Practice Essentials
A parathyroid adenoma is a benign tumor on a parathyroid gland. In primary hyperparathyroidism due to adenomas, the normal feedback on parathyroid hormone production by extracellular calcium seems to be lost, resulting in a change in the set point. However, this is not the case in primary hyperparathyroidism from parathyroid hyperplasia; an increase in the cell numbers is probably the cause. In approximately 85-90% of cases, primary hyperparathyroidism is caused by a single adenoma. In 10-15% of cases, multiple glands are involved (ie, either multiple adenomas or hyperplasia). [1, 2, 3, 4]
Primary hyperparathyroidism (HPT) is a condition characterized by an inappropriate excess of parathyroid hormone (PTH) secretion. The elevated PTH levels result in hypercalcemia and hypophosphatemia, with associated medical comorbidities including calculus formation, bone and abdominal pain, polyuria, and depression. An estimated 100,000 new cases occur per year in the United States, with a 2.5:1 female-to-male predominance. Primary HPT is caused by a single parathyroid adenoma in 90% of patients and multigland disease in approximately 10%. [4] Rarely, patients develop hyperparathyroidism secondary to a parathyroid carcinoma.
Imaging studies to detect parathyroid adenomas should be performed only after the diagnosis of primary HPT is established on the basis of biochemical findings. The diagnosis of primary hyperparathyroidism is made when hypercalcemia and elevated PTH levels are present. [1] National Institutes of Health (NIH) guidelines recommend parathyroidectomy in all symptomatic patients and asymptomatic patients younger than 50 years, [5] although some authors recommend more expansive criteria for surgical therapy. [6] Preoperative localization studies are increasingly becoming the standard of care, as they enable minimally invasive surgical techniques. Many surgeons advocate for 2 concurrent examinations to definitively identify the site of disease, and almost all authors advocate for intraoperative parathyroid hormone level monitoring. [7]
NICE (National Institute for Health and Care Excellence) recommends cervical US and suggests a second modality, such as MS, if additional guidance is needed for determining surgical approach. The American Association of Endocrine Surgeons (AAES) also recommend US, along with another imaging modality with high resolution for surgical planning. [1, 8, 9, 2]
Preoperative localization studies are also critical in patients with prior neck surgery or recurrent postoperative hypercalcemia. These patients can be particularly challenging for the imager because of distortion of normal anatomic landmarks and an increasing incidence of ectopic adenomas.
Noninvasive parathyroid imaging studies include technetium (Tc)-99m sestamibi scintigraphy, ultrasound, computed tomography (CT) scanning, magnetic resonance imaging (MRI), and positron emission tomography (PET) scanning. Tc-99m sestamibi is considered the most sensitive and specific imaging modality, particularly when used with single-photon emission CT (SPECT). PET with or without simultaneous CT scan (PET/CT) can be used but is an expensive imaging modality. [1, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19]
Although more common in the past, invasive procedures such as parathyroid selective arteriography and/or selective parathyroid venous sampling are now rarely performed. Level III evidence suggests a role for preoperative imaging before minimally invasive parathyroidectomy. Ultrasonography and nuclear scintigraphy both have level II evidence as a first-line examination. [20] The authors advocate parathyroid ultrasonography as a first-line test given the lack of ionizing radiation, low cost, and ease of use. Confirmatory testing with nuclear scintigraphy or, increasingly, multiphase CT, is often obtained if surgery is considered. [20]
Computed Tomography
Multiphase CT has become the standard of care for diagnostically confounding cases or, at some institutions, for first-line preoperative localization given the high accuracy. The “4D-CT” scan was originally described using 4 separate images phases, 1 noncontrast and 3 post contrast. [11, 18, 19] The authors recommend using a 3-phase technique to reduce the radiation dose. The first noncontrast images can be helpful to distinguish adenomas from the intrinsically dense iodine-rich thyroid gland, while the early and delayed postcontrast images highlight the hypervascular nature of adenomas and their characteristic early washout.
CT acquisition involves intravenous administration of nonionic iodinated contrast at a dose of 2 mL per kg of patient weight to a maximum of 120 mL. An intravenous infusion rate of 4 mL per second via an 18-gauge catheter works well for enhancement conspicuity. The authors recommend a 3-phase 4D-CT protocol with helical acquisition at 1.25-mm slice thickness from the bottom of the mandibular teeth down to the carina with noncontrast, early postcontrast, and delayed postcontrast imaging. A helical postcontrast sequence can be obtained 25 seconds after the start of intravenous contrast administration. Following a subsequent 30-second delay, a delayed-phase sequence can be acquired. [21]
Prior to the intravenous administration of contrast material, parathyroid adenomas demonstrate attenuation similar to that of muscle. Parathyroid adenomas tend to be hypervascular structures with variable contrast enhancement and early washout. A hypervascular soft-tissue mass near the expected location of the parathyroid glands is considered to represent a parathyroid adenoma. Ectopic glands may be seen, most commonly within the mediastinum. [22] A 4D-CT study is illustrated below with the characteristic hypodensity relative to normal thyroid, early avid enhancement, and washout.
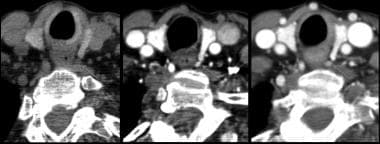 Axial CT images in noncontrast (A) early post-contrast (B) and delayed post-contrast (C) phases demonstrate a subtle left tracheoesophageal groove lesion with characteristic early enhancement and washout. This case illustrates the sensitivity of 4D-CT for small adenomas.
Axial CT images in noncontrast (A) early post-contrast (B) and delayed post-contrast (C) phases demonstrate a subtle left tracheoesophageal groove lesion with characteristic early enhancement and washout. This case illustrates the sensitivity of 4D-CT for small adenomas.
Intrathyroidal lesions may be subtle; detection is greatly improved by a multiphase technique, as in the image below. 4D-CT is sensitive for small adenomas that may elude other imaging techniques.
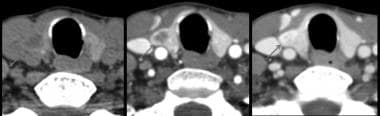 Axial CT images in noncontrast (A) early post-contrast (B) and delayed post-contrast (C) phases demonstrate an intrathyroidal lesion with subtle hypodensity on precontrast imaging and delayed enhancement. This enhancement pattern is seen less commonly than early enhancement and washout.
Axial CT images in noncontrast (A) early post-contrast (B) and delayed post-contrast (C) phases demonstrate an intrathyroidal lesion with subtle hypodensity on precontrast imaging and delayed enhancement. This enhancement pattern is seen less commonly than early enhancement and washout.
A prominent feeding artery at the margin of a parathyroid adenoma (polar vessel), first described on ultrasound, may be seen in up to two thirds of parathyroid adenomas on high-quality 4D-CT studies. This finding can increase diagnostic confidence that a suspicious lesion is a parathyroid adenoma instead of a lymph node or thyroid nodule. [23]
4D-DCT is increasingly being used for preoperative parathyroid localization and, in some studies, has been shown to be associated with a reduced number of glands explored and increased use of minimally invasive parathyroid surgery. [11, 18, 19] In a study by Jategaonker et al, the sensitivity and specificity of 4D-CT was 90.4% and 100% respectively, versus 63% sensitivity and 93.7% specificity for nuclear imaging studies and 41% sensitivity and 95% specificity for ultrasound. [11]
CT is limited by the ionizing radiation required for the multiphase technique. However, newer dose-reduction techniques, including automatic tube current modulation, appear to be effective in reducing the radiation dose.
Most modern multiphase 4D-CT techniques report a sensitivity and specificity exceeding 90%. The 4D-CT scan appears superior to both ultrasound and nuclear studies in side-by-side comparisons, particularly when attempting to diagnose the precise site of disease before minimally invasive surgery. [24]
In a study by Mekel et al of 27 patients who underwent parathyroidectomy for primary hyperthyroidism, 4D-CT identified a single adenoma in 26 patients, in whom a parathyroid adenoma was confirmed in surgery. Sensitivity was 81.4% and positive predictive value was 100% for 4D-CT in this study. [25]
False-negative findings result from small or ectopic parathyroid glands, poor visualization of neck structures as a result of streak artifact or distorted neck anatomy due to prior surgery, and misinterpretation of a parathyroid adenoma for a thyroid nodule. Multigland disease, including 4-gland hyperplasia, can be particularly challenging to diagnose, even with modern CT technique.
Magnetic Resonance Imaging
A typical MRI protocol for detecting parathyroid adenoma involves the acquisition of images through the neck and mediastinum. Axial, coronal, and sagittal views are typically acquired. A surface neck coil is used to image the neck and a chest coil for the mediastinum.
Images are obtained from the hyoid bone to the lung apices by using T1- and T2-weighted spin-echo sequences. T2 acquisitions are typically fat-suppressed to increase conspicuity of the glands, with short tau inversion recovery (STIR), frequency-selective fat saturation, or DIXON-based fat-suppression techniques. A section thickness of 3 mm is typically acquired, with minimal intersection gap. Postcontrast T1 imaging is typically fat suppressed to increase enhancement conspicuity. [26]
MRI findings
Normal parathyroid glands usually are not seen on MRI. Parathyroid adenomas are identified as soft-tissue masses in the expected location of the parathyroid glands. They characteristically demonstrate low T1 signal, avid enhancement, and high T2 signal. An axial STIR image of a parathyroid adenoma showing the characteristic T2 hyperintensity is shown below.
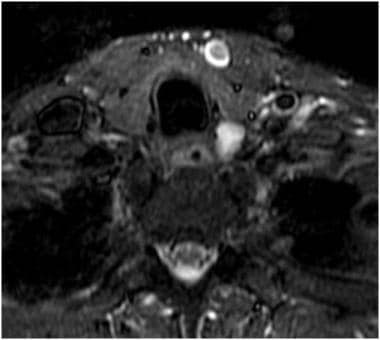 Axial STIR image showing a T2 hyperintense lesion in the left tracheoesophageal groove representing a parathyroid adenoma at surgery.
Axial STIR image showing a T2 hyperintense lesion in the left tracheoesophageal groove representing a parathyroid adenoma at surgery.
As many as 30% of abnormal parathyroid glands do not have typical MRI signal intensity characteristics. Atypical patterns include high signal intensity on T1-weighted images and low-to-medium signal intensity on T2-weighted images, low signal intensity on both T1- and T2-weighted images, and high signal intensity on both T1- and T2-weighted images. Low signal intensity on both T1- and T2-weighted images reflects cellular degenerative changes, old hemorrhage with hemosiderin-laden macrophages, and fibrosis in the abnormal gland. High signal intensity on both T1- and T2-weighted images has been associated with hemorrhage without significant degenerative or fibrotic changes. [27]
Fat suppression can be problematic in the neck, requiring special attention to technique. There are little data supporting advanced MR techniques such as MR perfusion or dynamic contrast enhanced imaging.
Sensitivity for MRI ranges appears significantly lower than that for CT—in the 70% range. However, MRI appears especially useful in detecting ectopic mediastinal glands, with sensitivities exceeding 80%. [28]
False-positive findings are reported to result from the misidentification of the following as parathyroid adenomas: enlarged lymph nodes, thyroid nodules (adenomas and/or exophytic colloid cysts), enlarged cervical ganglia, and other neck masses such as sarcoid nodules and neurofibromas. Enlarged lymph nodes have signal intensity characteristics similar to those of abnormal parathyroid glands. Abnormal parathyroid glands are expected to be medial to the carotid sheath, whereas lymph nodes are most frequently situated around or lateral to the sheath.
False-negative findings most commonly result from small parathyroid glands. The mean volume of detected abnormal glands has been reported as 3.5 cm3, while the mean volume of missed glands is 1.4 cm3. [27] Other reported false-negative findings result from concomitant thyroid disease, anatomic distortion due to prior surgery, ectopic glands (especially intrathyroidal glands), and atypical signal intensity characteristics.
In a study of 11 patients with parathyroid adenoma in whom 4D-MRI was used, parathyroid adenomas were identified in 10 patients. In 9 patients, there was an exact match as compared to ultrasound and sestamibi scan (MIBI). Sensitivity of 4D-MRI was 90% (100% after optimization), and specificity was 100%. [29]
Ultrasonography
The use of high-frequency 12- or 15-MHz transducers has become the standard for interrogating the parathyroid glands. The patient should be supine with his or her neck hyperextended. The examination should proceed from the carotid bifurcation superiorly to the sternal notch inferiorly and the carotid artery/internal jugular vein laterally. [30, 31]
NICE (National Institute for Health and Care Excellence) recommends cervical US and suggests a second modality, such as MS, if additional guidance is needed for determining surgical approach. The American Association of Endocrine Surgeons (AAES) also recommend US, along with another imaging modality with high resolution for surgical planning. [1, 8, 9, 2]
Normal-sized parathyroid glands are usually not visualized with ultrasound. On gray-scale images, parathyroid adenomas appear as a discrete, oval, anechoic or hypoechoic masses located posterior to the thyroid gland, anterior to the longus colli muscles, and, frequently, medial to the common carotid artery.
An echogenic line that separates the thyroid gland from the enlarged parathyroid gland can usually be seen. [32] Larger adenomas are more likely to have cystic change, lobulations, increased echogenicity due to fatty deposition, and occasional calcifications. [33]
Color Doppler ultrasound has been used to localize enlarged parathyroid glands. Parathyroid adenomas tend to be hypervascular lesions. An extrathyroidal artery may lead to a parathyroid adenoma in up to 83% of patients. [34] An extrathyroidal feeding vessel may provide a roadmap to an otherwise inconspicuous gland. Characteristically, the extrathyroidal artery enters at one pole of the gland (polar artery—a finding that can occasionally be appreciated on 4D-CT as well). (See the image below.) However, color Doppler sonograms of parathyroid adenomas may not show increased vascularity until the lesions are 1 cm in size.
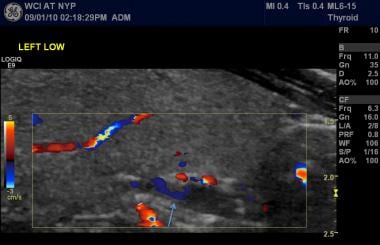 Ultrasound imaging with color Doppler interrogation showing a hypoechoic lesion posterior to the thyroid gland with a polar vessel sign (arrow).
Ultrasound imaging with color Doppler interrogation showing a hypoechoic lesion posterior to the thyroid gland with a polar vessel sign (arrow).
The sensitivity of ultrasound in detecting parathyroid adenomas has been reported from 55 to 83%. Ultrasound is especially limited in the mediastinum because of a poor or absent acoustic window. The specificity of ultrasound in detecting parathyroid adenomas ranges from 40 to 98%.
In a study of 146 patients with parathyroid adenoma (88% single gland, 7% multigland, and 5% negative explorations) by Touska et al, the sensitivity and specificity of SPECT/CT-guided ultrasound were 83% and 96%, respectively, with sensitivity being higher for single gland (87%) than multigland disease (70%). [14]
False-positive findings result when thyroid nodules, enlarged lymph nodes, the esophagus, longus colli muscles, and perithyroid veins are mistaken for enlarged parathyroid glands.
False-negative studies result from small parathyroid glands; ectopic locations lacking an adequate acoustic window; and poor visualization of neck structures due to previous surgery, thyromegaly, or body habitus. [31]
Localization of adenomas in the mediastinum is limited because of the lack of an acoustic window and the difficulty in visualizing structures posterior to the air-filled trachea and esophagus. If an intrathyroidal lesion is detected, the lesion cannot confidently be differentiated as a parathyroid adenoma or thyroid nodule. Aspiration biopsy is required.
Nuclear Imaging
Radiopharmaceutical agents
Nuclear medicine imaging of the parathyroid glands was introduced in the late 1970s using thallium-201 (201Tl) as an imaging agent. Subsequently, the 201Tl–technetium-99m (99mTc)-pertechnetate (thallium-pertechnetate) subtraction method was described, which became the first widely accepted method for radionuclide imaging of the parathyroid glands. [35]
Thyroid tissue takes up both 201Tl and 99mTc-pertechnetate. Abnormal parathyroid tissue, such as parathyroid adenomas, hyperplastic parathyroid glands, and parathyroid carcinoma, takes up 201Tl but not 99mTc-pertechnetate. Separate 201Tl and 99mTc-pertechnetate images are obtained in a single session without moving the patient, and a subtraction image is generated. An example of a dual-tracer acquisition with 99mTc-pertechnetate and 99mTc sestamibi is shown below.
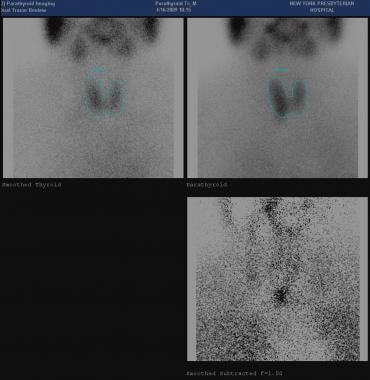 Planar acquisition from dual-tracer 99mTc pertechnetate (upper left) and 99mTc sestamibi (upper right) imaging protocol showing subtracted image (lower right) with a right lower pole parathyroid adenoma.
Planar acquisition from dual-tracer 99mTc pertechnetate (upper left) and 99mTc sestamibi (upper right) imaging protocol showing subtracted image (lower right) with a right lower pole parathyroid adenoma.
In the 1990s, 99mTc sestamibi was introduced for parathyroid imaging for both subtraction and single-agent, dual-phase technique. [36] 99mTc tetrofosmin was subsequently discovered to have imaging characteristics similar to 99mTc sestamibi. The discussion focusd on 99mTc sestamibi and 99mTc tetrofosmin, which have largely supplanted thallium in modern imaging protocols. [16, 17]
Technetium-99m sestamibi imaging and t echnetium-99m tetrofosmin imaging
Technetium-99m sestamibi is taken up by both thyroid tissue and abnormal parathyroid tissue. [16, 17] A dual-phase single-agent technique is based on the differential washout of 99mTc sestamibi from thyroid tissue compared to abnormal parathyroid tissue. The rate of washout from abnormal parathyroid tissue, such as parathyroid adenoma, is much slower than that of normal thyroid tissue.
One significant difference between 99mTc tetrofosmin and 99mTc sestamibi is the differential washout of the radiotracer from the thyroid gland. The thyroid washout rates are slower for 99mTc tetrofosmin than for 99mTc sestamibi. [37]
A typical protocol involves the intravenous injection of 20-25 mCi of 99mTc sestamibi or 99mTc tetrofosmin, followed by the acquisition of early and delayed images of the neck and upper thorax and/or mediastinum. The initial early image is obtained 10-15 minutes after the injection, and delayed imaging is obtained 1.5-3 hours after the injection. Single-photon emission CT (SPECT) imaging can be performed for improved anatomic localization. [38, 13, 14] A typical protocol for dual-phase scintigraphy with 99mTc sestamibi or 99mTc tetrofosmin follows [39] :
-
Examine the patient's neck for palpable thyroid or other neck masses.
-
Place the patient in a supine position with his or her neck hyperextended under the gamma camera.
-
Set energy windows to 140 keV ± 28.
-
Intravenously inject 20-25 mCi of 99mTc sestamibi or 99mTc tetrofosmin.
-
Use a camera with a large field of view and a high-resolution collimator.
-
Obtain anterior images of the neck and upper thorax and/or mediastinum. Image acquisition time is 10 minutes.
-
Obtain early thyroid-phase images 10-15 minutes after the injection.
-
Obtain delayed parathyroid-phase images 1.5-3 hours after the injection.
Optional imaging procedures include the following:
-
Right and left anterior oblique views can be obtained.
-
If nodules are palpable, delayed images can be obtained after 5-6 hours.
-
99mTc pertechnetate can be injected after delayed imaging.
-
Sodium iodide I-123 images may be obtained in a second examination on the next day.
-
SPECT can be performed for improved anatomic localization.
The agent may also be injected prior to minimally invasive parathyroid surgery on an outpatient basis, and a hand-held gamma probe can be used intraoperatively to guide the incision and localize the abnormal gland.
The sensitivity of the 99mTc sestamibi or 99mTc tetrofosmin techniques in detecting parathyroid adenomas has been reported ranging from 70 to 100%. Early SPECT imaging has a reported sensitivity of 91-96%.
In a study of 146 patients with parathyroid adenoma (88% single gland, 7% multigland, and 5% negative explorations) by Touska et al, the sensitivity and specificity of SPECT/CT-guided ultrasound were 83% and 96%, respectively, with sensitivity being higher for single gland (87%) than multigland disease (70%). [14]
False-positive findings in 99mTc sestamibi and 99mTc tetrofosmin dual-phase imaging include uptake in coexisting thyroid nodules, which are interpreted as parathyroid adenomas. False-negative findings include parathyroid lesions, which are too small to be detected, and unusually rapid washout from a parathyroid adenoma.
(11)C-methionine positron emission tomography/computed tomography (Met-PET/CT), in a study by Lenschow et al, raised the rate of correctly localized single parathyroid adenomas in patients with negative cervical ultrasonography and MIBI-SPECT/CT and increased the number of focused surgical approaches. Cervical US localized a single parathyroid adenoma in 10 of 17 patients (59%), while MIBI-SPECT/CT identified 11 of 17 single adenomas (65%). In the remaining 6 patients, Met-PET/CT identified 5 single adenomas. This step-up approach correctly identified single adenomas in 16 od 17 patients (94%). [40]
Angiography
Invasive examinations, such as parathyroid arteriography and parathyroid venous sampling, can be considered when the findings of noninvasive imaging modalities are nondiagnostic.
Angiographic and perfusion characteristics of parathyroid adenomas were first described in the 1970s and were used to identify abnormal hypervascular glands with preoperative digital subtraction angiography. A characteristic “blush” has been described following the injection of intraarterial contrast, indicating the presence of an abnormal gland that is hypervascular compared with normal thyroid and parathyroid tissue. [41] Similar hypervascular and washout principles are applied to modern cross-sectional imaging interpretation.
Typically, the paired inferior thyroid arteries supply the parathyroid glands. However, parathyroid gland blood supply can also be derived from the superior thyroid arteries, small branches of the laryngeal and tracheoesophageal arteries, and, occasionally, a thyroidea ima artery. The superior thyroid arteries are branches of the external carotid arteries. The inferior thyroid arteries are branches of the thyrocervical trunk.
Digital subtraction angiography (DSA) and/or conventional arteriography can be used to localize a parathyroid adenoma. Selective arteriography of both thyrocervical trunks, both internal mammary arteries, and both common carotid arteries is recommended. [42] The thyrocervical trunks are examined to assess intrathyroid glands, juxtathyroid glands, and glands that have descended into the superior mediastinum in the tracheoesophageal groove.
For ectopic mediastinal or thymic glands, the internal mammary arteries can be studied. The common carotid arteries are injected to detect parathymic or juxtathyroid glands. Occasionally, arteriography of the aortic arch, and possibly the innominate artery, is performed to search for a thyroidea ima artery if findings from the aforementioned selective angiograms are negative.
The risks of parathyroid arteriography are stroke and spinal cord injury. Arteriography of the common carotid arteries and, especially, superselective catheterization of the superior thyroid arteries, often require extensive manipulation of the guidewires and catheters in the region of the carotid bifurcation.
Selective venous sampling and parathyroid hormone measurements are performed to determine the general location of a parathyroid adenoma. A parathyroid arteriogram should be performed first because this serves as a guide or road map to the more variable parathyroid venous pathway. [42] An end-hole catheter without side holes should be used to prevent the mixing of blood from adjacent veins. Sampling of small veins is the goal. Attempts should be made to sample the right and left thymic veins, inferior thyroid veins, and vertebral veins (if the middle and inferior thyroid veins were ligated in a previous operation). A peripheral vein sample is obtained, and a 2-fold gradient between the parathyroid hormone concentration in the sampled vein and that of the peripheral vein must be observed.
The sensitivity of DSA has been reported as 49% and that of parathyroid venous sampling ranges from 70-80%. [42]
-
Axial CT images in noncontrast (A) early post-contrast (B) and delayed post-contrast (C) phases demonstrate a subtle left tracheoesophageal groove lesion with characteristic early enhancement and washout. This case illustrates the sensitivity of 4D-CT for small adenomas.
-
Axial CT images in noncontrast (A) early post-contrast (B) and delayed post-contrast (C) phases demonstrate an intrathyroidal lesion with subtle hypodensity on precontrast imaging and delayed enhancement. This enhancement pattern is seen less commonly than early enhancement and washout.
-
Axial STIR image showing a T2 hyperintense lesion in the left tracheoesophageal groove representing a parathyroid adenoma at surgery.
-
Ultrasound imaging with color Doppler interrogation showing a hypoechoic lesion posterior to the thyroid gland with a polar vessel sign (arrow).
-
Planar acquisition from dual-tracer 99mTc pertechnetate (upper left) and 99mTc sestamibi (upper right) imaging protocol showing subtracted image (lower right) with a right lower pole parathyroid adenoma.






