Practice Essentials
Pelvic insufficiency fracture is type of stress fracture. The other subtype is fatigue fracture. Insufficiency fracture is caused by normal or physiologic stress upon weakened bone. Loss of bone trabeculae decreases the bone's elastic resistance. [1, 2, 3, 4, 5, 6, 7] Causes include osteoporosis, prolonged use of corticosteroids, chronic diseases such as diabetes and renal failure, and previous radiotherapy. Pelvic insufficiency fracture (PIF) associated with radiation therapy for gynecologic cancers is high (14%); most of these fractures occur in the sacral bone or joint (73.6%). [8] In a study by Jorgensen et al, preoperative chemoradiotherapy for rectal cancer was associated with a 14-fold higher risk of pelvic insufficiency fractures after 3 years, and female gender and age greater than 65 years each tripled the risk of pelvic insufficiency fractures. [9] Iliac wing fractures are often associated with sacral insufficiency in patients with osteoporosis.
Pelvic fracture is a disruption of the bony structures of the pelvis, including pelvic ring fractures, acetabular fractures, and avulsion fractures. The bony pelvis consists of the ilium, ischium, and pubis, which form an anatomic ring with the sacrum.
Iliac bone insufficiency fractures may be missed on CT and MRI but identified on radioisotope bone scans. [10] Other sites frequently affected by insufficiency fractures are the thoracic vertebra, tibia, fibula, and calcaneus. [11, 12, 13, 1, 14] The frequency of undetected sacral fractures in the elderly is high becaue of vague presenting symptoms and inadequate standard lumbosacral. imaging [15]
Bone scintigraphy and MRI are the imaging modalities of choice for insufficiency fractures of the pelvis. [16, 17, 18, 19, 20, 21, 22, 23, 24, 25] Bone scintigraphy is highly sensitive, but it relies on accurate interpretation of the uptake pattern, and atypical uptake patterns may be difficult to interpret. Abnormal uptake may persist for several months. Pelvic insufficiency fractures are frequently diagnosed on technetium-99m methylene diphosphonate bone scan. [26] MRI is sensitive for the detection of fractures, soft tissue edema, and marrow changes and may be better at demonstrating alternative diagnoses than bone scintigraphy or CT scanning. [27, 28, 29]
Cabarrus et al compared the sensitivities of CT scanning and MRI in detecting pelvic insufficiency fractures and found MRI to be substantially better in detecting such fractures. In patients undergoing both imaging modalities, 128 of 129 (99%) of fractures were detected by MRI, whereas only 89 of 129 fractures (69%) were detected by CT. [24]
CT provides further definition of the fracture, especially if MRI is unavailable or bone scintigraphy is inconclusive. CT scanning may not accurately detect fractures oriented transversely.
Failure to recognize insufficiency fractures of the pelvis may result in an incorrect diagnosis of malignancy. This may occur when areas of increased uptake are seen on bone scan or when marrow signal changes of the pelvis are observed on MRI, especially in patients who have undergone pelvic irradiation for gynecologic malignancies. [2] Care should be taken to recognize the bone scan uptake pattern, particularly atypical patterns; on MRI, altered bone marrow signal in the sacrum is cause for suspicion.
(See the images below.)
 Anteroposterior radiograph of the pelvis demonstrates areas of sclerosis in both sacral alae. Parasymphyseal fractures oriented vertically are seen as linear areas of osteolysis and adjacent sclerosis (arrows). Insufficiency fractures subsequently were confirmed on bone scans and CT.
Anteroposterior radiograph of the pelvis demonstrates areas of sclerosis in both sacral alae. Parasymphyseal fractures oriented vertically are seen as linear areas of osteolysis and adjacent sclerosis (arrows). Insufficiency fractures subsequently were confirmed on bone scans and CT.
 Axial CT of the sacrum reveals fractures (arrows) in both sacral alae. Note the sclerosis of the adjacent bone.
Axial CT of the sacrum reveals fractures (arrows) in both sacral alae. Note the sclerosis of the adjacent bone.
 Axial CT of the pubis reveals insufficiency fractures (arrows) in both parasymphyseal regions. Total hip replacement is an additional predisposing causative factor.
Axial CT of the pubis reveals insufficiency fractures (arrows) in both parasymphyseal regions. Total hip replacement is an additional predisposing causative factor.
Radiography
Radiographic findings of pelvic insufficiency fracture depend on the site of the fracture. Parasymphyseal and pubic ramus fractures may have an aggressive appearance, depending on the stage of fracture maturity. Findings include sclerosis, lytic fracture line, bone expansion, exuberant callus, and osteolysis, although a lytic fracture line or cortical break rarely is observed. The most common finding is a sclerotic band or line. The degree of confidence is low. Sacral fractures are difficult to detect because of osteoporosis, overlying bowel gas, and calcified vessels. Parasymphyseal and pubic ramus fractures often are mistaken for malignant lesions. Sacral, iliac, and supra-acetabular fractures often are difficult to detect.
(See the image below.)
Anteroposterior radiograph of the pelvis demonstrates areas of sclerosis in both sacral alae. Parasymphyseal fractures oriented vertically are seen as linear areas of osteolysis and adjacent sclerosis (arrows). Insufficiency fractures subsequently were confirmed on bone scans and CT.
Computed Tomography
CT findings may be definitive for the diagnosis of insufficiency fractures of the pelvis. CT is specific and is useful as an alternative to MRI or bone scintigraphy when radiographs are inconclusive. On CT scans, sacral fractures typically are oriented vertically and are located parallel to the sacroiliac joints. [30] (See the image below.)
Axial CT of the sacrum reveals fractures (arrows) in both sacral alae. Note the sclerosis of the adjacent bone.
A linear fracture line with surrounding sclerosis is observed, and pubic fractures are seen as a lytic fracture line often surrounded by callus. (See the images below.)
 Coronal CT of the sacrum demonstrates fractures (arrows) in both sacral alae. These fractures are oriented parallel to the sacroiliac joints. Note the prominent adjacent sclerosis.
Axial CT of the pubis reveals insufficiency fractures (arrows) in both parasymphyseal regions. Total hip replacement is an additional predisposing causative factor.
Coronal CT of the sacrum demonstrates fractures (arrows) in both sacral alae. These fractures are oriented parallel to the sacroiliac joints. Note the prominent adjacent sclerosis.
Axial CT of the pubis reveals insufficiency fractures (arrows) in both parasymphyseal regions. Total hip replacement is an additional predisposing causative factor.
Typically, a soft tissue mass is absent, bone destruction is lacking, and adjacent fascial planes are preserved. CT also is useful for detecting large bony sacral defects, such as Tarlov cysts (see the image below) and for the diagnosis of coexisting malignant lesions.
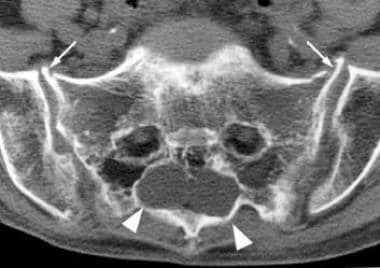 Axial CT of the sacrum reveals 2 large Tarlov cysts (arrowheads) in the sacrum. The sacral insufficiency fractures produce anterior cortical breaks (arrows).
Axial CT of the sacrum reveals 2 large Tarlov cysts (arrowheads) in the sacrum. The sacral insufficiency fractures produce anterior cortical breaks (arrows).
Magnetic Resonance Imaging
MRI is highly sensitive and highly specific. However, it cannot be used in patients with pacemakers, which is a significant limitation in the elderly population. MRI shows decreased signal on T1-weighted images and increased signal on T2-weighted images. In the sacrum, signal changes are seen as linear bands within the sacral ala and body; such bands are parallel to the sacroiliac joints. [30] (See the image below.)
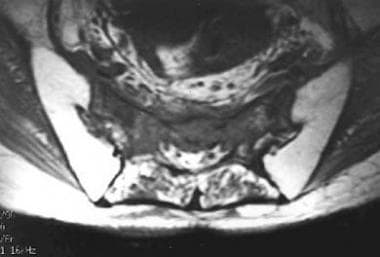 Axial T1-weighted MRI of the sacrum demonstrates decreased signal in the body and both alae of the sacrum. Bilateral sacral insufficiency fractures were confirmed by CT.
Axial T1-weighted MRI of the sacrum demonstrates decreased signal in the body and both alae of the sacrum. Bilateral sacral insufficiency fractures were confirmed by CT.
On T2-weighted images, the fracture line may be seen if it is surrounded by adjacent marrow edema. (See the images below.)
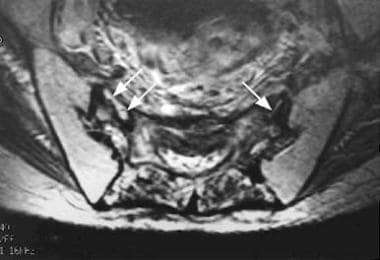 Axial T2-weighted MRI of the sacrum demonstrates linear bands of decreased signal in both sacral alae, parallel to the sacroiliac joints. Traces of fluid are observed within the fractures (small arrows). Adjacent edema is seen as areas of increased signal. Bilateral sacral insufficiency fractures were subsequently confirmed by CT.
Axial T2-weighted MRI of the sacrum demonstrates linear bands of decreased signal in both sacral alae, parallel to the sacroiliac joints. Traces of fluid are observed within the fractures (small arrows). Adjacent edema is seen as areas of increased signal. Bilateral sacral insufficiency fractures were subsequently confirmed by CT.
 Axial CT of the sacrum reveals insufficiency fractures in both sacral alae and the sacral body (arrows).
Axial CT of the sacrum reveals insufficiency fractures in both sacral alae and the sacral body (arrows).
Nuclear Imaging
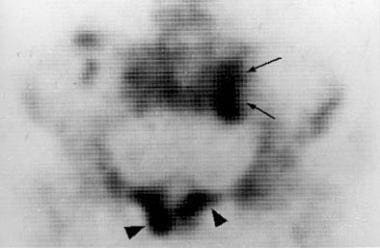
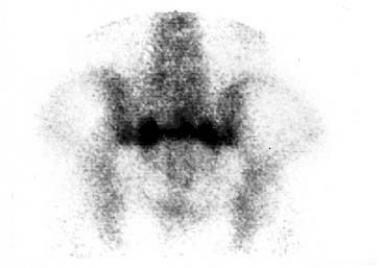
In nuclear studies, the typical H-shaped or butterfly pattern of uptake in the sacrum is diagnostic of insufficiency fracture (see the image below). The vertical limbs of the H lie within the sacral ala, parallel to the sacroiliac joints; the transverse limb of the H extends across the sacral body. The degree of confidence may be high. Nuclear studies are highly sensitive and highly specific when a typical pattern of sacral uptake or concomitant sacral and pubic uptake is observed. Pelvic insufficiency fractures are frequently diagnosed on technetium-99m methylene diphosphonate bone scan. [26, 30] If a typical pattern of abnormality is not present, the bone scan is much less specific. For variant or incomplete patterns of uptake, the findings may be mistaken as signifying malignancy or other diseases. CT or MRI is useful in such cases. [27, 26]
 Bone scan of the pelvis reveals a butterfly-shaped area of uptake in the sacrum (arrows). Focal uptake in the pubis (arrowhead) corresponds to an associated parasymphyseal insufficiency fracture.
Bone scan of the pelvis reveals a butterfly-shaped area of uptake in the sacrum (arrows). Focal uptake in the pubis (arrowhead) corresponds to an associated parasymphyseal insufficiency fracture.
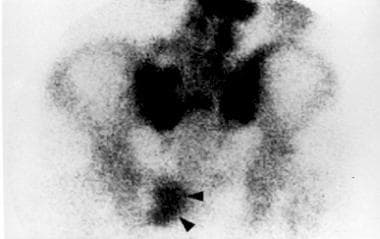
Other sacral variant uptake patterns occur frequently and include the unilateral ala, incomplete H, and horizontal linear dot patterns. (See the images below.)
 Bone scan of the pelvis reveals an incomplete (or partial) H-shaped area of uptake in the sacrum (arrows). Bilateral parasymphyseal insufficiency fractures (arrowheads) are present.
Bone scan of the pelvis reveals an incomplete (or partial) H-shaped area of uptake in the sacrum (arrows). Bilateral parasymphyseal insufficiency fractures (arrowheads) are present.
 Bone scan of the pelvis demonstrates a horizontal linear dot pattern of uptake in the sacrum.
Bone scan of the pelvis demonstrates a horizontal linear dot pattern of uptake in the sacrum.
Iliac fractures are seen as linear areas of uptake, while pubic and supra-acetabular fractures produce areas of linear or focal uptake.
Concomitant findings of 2 or more areas of uptake in the sacrum and at another pelvic site are considered diagnostic of insufficiency fractures of the pelvis. (See the image below.)
 Bone scan of the pelvis demonstrates a linear area of uptake in the pubis (arrowheads). A concomitant H-shaped insufficiency fracture of the sacrum is observed.
Bone scan of the pelvis demonstrates a linear area of uptake in the pubis (arrowheads). A concomitant H-shaped insufficiency fracture of the sacrum is observed.
-
Anteroposterior radiograph of the pelvis demonstrates areas of sclerosis in both sacral alae. Parasymphyseal fractures oriented vertically are seen as linear areas of osteolysis and adjacent sclerosis (arrows). Insufficiency fractures subsequently were confirmed on bone scans and CT.
-
Axial CT of the sacrum reveals fractures (arrows) in both sacral alae. Note the sclerosis of the adjacent bone.
-
Coronal CT of the sacrum demonstrates fractures (arrows) in both sacral alae. These fractures are oriented parallel to the sacroiliac joints. Note the prominent adjacent sclerosis.
-
Axial CT of the pubis reveals insufficiency fractures (arrows) in both parasymphyseal regions. Total hip replacement is an additional predisposing causative factor.
-
Axial CT of the sacrum reveals 2 large Tarlov cysts (arrowheads) in the sacrum. The sacral insufficiency fractures produce anterior cortical breaks (arrows).
-
Axial T1-weighted MRI of the sacrum demonstrates decreased signal in the body and both alae of the sacrum. Bilateral sacral insufficiency fractures were confirmed by CT.
-
Axial T2-weighted MRI of the sacrum demonstrates linear bands of decreased signal in both sacral alae, parallel to the sacroiliac joints. Traces of fluid are observed within the fractures (small arrows). Adjacent edema is seen as areas of increased signal. Bilateral sacral insufficiency fractures were subsequently confirmed by CT.
-
Axial CT of the sacrum reveals insufficiency fractures in both sacral alae and the sacral body (arrows).
-
Bone scan of the pelvis reveals a butterfly-shaped area of uptake in the sacrum (arrows). Focal uptake in the pubis (arrowhead) corresponds to an associated parasymphyseal insufficiency fracture.
-
Bone scan of the pelvis reveals an incomplete (or partial) H-shaped area of uptake in the sacrum (arrows). Bilateral parasymphyseal insufficiency fractures (arrowheads) are present.
-
Bone scan of the pelvis demonstrates a horizontal linear dot pattern of uptake in the sacrum.
-
Bone scan of the pelvis demonstrates a linear area of uptake in the pubis (arrowheads). A concomitant H-shaped insufficiency fracture of the sacrum is observed.









