterior to the aorta to enter the atrium.
Intact inferior vena cava. Transverse ultrasonogram of the abdomen in patient with polysplenia. This image demonstrates an antecrural vessel, a finding that indicates an intact inferior vena cava, which is in the process of crossing over anterior to the aorta to enter the atrium.
 Intact inferior cava. Sagittal ultrasonogram of the abdomen in a patient with polysplenia (same patient as in the previous image). This image demonstrates an antecrural vessel, a finding that indicates an intact inferior cava, which is in the process of crossing over anterior to the aorta to enter the atrium. Compare this ultrasonogram with the transverse ultrasonogram in the previous image.
Intact inferior cava. Sagittal ultrasonogram of the abdomen in a patient with polysplenia (same patient as in the previous image). This image demonstrates an antecrural vessel, a finding that indicates an intact inferior cava, which is in the process of crossing over anterior to the aorta to enter the atrium. Compare this ultrasonogram with the transverse ultrasonogram in the previous image.
 Intact inferior cava. Sagittal ultrasonogram of the abdomen in a patient with polysplenia. This image demonstrates an intact intrahepatic cava with a normal appearance. Because the abdominal caval laterality was congruent with that of the atria in this patient, crossing over did not occur. Reproduced with permission.
Intact inferior cava. Sagittal ultrasonogram of the abdomen in a patient with polysplenia. This image demonstrates an intact intrahepatic cava with a normal appearance. Because the abdominal caval laterality was congruent with that of the atria in this patient, crossing over did not occur. Reproduced with permission.
 Intact inferior vena cava. Transverse ultrasonogram in a patient with asplenia. This image demonstrates the aorta and vena cava on either side of the midline, an appearance that simulates solitus anatomy. Reproduced with permission.
Intact inferior vena cava. Transverse ultrasonogram in a patient with asplenia. This image demonstrates the aorta and vena cava on either side of the midline, an appearance that simulates solitus anatomy. Reproduced with permission.
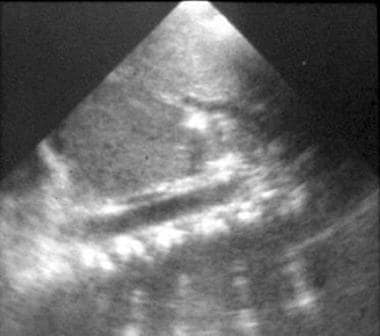
In cases of total anomalous venous connections below the diaphragm, the anomalous connecting vein is easily identified; it enters the abdomen anterior to the esophagus through the esophageal hiatus. Its course to the exact point of abdominal drainage can then be determined (see the image below).
 Total anomalous pulmonary venous connection (TAPVC). Sagittal abdominal ultrasonogram in a patient with asplenia and TAPVC below the diaphragm. This image shows that the anomalous vessel bypasses the portal vein and connects to a hepatic vein. Note the abrupt caliber change in the draining pulmonary vein in this patient with severe pulmonary venous outflow obstruction. Reproduced with permission.
Total anomalous pulmonary venous connection (TAPVC). Sagittal abdominal ultrasonogram in a patient with asplenia and TAPVC below the diaphragm. This image shows that the anomalous vessel bypasses the portal vein and connects to a hepatic vein. Note the abrupt caliber change in the draining pulmonary vein in this patient with severe pulmonary venous outflow obstruction. Reproduced with permission.
Other anomalies, such as a dilated duodenum in cases of duodenal stenosis and/or atresia, midline horseshoe adrenal gland, and renal anomalies, can also be identified.
The disadvantages of ultrasonography are that it is operator dependent and that sound waves cannot penetrate bone or air. Therefore, bronchial branching anatomy cannot be accurately evaluated, and the abdominal examination may be relatively impeded in patients with large amounts of bowel gas. Although ultrasonography is extremely useful in heterotaxic conditions, this modality is also highly operator dependent. An operator's failure to understand the anomalies that occur could lead to a significant number of false-positive and false-negative results. For example, a failure to understand the location of splenules along the greater curvature of the stomach could prevent a diagnosis. Conversely, imaging of the hepatic extension in asplenia could lead to a false diagnosis of polysplenia or situs inversus totalis.
Nuclear Imaging
In the diagnosis of asplenia versus polysplenia, resorting to the liver-spleen scan is tempting. Indeed, in healthy patients with solitus anatomy, the liver and spleen are clearly identified with the use of technetium-99m sulfur-colloid (99mTc-SC) scintigraphy. [18, 35, 36]
However, differentiation of hepatic versus splenic activity is considerably more difficult (1) in patients who may have no spleen and in whom the liver may extend into both upper quadrants and (2) in those who may have splenic tissue in either quadrant (see the image below). Unlike ultrasonography and MRI, scintigraphy requires radiation exposure and venipuncture.
When splenules are close together, the splenic mass appears as a single spleen, which is difficult to differentiate from situs solitus or situs inversus totalis. If the hepatic mass extends to both upper quadrants, identification of the splenic tissue may necessitate selective splenic scintigraphy with radiolabeled, heat-damaged red blood cells and/or hepatobiliary scintigraphy.
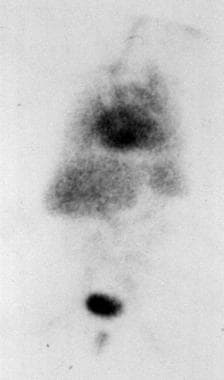 Anterior scintigraphic examination obtained in a patient with asplenia. Hepatic extension into the left upper quadrant may simulate nonexistent splenic tissue. Reproduced with permission.
Anterior scintigraphic examination obtained in a patient with asplenia. Hepatic extension into the left upper quadrant may simulate nonexistent splenic tissue. Reproduced with permission.
In some patients, splenic activity may be clearly distinct from that of the liver if the splenules are clearly distinguished from the liver and from each other.
Scintigraphy with a bolus of contrast material that is administered during angiography may demonstrate caval interruption with azygous continuation, if the agent is injected into a foot vein. The images may demonstrate the absence of a direct connection to the inferior atrium. However, other viscerovascular abnormalities are not typically depicted. Given the availability of ultrasonography, CT scanning, and MRI, scintigraphic evaluation is needed infrequently.
Angiography
Before the advent of cross-sectional imaging techniques, angiography was used to diagnose heterotaxy, define cardiac anatomy, and define abdominal viscerovascular heterotaxy.
Abdominal angiograms in patients with polysplenia demonstrate a variable arterial supply to the splenules. Typically, these are supplied by 2 or more arteries, which may arise as branches of a common celiacomesenteric trunk, from terminal branches of the gastroepiploic artery, or directly from the ipsilateral side of the abdominal aorta. The splenules are identified with a blush that moves more rapidly through the splenic tissue than through the overlying liver.
Although MRI and echocardiography are extensively used for the evaluation of cardiac malformations in these patients, cineangiography retains an eminent place in the preoperative cardiac evaluation in these complex cases. Abdominal angiography is no longer used for the evaluation of these conditions.
Although venous anomalies, such as azygous continuation of an interrupted intrahepatic inferior cava, may occur as an isolated anomaly in situs solitus, the lobulated splenules and abnormal celiacomesenteric anatomic branching is highly suggestive of the syndrome.
-
Polysplenia. Ultrasonogram of the left upper quadrant reveals multiple, widely spaced splenules above the left kidney. Reproduced with permission.
-
Polysplenia. Ultrasonogram of the left upper quadrant reveals a few closely spaced splenules above the left kidney. The adrenal gland lies medial and immediately adjacent to the splenules. Reproduced with permission.
-
T1-weighted magnetic resonance image obtained in a patient with polysplenia. Multiple widely spaced splenules are obvious along the greater curvature of the left-sided stomach. Reproduced with permission from Hernanz-Schulman M et al. AJR Am J Roentgenol. 1990;154(4):797-802.
-
Computed tomography scan obtained in the excretory phase during the intravenous administration of contrast material in a patient with polysplenia. This image demonstrates multiple splenules in the right upper quadrant, along the greater curvature of the right-sided stomach. Note that the liver extends over the splenic mass.
-
Abnormalities of rotation. Upper gastrointestinal image demonstrates inverted nonrotation and a right-sided stomach in a patient with polysplenia.
-
Abnormalities of rotation. Image obtained during a barium enema examination in a patient with polysplenia (same patient as in the previous image). This radiograph demonstrates inverted nonrotation.
-
Interruption of the inferior vena cava. Transverse ultrasonogram of the abdomen in a patient with polysplenia. This image demonstrates a large retrocrural vessel, which is similar in size and adjacent to the right side of the aorta, a finding that indicates azygous continuation and caval interruption.
-
Interruption of the inferior vena cava. Axial T1-weighted magnetic resonance image of the abdomen. This image demonstrates a large retrocrural vessel, which is similar in size and adjacent to the right side of the aorta, a finding that indicates azygous continuation and caval interruption.
-
Interruption of the inferior vena cava. Coronal T1-weighted magnetic resonance image of the abdomen in a patient with polysplenia. This image demonstrates the enlarged azygous vein, which is parallel to the aorta and to its right. A partial volume-averaging artifact is present in the azygous vein and arch.
-
Intact inferior vena cava. Transverse ultrasonogram of the abdomen in patient with polysplenia. This image demonstrates an antecrural vessel, a finding that indicates an intact inferior vena cava, which is in the process of crossing over anterior to the aorta to enter the atrium.
-
Intact inferior cava. Sagittal ultrasonogram of the abdomen in a patient with polysplenia (same patient as in the previous image). This image demonstrates an antecrural vessel, a finding that indicates an intact inferior cava, which is in the process of crossing over anterior to the aorta to enter the atrium. Compare this ultrasonogram with the transverse ultrasonogram in the previous image.
-
Intact inferior cava. Sagittal ultrasonogram of the abdomen in a patient with polysplenia. This image demonstrates an intact intrahepatic cava with a normal appearance. Because the abdominal caval laterality was congruent with that of the atria in this patient, crossing over did not occur. Reproduced with permission.
-
Intact inferior vena cava. Transverse ultrasonogram in a patient with asplenia. This image demonstrates the aorta and vena cava on either side of the midline, an appearance that simulates solitus anatomy. Reproduced with permission.
-
Total anomalous pulmonary venous connection (TAPVC). Sagittal abdominal ultrasonogram in a patient with asplenia and TAPVC below the diaphragm. This image shows that the anomalous vessel bypasses the portal vein and connects to a hepatic vein. Note the abrupt caliber change in the draining pulmonary vein in this patient with severe pulmonary venous outflow obstruction. Reproduced with permission.
-
Total anomalous pulmonary venous connection (TAPVC). Axial T1-weighted magnetic resonance image in a patient with asplenia and TAPVC below the diaphragm. This image shows the anomalous vessel anterior to the gastroesophageal junction (high-intensity focus). The hepatic draining vein is the smaller-caliber vessel immediately anterior to the anomalous vessel. The caliber difference indicates the presence of an obstruction. The intrahepatic vena cava is seen to the right, and the aorta is anterior to the spine to the left of the midline.
-
Total anomalous pulmonary venous connection (TAPVC). Coronal T1-weighted magnetic resonance image obtained in a patient with asplenia and TAPVC below the diaphragm (same patient as in the previous image). The anomalous vessel receives the pulmonary veins in the chest and courses below the diaphragm. Reproduced with permission.
-
Bilateral superior cavae. Coronal T1-weighted magnetic resonance image in a patient with polysplenia. This image demonstrates bilateral superior cavae, a large atrial septal defect, and a single-ventricle anatomy. Portions of a transverse aortic arch and pulmonary outflow tract are also visible.
-
Preduodenal portal vein. Transverse ultrasonogram obtained just caudal to the pancreas in an infant with polysplenia. This image demonstrates the superior mesenteric vein just ventral to and to the left of the superior mesenteric artery (denoted by the characteristic hyperechoic halo). The relationship of the artery and vein is abnormal; the vein is to the left and anterior to the artery, rather than to the right and in the same plane as the artery in the normal relationship. Reproduced with permission.
-
Preduodenal portal vein. Transverse ultrasonogram obtained at the level of the pancreas in an infant with polysplenia (same patient as in the previous image). This image demonstrates that the superior mesenteric vein lies ventral to the pancreas and is separated from the superior mesenteric artery (denoted by the characteristic hyperechoic halo) by the pancreas. Reproduced with permission.
-
Preduodenal portal vein. Sagittal ultrasonogram obtained in an infant with polysplenia (same patient as in previous 2 images). This image demonstrates the superior mesenteric vein, which courses ventral to the pancreas, in a staircase configuration. Reproduced with permission.
-
Preduodenal portal vein. Sagittal ultrasonogram in an infant with asplenia. This image demonstrates the characteristic staircase configuration of the ventral course of the superior mesenteric–portal junction anterior to the pancreas and duodenum. The hyperechoic triangular structure indicates gas within the duodenal cap.
-
Conotruncal anomalies and total anomalous pulmonary venous connection (TAPVC). Axial T1-weighted magnetic resonance image in a patient with asplenia. This image demonstrates truncus arteriosus type II, with pulmonary arteries arising from the arterial trunk. A single right-sided superior vena cava is noted to the right of the truncus.
-
Conotruncal anomalies and total anomalous pulmonary venous connection (TAPVC). Axial T1-weighted magnetic resonance image in a patient with asplenia (same patient as in the previous image). This image demonstrates the common pulmonary vein is dorsal to the ambiguus atrium and receives pulmonary venous return. The signal intensity of the lung fields is relatively high; this finding indicates increased water content in the edematous lung, which is due to obstruction of pulmonary venous return. Note the single-atrium, single-ventricle anatomy. The descending aorta lies to the left of the spine. The cardiac apex is to the right.
-
Chest and abdominal radiograph in a neonate with asplenia. This image demonstrates a midline liver, mesocardia, and a right-sided stomach. Severe pulmonary edema is present, with a normal heart size; this finding is strongly suggestive of total anomalous pulmonary venous connection (TAPVC) with obstruction, which most likely drains subdiaphragmatically. Note the extension of the liver into both upper quadrants.
-
Chest radiograph in a female adolescent with polysplenia. This image demonstrates characteristic findings such as an enlarged, left-sided azygous arch (black arrows) that indicates inverted caval interruption anatomy. Bilateral hyparterial bronchi also strongly suggest heterotaxy with a left-sided tendency. The aortic arch (A) is on the right, and the cardiac apex and stomach are on the left. The white arrowheads point to symmetrical epibronchial pulmonary arteries. Reproduced with permission.
-
Radiograph in an infant with polysplenia. This image seems to demonstrate solitus anatomy. The cardiac apex and stomach lie on the left side. A large thymic shadow overlies and obscures the hilar anatomy. A surgical clip is noted on the left. Reproduced with permission.
-
Axial T1-weighted magnetic resonance image in a patient with asplenia. This image demonstrates hepatic extension over the greater curvature of the stomach. Mesogastria and microgastria are also present. Reproduced with permission.
-
Left coronal ultrasonogram obtained along the greater curvature of the stomach in a patient with asplenia. Although identification of a solid viscus in the expected location of the spleen may be misleading, note the absence of a splenic hilum and the characteristic portal echoes that parallel the long axis of the organ. These findings reveal that the solid viscus represents extension of the liver rather than splenic tissue. Reproduced with permission.
-
Anterior scintigraphic examination obtained in a patient with asplenia. Hepatic extension into the left upper quadrant may simulate nonexistent splenic tissue. Reproduced with permission.
-
Total anomalous pulmonary venous connection (TAPVC). Radiograph from a newborn following insertion of an umbilical catheter. This image shows dextrocardia, a midline liver, an abnormal course of the umbilical catheters, and a venous line that courses to the left of the arterial line. Findings of heterotaxy or situs ambiguus are present. This radiograph also reveals severe pulmonary edema. In this setting, the findings strongly suggest the presence of TAPVC with obstruction to the venous outflow.
-
Polysplenia. Upper gastrointestinal (UGI) radiograph in a patient who presented with vomiting. Although many patients with heterotaxy present with severe congenital cardiac malformations, (eg, truncus arteriosus, anomalous pulmonary venous connections, atrioventricular septal defects), not all do. Some patients have milder forms of congenital heart disease, such as ventricular septal defect (VSD), or no cardiac disease. Patients with these conditions may have other anomalies, such as vomiting due to malrotation, duodenal stenosis, or jaundice due to biliary atresia. UGI studies in a patient who presented with vomiting revealed a right-sided stomach, malrotation, and a duodenal diaphragm. Findings from further evaluation were diagnostic of polysplenia. Rarely, asymptomatic manifestations, such as interruption of the inferior vena cava and polysplenia, may be discovered during medical imaging performed for unrelated complaints.
-
Sagittal ultrasonogram in a patient with asplenia and total anomalous pulmonary venous connections (TAPVCs) below the diaphragm. This image demonstrates an anomalous vessel that enters the abdomen and courses into the liver. Although pulmonary angiograms could delineate the anomalous pulmonary venous connection, the anomalous vessel can be easily identified with less-invasive imaging. Ultrasonography, magnetic resonance imaging, or computed tomography scanning can demonstrate the anomalous vessel as it enters the abdomen anterior to the esophagus.




