Practice Essentials
Intracranial germinoma is uncommon and accounts for less than 1% of all intracranial tumors. It usually arises in the midline of the brain, most commonly in the pineal region. Pineal germinoma tends to spread through cerebrospinal fluid (CSF), and metastases predominantly occur in adolescents or young adults. Dissemination usually develops several years after initial tumor diagnosis and has a relatively good clinical prognosis. [1] Pineal germinoma originates from primordial germ cells, similar to those in gonadal germinoma. Cells have large nuclei with prominent nucleoli, and lymphocytic infiltration is common. CSF cells stain for placental alkaline phosphatase and beta-human chorionic gonadotropin (β-HCG). [2]
Although pineal region neoplasms constitute only 0.3 to 2.7% of intracranial tumors, they are considered an important clinical entity because of their strategic location. Pineal region neoplasms can be classified into 3 major groups according to their cellular origin: (1) tumors of germ cell origin, (2) tumors of pineal cell origin, and (3) tumors of other cell origin. Tumors of germ cell origin include germinoma, mature teratoma, malignant teratoma, embryonal cell carcinoma, endodermal sinus tumor, choriocarcinoma, and mixed germ cell tumor. Synchronous pineal and suprasellar germinomas are found in 5-10% of cases. Germinomas account for 50% of pineal parenchymal tumors. They are much more common among males (male-to-female ratio 13:1). Most patients are 20 years of age or younger at the time of evaluation. [2]
Intracranial germinoma is diagnosed on the basis of magnetic resonance imaging (MRI) findings, serum and CSF markers, and tumor stereotactic biopsy. Imaging techniques such as susceptibility-weighted imaging (SWI), T2* gradient echo (GRE), or arterial spin labeling–based perfusion-weighted MRI (ASL-PWI) facilitate diagnosis. Germinoma is a highly radiosensitive tumor, with survival rates greater than 90% in the context of chemoradiotherapy. However, patients with resistant disease have limited therapeutic options and poor survival. [3, 4] Findings that point to worse prognosis include local invasion, CSF seeding, and extensive peritumor edema. In germinoma, proximal seeding is most common. [2]
MRI is the preferred imaging modality. MRI enables accurate delineation of pineal masses before surgery and allows true pineal masses to be distinguished from parapineal masses that impinge on the pineal gland. [5, 6] MRI is not perfect in detecting calcifications. Computed tomography (CT) scanning may be performed to evaluate a calcified pineal gland that is associated with a pineal germinoma or tumor calcification that is associated with other neoplasms in the pineal region. [7, 8, 9, 10, 11]
No abnormality is seen on arterial phase cerebral angiography for patients with pineal germinoma. In the venous phase, superior and posterior displacement of internal cerebral veins and of the vein of Galen may be seen on lateral projections. A larger pineal region mass can cause posterior bowing of the precentral cerebellar vein. On anteroposterior projections, the posterior portion of the 2 internal cerebral veins may be slightly separated.
Germinoma is associated with a high incidence of pineal gland calcification. This tumor does not calcify, but it may engulf a calcified pineal gland. A calcified pineal gland on plain radiography in a boy younger than 10 years suggests pineal germinoma. The degree of confidence with radiography is low. Furthermore, pineal calcification can be seen in patients with pineal cell tumors.
Standard treatment includes neoadjuvant chemotherapy (NC) followed by radiotherapy (RT). Some data suggest that a reduced NC course and whole ventricular radiotherapy (WVR) may effectively treat adult germinoma. [12]
(MRI scans of pineal germinomas are presented below.)
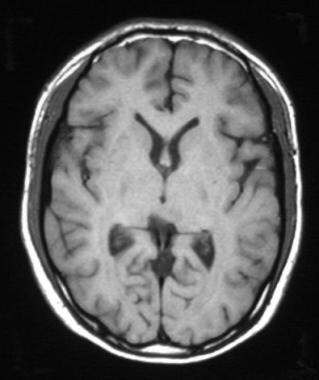 Pineal germinoma in a 19-year-old man. Axial T1-weighted MRI shows an isointense lesion in the pineal region.
Pineal germinoma in a 19-year-old man. Axial T1-weighted MRI shows an isointense lesion in the pineal region.
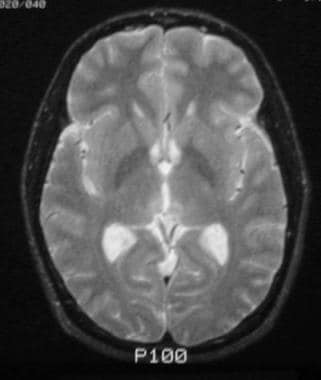
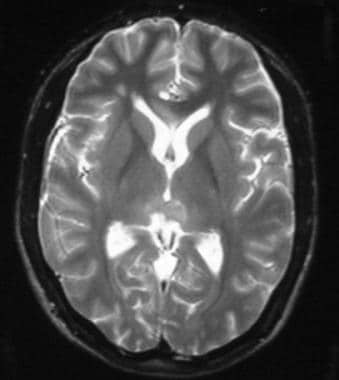 Pineal germinoma in a 19-year-old man. Axial T2-weighted MRI shows an isointense mass in the pineal region.
Pineal germinoma in a 19-year-old man. Axial T2-weighted MRI shows an isointense mass in the pineal region.
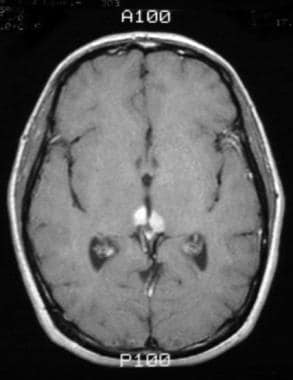
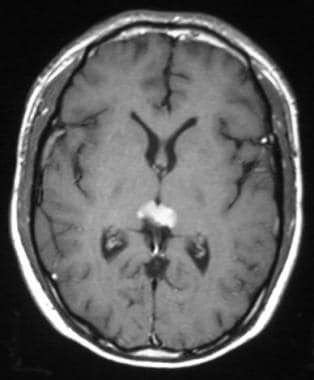 Pineal germinoma in a 19-year-old man. Axial T1-weighted contrast-enhanced MRI shows a homogeneously enhancing mass in the pineal region.
Pineal germinoma in a 19-year-old man. Axial T1-weighted contrast-enhanced MRI shows a homogeneously enhancing mass in the pineal region.
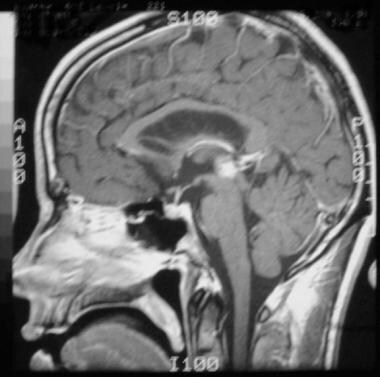
 Pineal germinoma in a 19-year-old man. Sagittal T1-weighted contrast-enhanced MRI shows an enhancing mass in the pineal region. Compression of the quadrigeminal plate and aqueduct is shown.
Pineal germinoma in a 19-year-old man. Sagittal T1-weighted contrast-enhanced MRI shows an enhancing mass in the pineal region. Compression of the quadrigeminal plate and aqueduct is shown.
Computed Tomography
Nonenhanced CT scans typically show a slightly hyperattenuating mass that engulfs a prominent calcified pineal gland. Contrast-enhanced CT scanning reveals homogeneous and intense enhancement.
CT scanning is more sensitive than plain radiography in depicting pineal calcification. Small speckles of calcification can be seen in children as young as 6 years and are considered a normal finding. In general, pineal calcification in children younger than 6 years is suggestive of pineal neoplasm. Some authors believe that pineal calcification is uncommon in children younger than 10 years and that pineal calcifications should be less than 1 cm in diameter in size.
CT scans typically show calcification in the adult pineal gland. In children younger than 5 years, calcification often is not present. Calcification of the pineal gland reaches a plateau at about 30 years of age. Calcifications can be identified more easily on a head CT scan, sometimes leading to accurate diagnosis. Pineal parenchymal tumors (eg, pineocytoma, pineoblastoma) tend to peripherally disperse calcification, whereas germ cell tumors tend to engulf calcifications. [2]
Zhang et al have reported on the use of 16-slice helical CT perfusion imaging for assessing germinomas and other intracranial neoplasms. [13] Germinoma was notable for a high permeability surface value and a rapid escalated time-density curve with a slowly and continuously elevated platform.
(See the image below.)
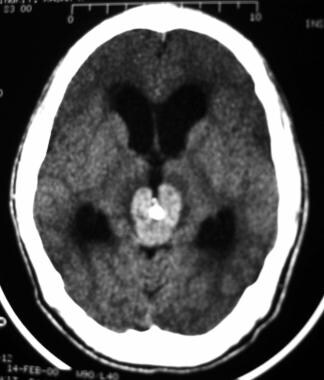 Axial, post-contrast CT shows an enhancing mass in the pineal region, which engulfs a calcified pineal gland
Axial, post-contrast CT shows an enhancing mass in the pineal region, which engulfs a calcified pineal gland
Magnetic Resonance Imaging
Germinomas are usually isointense relative to cerebral gray matter on both T1-weighted images and T2-weighted images. [8, 2] Occasionally, tumors may be hypointense on T1-weighted images and hyperintense on T2-weighted images. After the intravenous injection of gadolinium-based contrast material, homogeneous and intense enhancement is seen. For this reason, contrast-enhanced MRI is particularly useful for evaluating the subarachnoid seeding of germinomas.
Dense tumors such as pineoblastoma and germinoma show restricted diffusion on diffusion-weighted images. On the other hand, pineal cysts are nonenhancing and usually have a thin wall; therefore, an image showing a thick wall excludes diagnosis of a cyst. [2, 8] Full-spine MRI may be considered as part of the initial evaluation. Local invasion and remote seeding are significant for prognosis and may drastically change initial management and adjuvant therapy. [2]
MRI enables accurate anatomic delineation of the tumoral mass and determination of its relationships with surrounding structures. Thus, MRI can provide adequate information that assists the neurosurgeon in planning for biopsy.
Gadolinium-based contrast agents have been linked to the development of nephrogenic systemic fibrosis (NSF) or nephrogenic fibrosing dermopathy (NFD). This disease has occurred in patients with moderate to end-stage renal disease after they were given a gadolinium-based contrast agent to enhance MRI or magnetic resonance angiography (MRA) scans. NSF/NFD is a debilitating and sometimes fatal disease. Characteristics include red or dark patches on the skin; burning, itching, swelling, hardening, and tightening of the skin; yellow spots on the whites of the eyes; joint stiffness with trouble moving or straightening the arms, hands, legs, or feet; pain deep in the hip bones or ribs; and muscle weakness.
Pineal germinoma predominantly involves the pineal gland, but the medial aspect of the pulvinar of the thalamus is frequently involved. In contrast to pineal germinomas, benign cysts in the pineal gland, which have been found in almost a quarter of healthy young adults, are sharply delineated and ovoid shaped, without intracystic trabeculations and with signal intensity similar to that of ventricular CSF on both T1- and T2-weighted images. Pineal cysts are usually an incidental finding but in rare cases may become symptomatic. [14] Occasionally, small cystic changes may be seen in a germinoma. A study of pineal cysts found a mean largest inner cross-sectional diameter of 4.3 mm (range, 2-14 mm). [15]
Papillary tumor of the pineal region (PTPR) differs from pineal germinoma in that PTPR has been found to have intrinsic T1 hyperintensity; the presence of such a mass in the posterior commissure or pineal region, with absence of fat, hemorrhage, melanin, or calcification on imaging, suggests the diagnosis of PTPR. [16]
(Pineal germinomas are depicted in the MRI scans below.)
Pineal germinoma in a 19-year-old man. Axial T1-weighted MRI shows an isointense lesion in the pineal region.
Pineal germinoma in a 19-year-old man. Axial T2-weighted MRI shows an isointense mass in the pineal region.
Pineal germinoma in a 19-year-old man. Axial T1-weighted contrast-enhanced MRI shows a homogeneously enhancing mass in the pineal region.
Pineal germinoma in a 19-year-old man. Sagittal T1-weighted contrast-enhanced MRI shows an enhancing mass in the pineal region. Compression of the quadrigeminal plate and aqueduct is shown.
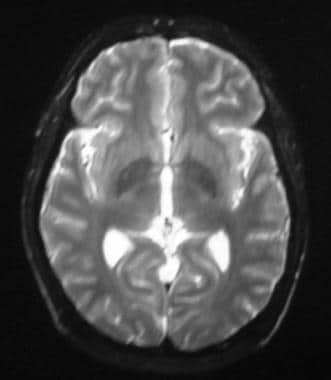
 Pineal germinoma in a 30-year-old man. Axial T2-weighted MRI shows a mildly hyperintense lesion involving the pineal region.
Pineal germinoma in a 30-year-old man. Axial T2-weighted MRI shows a mildly hyperintense lesion involving the pineal region.
 Pineal germinoma in a 30-year-old man. Sagittal T1-weighted contrast-enhanced image shows an enhancing mass in the pineal region.
Pineal germinoma in a 30-year-old man. Sagittal T1-weighted contrast-enhanced image shows an enhancing mass in the pineal region.
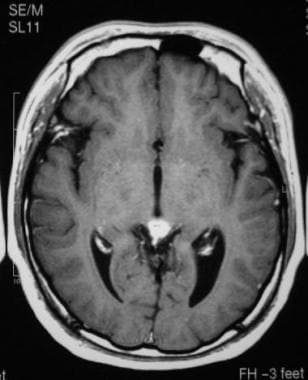
 Pineal germinoma in a 30-year-old man. Axial T1-weighted contrast-enhanced image shows an enhancing mass in the pineal region with bilateral extension into the posterior thalami.
Pineal germinoma in a 30-year-old man. Axial T1-weighted contrast-enhanced image shows an enhancing mass in the pineal region with bilateral extension into the posterior thalami.
 Pineal germinoma in a 30-year-old man. After radiation treatment, axial T2-weighted MRI shows high signal intensity in the pineal region.
Pineal germinoma in a 30-year-old man. After radiation treatment, axial T2-weighted MRI shows high signal intensity in the pineal region.
 Pineal germinoma in a 30-year-old man. After radiation treatment, axial T1-weighted contrast-enhanced MRI shows no enhancing tumor.
Pineal germinoma in a 30-year-old man. After radiation treatment, axial T1-weighted contrast-enhanced MRI shows no enhancing tumor.
 Pineal germinoma in a 30-year-old man. After radiation therapy, sagittal T1-weighted contrast-enhanced MRI shows no abnormal enhancing tumor.
Pineal germinoma in a 30-year-old man. After radiation therapy, sagittal T1-weighted contrast-enhanced MRI shows no abnormal enhancing tumor.
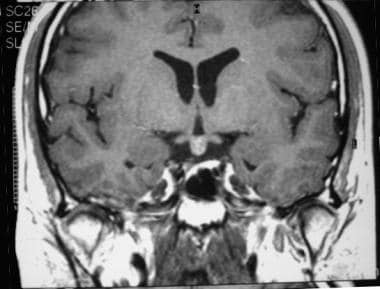 Coronal, post-contrast T1-weighted image shows a small enhancing mass in the region of the pituitary infundibulum in the suprasellar cistern.
Coronal, post-contrast T1-weighted image shows a small enhancing mass in the region of the pituitary infundibulum in the suprasellar cistern.
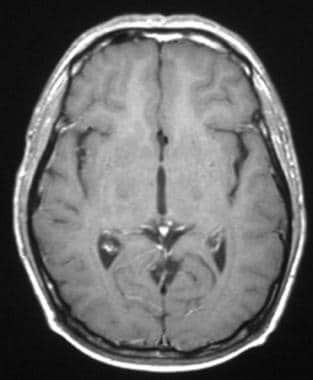
 Axial, post-contrast T1 weighted image shows an enhancing mass in the pineal region.
Axial, post-contrast T1 weighted image shows an enhancing mass in the pineal region.
-
Pineal germinoma in a 19-year-old man. Axial T1-weighted MRI shows an isointense lesion in the pineal region.
-
Pineal germinoma in a 19-year-old man. Axial T2-weighted MRI shows an isointense mass in the pineal region.
-
Pineal germinoma in a 19-year-old man. Axial T1-weighted contrast-enhanced MRI shows a homogeneously enhancing mass in the pineal region.
-
Pineal germinoma in a 19-year-old man. Sagittal T1-weighted contrast-enhanced MRI shows an enhancing mass in the pineal region. Compression of the quadrigeminal plate and aqueduct is shown.
-
Pineal germinoma in a 30-year-old man. Axial T2-weighted MRI shows a mildly hyperintense lesion involving the pineal region.
-
Pineal germinoma in a 30-year-old man. Sagittal T1-weighted contrast-enhanced image shows an enhancing mass in the pineal region.
-
Pineal germinoma in a 30-year-old man. Axial T1-weighted contrast-enhanced image shows an enhancing mass in the pineal region with bilateral extension into the posterior thalami.
-
Pineal germinoma in a 30-year-old man. After radiation treatment, axial T2-weighted MRI shows high signal intensity in the pineal region.
-
Pineal germinoma in a 30-year-old man. After radiation treatment, axial T1-weighted contrast-enhanced MRI shows no enhancing tumor.
-
Pineal germinoma in a 30-year-old man. After radiation therapy, sagittal T1-weighted contrast-enhanced MRI shows no abnormal enhancing tumor.
-
Axial, post-contrast CT shows an enhancing mass in the pineal region, which engulfs a calcified pineal gland
-
Coronal, post-contrast T1-weighted image shows a small enhancing mass in the region of the pituitary infundibulum in the suprasellar cistern.
-
Axial, post-contrast T1 weighted image shows an enhancing mass in the pineal region.









